Complications of septal surgeries
Reading File
Finding Sources
Finding Sources
Searching PubMed
septoplasty complications
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have comprehensive information from Cummings Otolaryngology and Scott-Brown's to compile a thorough answer.
Complications of Septal Surgeries
Septal surgeries include Submucous Resection (SMR), Septoplasty, and increasingly Extracorporeal Septoplasty / Septorhinoplasty. Complications are largely attributable to poor surgical planning or technique.
1. Intraoperative Complications
Hemorrhage
- Most common immediate complication. Mild oozing is expected, not a true complication.
- Significant bleeding is more likely when septoplasty is combined with inferior turbinate resection.
- Controlled with vasoconstrictors (lidocaine + epinephrine), bipolar cautery, or packing.
Mucosal Tears / Bilateral Fenestrations
- Unrepaired contiguous mucoperichondrial tears on both sides of the septum are a primary cause of septal perforation.
- Placing crushed cartilage back into the mucoperichondrial envelope at the end of the procedure creates a barrier against perforation development.
2. Early Postoperative Complications
Septal Hematoma
- Occurs when a quilting suture is not placed at closure, allowing blood to collect between the mucoperichondrial flaps.
- Presents with bilateral nasal obstruction and a boggy, bluish swelling on examination.
- Must be drained promptly - untreated hematoma leads to:
- Cartilage necrosis (avascular necrosis from pressure)
- Septal abscess
- Septal perforation
- Saddle nose deformity
Septal Abscess
- Secondary infection of an untreated or inadequately drained hematoma.
- Presents with nasal obstruction, pain, swelling, and fever.
- Leads to rapid cartilage destruction; requires urgent surgical drainage and antibiotics.
- Complications of septal abscess include perforation, saddle nose, and columellar retraction.
Infection / Rhinosinusitis
- True infection is rare after septoplasty.
- Rhinorrhea may persist for several months postoperatively and is not always indicative of infection.
3. Late / Long-term Complications
Septal Perforation
- Results from:
- Unrepaired bilateral (contiguous) mucoperichondrial tears
- Failure to re-skeletonize the mucoperichondrial envelope at completion of resection
- Avascular necrosis following untreated hematoma
- Manifests as whistling on inspiration, crusting, epistaxis, and persistent obstruction.
Saddle Nose Deformity
- Over-resection of the dorsal strut removes the structural support of the nasal bridge, causing collapse.
- Also results from cartilage destruction secondary to hematoma or abscess.
- Principle: always preserve an L-strut of at least 10-15 mm of dorsal and caudal cartilage.
Nasal Tip Ptosis / Columellar Retraction
- Caused by over-resection of the caudal septum, which provides tip projection and support.
- Loss of medial crural support leads to tip drooping and/or columellar retraction.
Nasal Dorsal Collapse / Inverted-V Deformity
- Occurs with loss of dorsal nasal support from aggressive resection.
Persistent Nasal Obstruction (Most Common Overall Complication)
- The single most frequent complaint after septoplasty.
- Often due to inadequate resection of the posterior bony spur - a common pitfall when only the anterior deviated cartilage is addressed with a swivel knife.
- The remaining posterior spur creates ongoing obstruction AND makes revision surgery technically harder (difficult anterior dissection due to scarring).
Synechiae (Adhesions)
- Fibrous bands form between the septum and the inferior turbinate or lateral nasal wall.
- More common with traumatic suturing technique, especially when straight septal needles are used.
- Cause nasal obstruction and are managed by division + placement of a silastic sheet spacer.
4. Sensory / Neurological Complications
Upper Dental Anesthesia / Numbness
- The nasopalatine nerve and anterior superior alveolar nerve can be stretched or damaged during dissection, causing numbness of the upper incisors and anterior palate.
- Usually transient; rarely permanent.
Tooth Discoloration
- Upper incisor teeth discoloration has been reported, attributed to nerve/vascular disruption to the teeth during septal surgery.
5. Aesthetic Complications
| Complication | Cause |
|---|---|
| Saddle nose / low dorsum | Over-resection of dorsal strut |
| Tip ptosis | Over-resection of caudal septum |
| Inverted-V deformity | Loss of middle vault support |
| Nasal base widening | Columellar retraction |
| Nose rigidity | Bone grafting techniques |
6. Special Considerations
SMR vs. Septoplasty
- SMR (classic Killian's operation) is less preferred today because it removes too much cartilage, risking saddle nose and tip ptosis. Septoplasty with conservative cartilage preservation is now standard.
- In pediatric patients, resection must be especially conservative to avoid disrupting endochondral ossification plates, which would impair nasal growth.
Revision Surgery
- Posterior septal spurs left untreated at primary surgery make revision dissection difficult due to anterior scarring.
- Revision septoplasty is technically harder and carries higher risk of perforation.
Sources:
- Cummings Otolaryngology Head and Neck Surgery (9780323612173), p. 582
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 (9781138094611), p. 1195
Complications of septal surgeries
Reading File
Finding Sources
Finding Sources
Searching PubMed
septoplasty complications
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
I have all the needed content from the primary sources. Here is the complete, well-organized answer.
Complications of Septal Surgeries
Septal surgeries include Submucous Resection (SMR), Septoplasty, and Septorhinoplasty. Complications are mostly attributable to poor surgical planning or operative technique.
1. Persistent Nasal Obstruction (Most Common)
The single most frequent complaint after septoplasty is persistence of the subjective symptom of nasal obstruction.
- Usually caused by inadequate resection of the posterior bony spur - a pitfall when only the anterior deviated cartilage is removed (e.g., with a swivel knife) without addressing the full septum including its posterior bony component.
- The residual spur causes ongoing obstruction, and the resulting anterior scarring makes revision septoplasty technically harder - the revision surgeon faces difficult dissection anteriorly to reach and address the posterior spur.
2. Hemorrhage
- Mild postoperative oozing is expected and is not a true complication in the early phase.
- Significant postoperative bleeding is more likely when septoplasty is combined with inferior turbinate resection.
- Controlled intraoperatively with vasoconstrictors (lidocaine + epinephrine), bipolar cautery, and nasal packing.
3. Septal Hematoma
- Occurs when a quilting (through-and-through) suture is not placed at closure, allowing blood to accumulate between the two mucoperichondrial flaps.
- Presents with bilateral nasal obstruction and a boggy, blue-red swelling of the septum.
- Must be drained urgently - untreated hematoma leads to:
- Avascular necrosis of septal cartilage (cartilage has no blood supply of its own; it depends entirely on the perichondrium)
- Septal abscess
- Septal perforation
- Saddle nose deformity
- Columellar retraction and nasal base widening
4. Septal Abscess
- Secondary infection of an incompletely drained or untreated hematoma.
- Presents with nasal obstruction, pain, fever, and a tender fluctuant swelling.
- Causative organisms: Streptococcus pneumoniae and group A beta-hemolytic streptococci.
- Leads rapidly to cartilage lysis and saddle nose deformity.
- Management: surgical drainage + nasal packing + systemic antibiotics.
- Note: In children under 2 years with septal abscess, child abuse should be considered.
5. Septal Perforation
Causes:
- Unrepaired bilateral (contiguous) mucoperichondrial tears on both sides of the septum at the same location - the most direct cause.
- Failure to re-skeletonize (replace crushed cartilage into) the mucoperichondrial envelope at the end of resection - the envelope without a cartilage scaffold is vulnerable.
- Avascular necrosis secondary to untreated hematoma.
- Over-tight internal nasal splints compressing the septal membrane.
Presentation: Whistling on inspiration, crusting, epistaxis, and paradoxical obstruction.
6. Structural / Aesthetic Deformities
These arise from over-resection of the septal framework:
| Complication | Mechanism |
|---|---|
| Saddle nose deformity | Over-resection of the dorsal strut removes nasal bridge support, causing collapse of the middle vault |
| Nasal tip ptosis | Over-resection of the caudal septum removes the major tip support mechanism |
| Columellar retraction | Loss of caudal septal support with retraction of the columella |
| Nasal base widening | Secondary to columellar retraction |
| Inverted-V deformity | Loss of middle vault support, leading to upper lateral cartilage collapse away from the nasal bones |
Key principle: A minimum L-strut of ~10-15 mm of both dorsal and caudal cartilage must be preserved to maintain structural integrity.
This is why surgery has moved away from aggressive SMR (Killian's operation, which removed large amounts of cartilage) toward conservative septoplasty with cartilage preservation and repositioning.
7. Synechiae (Adhesions)
- Fibrous bands between the septum and inferior turbinate or lateral nasal wall.
- More common with traumatic suturing technique, especially when straight septal needles are used instead of curved ones.
- Result in nasal obstruction; managed by division and placement of a silastic sheet spacer to prevent re-adhesion.
8. Infection / Rhinosinusitis
- True infection after septoplasty is rare.
- Rhinorrhea may persist for several months postoperatively - this is a side effect, not strictly a complication, and should be discussed with patients preoperatively.
9. Sensory / Neurological Complications
- Upper dental anesthesia / numbness of upper incisors - from stretch or injury to the nasopalatine nerve during dissection; usually transient, rarely permanent.
- Upper incisor tooth discoloration - reported from disruption of nerve and vascular supply to the teeth.
10. Aesthetic Changes from Nasal Valve Surgery
When septal surgery includes nasal valve repair:
- Rigidity of the nose can result from bone grafting techniques.
- Visible aesthetic changes to the nasal contour are an anticipated side effect that must be discussed with the patient preoperatively.
- When patients decline major nasal valve surgery due to aesthetic concerns, a combination of septal surgery, turbinate surgery, and minor nasal valve procedures can achieve comparable functional results with minimal visible change.
Summary Table
| Category | Complication |
|---|---|
| Most common | Persistent nasal obstruction |
| Hemorrhagic | Postoperative bleeding; more risk with turbinate surgery |
| Hematoma | Septal hematoma (missing quilting suture) |
| Infective | Septal abscess (from untreated hematoma) |
| Structural | Septal perforation, saddle nose, tip ptosis, columellar retraction, synechiae |
| Sensory | Upper dental numbness, tooth discoloration |
| Functional | Persistent obstruction from posterior spur; difficult revision surgery |
Sources:
- Cummings Otolaryngology Head and Neck Surgery, p. 582 - "Complications of Septoplasty"
- K.J. Lee's Essential Otolaryngology, p. 1011 - Septal hematoma and abscess
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1, p. 1195 - Complications of Septal Surgery
Modified wullstein classification
Reading File
Finding Sources
Finding Sources
Searching the Web
modified Wullstein classification tympanoplasty types
Reading File
Reading Web Page
https://entokey.com/ossiculoplasty-and-tympanoplasty-in-chro…
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive textbook content and the classic diagram. Here is the full answer.
Modified Wullstein Classification of Tympanoplasty
The Wullstein classification was originally proposed by Horst Ludwig Wullstein (1952) and classifies tympanoplasty operations into Types I-V based on the ossicular status found and the mechanism used to restore sound conduction to the oval window, with simultaneous round window protection.
The modified Wullstein classification - as used in modern otology (notably by Nadol, Schuknecht, and in Shambaugh's Surgery of the Ear) - refines Type III into subcategories and redefines Type V to reflect current surgical practice.
Classic Diagram (Shambaugh's Surgery of the Ear)
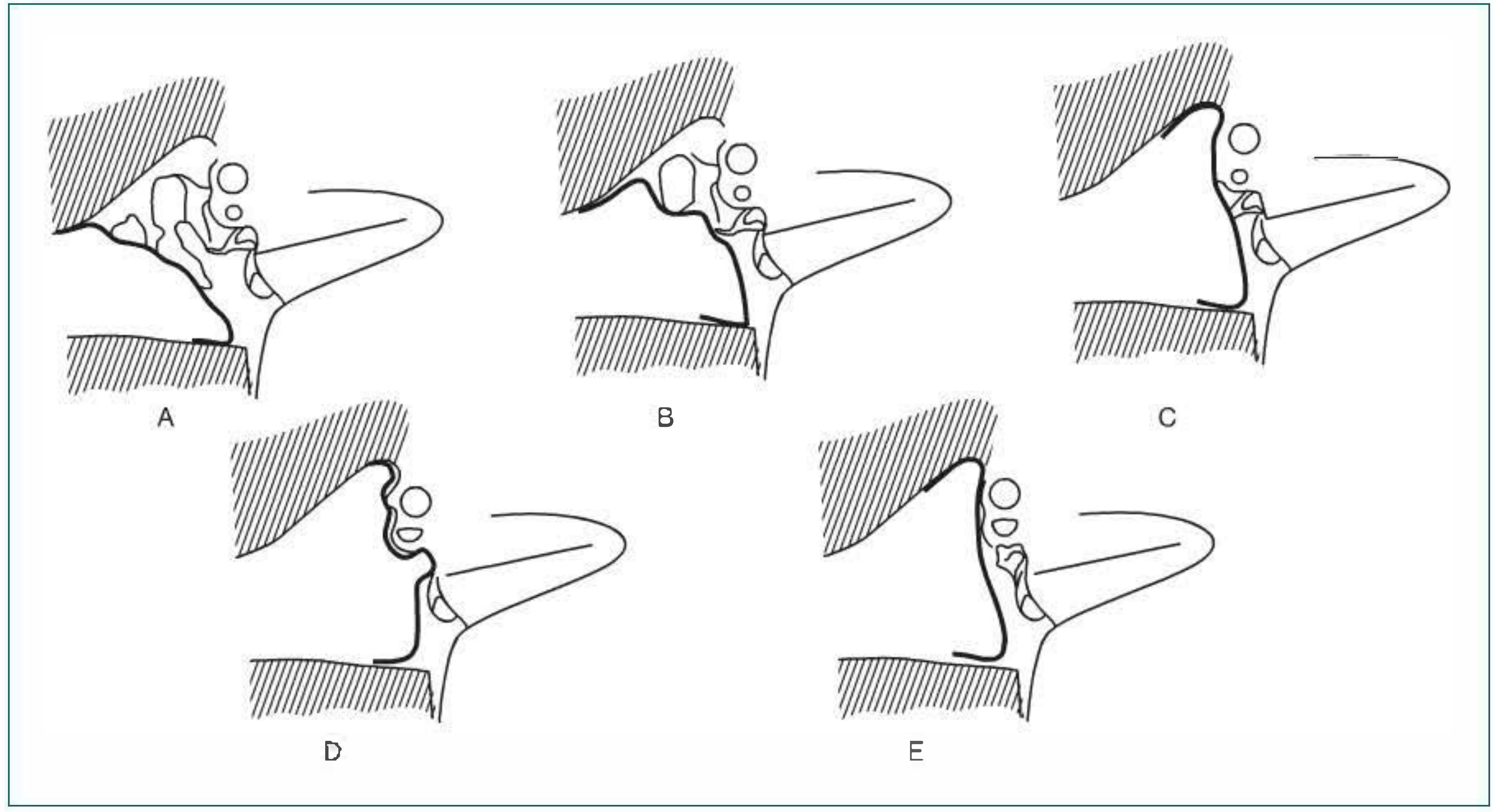
A = Type I, B = Type II, C = Type III (myringostapediopexy / columella effect), D = Type IV, E = Type V
Type I - Myringoplasty / Tympanoplasty
| Feature | Detail |
|---|---|
| Ossicular status | All ossicles intact and mobile |
| Problem | Tympanic membrane perforation only |
| Operation | Repair of the tympanic membrane (myringoplasty); middle ear explored to confirm normal ossicular chain |
| Sound pathway | Normal - TM → malleus → incus → stapes → oval window |
| Middle ear space | Restored to normal volume and geometry |
Distinction: Myringoplasty = repair of TM alone without middle ear exploration. Tympanoplasty Type I = repair + middle ear inspection confirming intact mobile ossicles.
Type II - Ossicular Reconstruction with Lever Mechanism Preserved
| Feature | Detail |
|---|---|
| Ossicular status | Partial erosion of malleus or incus (most commonly the lenticular process of the incus) |
| Operation | Repair of TM + restoration of ossicular continuity using bone graft, cartilage, or synthetic prosthesis |
| Sound pathway | Restored TM → repaired malleus-incus complex → stapes |
| Goal | Preserve the lever mechanism (ratio of TM area to stapes footplate area + ossicular lever arm) |
Not commonly performed in its original form today; most lenticular process erosions are now handled with PORP-type reconstructions (subsumed into Type III).
Type III - Columella Reconstruction (MOST COMMON)
The ossicular status here is: malleus and incus absent or non-functional, but stapes is present.
The modified classification subdivides Type III into three categories:
IIIa - Stapes Columella (Myringostapediopexy)
- TM graft is placed directly onto the stapes capitulum (head)
- No prosthesis used; the stapes itself acts as the columella
- Creates a shallow middle ear with a columella effect
- Requires an intact stapes superstructure
IIIb - Minor Columella (PORP)
- An ossicular or synthetic strut is placed between the stapes capitulum and the tympanic membrane / manubrium
- Uses a Partial Ossicular Replacement Prosthesis (PORP)
- Stapes superstructure must be intact
IIIc - Major Columella (TORP)
- Performed when the stapes crura are also missing - only the footplate remains
- A graft or prosthesis extends from the stapes footplate to the TM/manubrium
- Uses a Total Ossicular Replacement Prosthesis (TORP)
- A cartilage interposition graft is placed between the prosthesis head and the TM to prevent extrusion
Type IV - Cavum Minor / Round Window Protection
| Feature | Detail |
|---|---|
| Ossicular status | Only the mobile stapes footplate remains (no crura, no malleus, no incus) |
| Principle | The footplate is left directly exposed to incoming sound from the ear canal. A tissue graft acoustically shields the round window membrane from sound |
| Cavum minor | The small air space created between the acoustic shield and the round window - aerated by the Eustachian tube |
| Sound pathway | Sound → EAC → directly to exposed stapes footplate → oval window → cochlea. Round window is protected from direct sound (phase difference preserved) |
| Goal | Maintain the phase difference between oval and round window by shielding the round window |
This creates a "small middle ear" (cavum minor). Hearing results are modest but functional.
Type V - Fixed Stapes Footplate / Fenestration
| Feature | Detail |
|---|---|
| Ossicular status | Ankylosed (fixed) stapes footplate - oval window is non-functional |
| Goal | Bypass the fixed footplate by creating an alternative route for sound to reach the inner ear |
Va (Original Wullstein Type V) - Lateral Semicircular Canal Fenestration
- A new window (fenestra novovalis) is created in the lateral (horizontal) semicircular canal
- TM graft placed over this fenestra transmits sound directly to the perilymph
- Round window protected with tissue seal
- Rarely performed today; largely replaced by Type Vb and stapedectomy
Vb (Modified Type V) - Oval Window Stapedectomy / Footplate Removal
- The stapes footplate is removed and the oval window is sealed with a tissue graft
- Similar concept to a Type IV but adapted for a fixed footplate situation
- This is essentially the modern stapedectomy / stapedotomy approach
- Now the standard method; has supplanted Type Va
Summary Table
| Type | Ossicular Status | Procedure | Alternative Name |
|---|---|---|---|
| I | All ossicles intact & mobile | TM repair + middle ear exploration | Myringoplasty |
| II | Partial malleus/incus erosion | TM repair + restore continuity | Ossiculoplasty |
| IIIa | Malleus + incus absent; stapes intact | TM graft on stapes head | Myringostapediopexy |
| IIIb | Malleus + incus absent; stapes head present | PORP: stapes head to TM | Minor columella |
| IIIc | Malleus + incus + crura absent; footplate only | TORP: footplate to TM | Major columella |
| IV | Mobile footplate only | TM shields round window; footplate exposed | Cavum minor operation |
| Va | Fixed footplate | Lateral SCC fenestration covered by graft | Fenestration operation |
| Vb | Fixed footplate | Footplate removal + oval window graft | Stapedectomy / Stapedotomy |
Key Physiological Principle
All types are built on two concepts:
- Sound transformer function - restoring efficient sound conduction to the oval window
- Round window protection - ensuring the round window membrane does not receive the same sound pressure as the oval window simultaneously (which would cancel out the pressure differential needed for perilymph flow)
Sources:
- Shambaugh's Surgery of the Ear (9781607950264), pp. 490, Chapter 28-29 - Wullstein classification diagram and modified descriptions
- Ossiculoplasty and Tympanoplasty in Chronic Otitis Media (Ento Key / Cummings-affiliated source) - Modified Wullstein types with PORP/TORP taxonomy
TORP
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent images retrieved. Here is the complete account.
TORP - Total Ossicular Replacement Prosthesis
Definition
A TORP (Total Ossicular Replacement Prosthesis) is an alloplastic implant used in ossiculoplasty to restore sound conduction when the entire ossicular superstructure is absent - i.e., the malleus, incus, and stapes crura are all missing, leaving only the stapes footplate (mobile or fixed).
It bridges the gap between the stapes footplate and the tympanic membrane (TM), acting as a single column to transmit vibratory energy.
- PORP (Partial Ossicular Replacement Prosthesis) = used when stapes superstructure (head + crura) is intact - bridges stapes head to TM
- TORP = used when stapes superstructure is absent - bridges stapes footplate to TM
In Wullstein's classification, TORP placement corresponds to a Type IIIc (major columella) tympanoplasty.
Indications
- Chronic otitis media with total ossicular chain erosion/destruction
- Cholesteatoma with absent superstructure
- Traumatic ossicular disruption with absent crura
- Previous failed ossiculoplasty with complete ossicular loss
- Congenital ossicular anomalies
Anatomy of the TORP
A TORP has two main components:
| Component | Function |
|---|---|
| Footplate platform / base | Sits on the stapes footplate; transmits vibration into the oval window |
| Shaft / strut | Vertical column transmitting sound energy upward |
| Head plate | Upper surface that contacts the TM (via a cartilage interposition graft) |
Adjustable TORPs allow the shaft length to be modified intraoperatively to fit the exact middle ear dimensions. Fixed-length TORPs come in standard sizes and must be selected to match the measured distance.
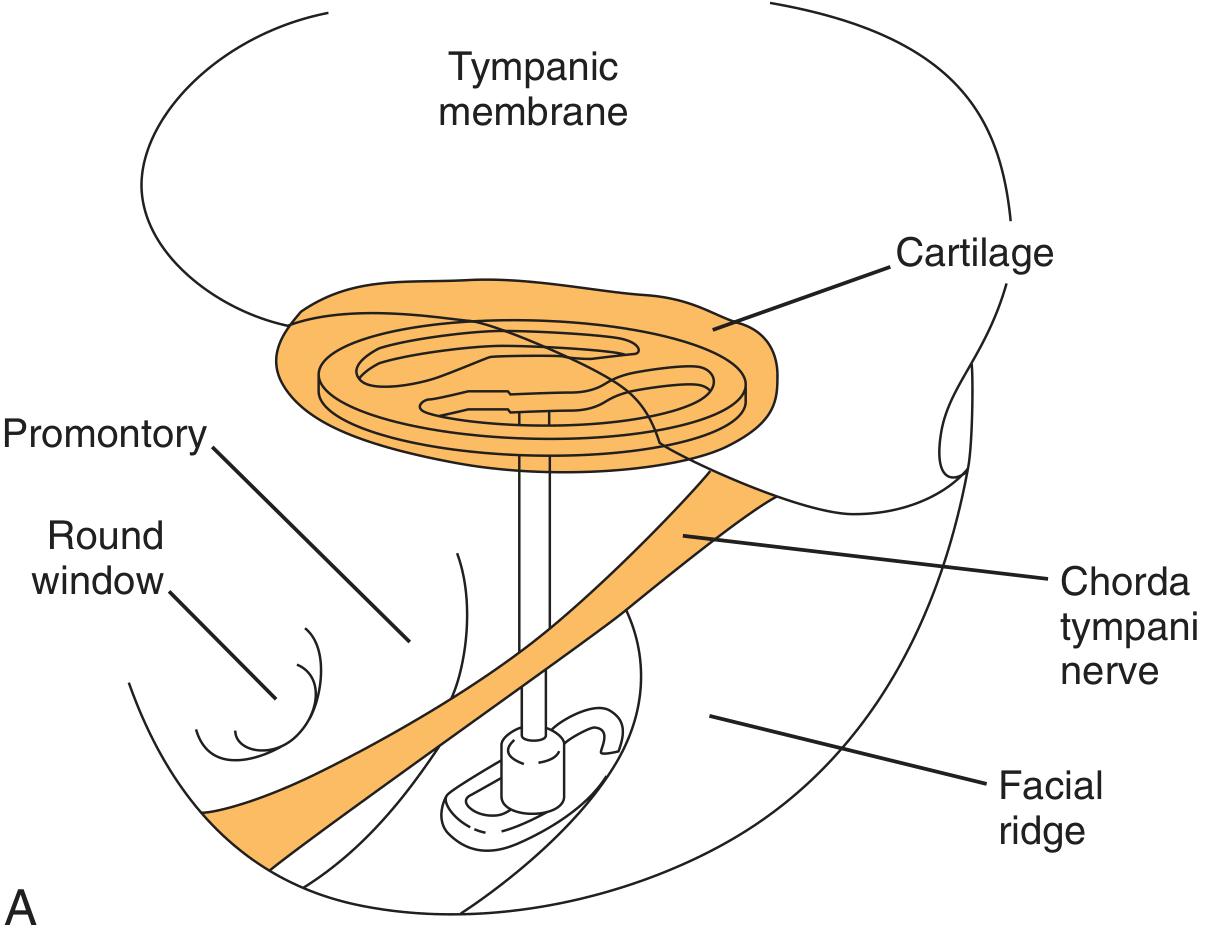
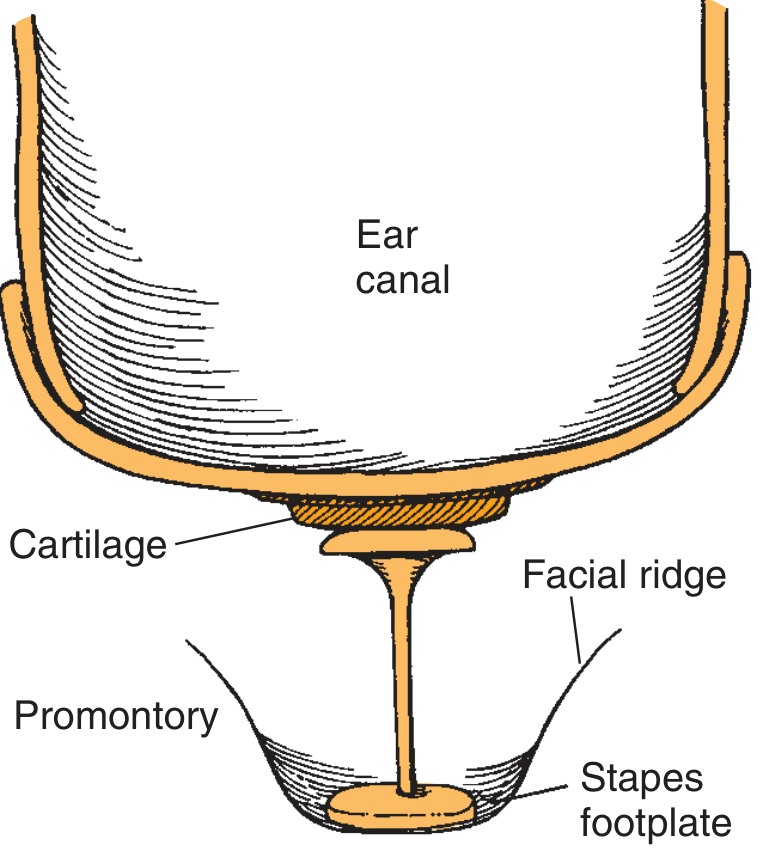
TORP in situ - Diagrams
TORP positioned between stapes footplate and tympanic membrane (intraoperative view)
Schematic of TORP - cartilage interposed between prosthesis head and TM
Materials Used
Historical (now less favored)
| Material | Issue |
|---|---|
| Polyethylene / Teflon | High extrusion rate |
| Proplast / Plasti-Pore | Improved biocompatibility but poor extrusion + hearing results |
| Ceravital / Bioglass (glass ceramics) | Extrusion issues |
Current Standard
| Material | Advantages | Disadvantages |
|---|---|---|
| Titanium | Lightweight (~4 mg), high rigidity, closest mass to native ossicles, excellent visualization during insertion (open headplate design), claw-like base for secure footplate contact, easy handling, low extrusion rate | Cost |
| Hydroxyapatite (HA) | Can integrate with bone without encapsulation; bonds to tissue | Brittle, hard to sculpt intraoperatively |
| Hydroxyapatite + Plasti-Pore composite | HA platform (low extrusion, tissue bonding) + Plasti-Pore shaft (easily trimmed to length) | Combined manufacturing complexity |
Key: Multiple RCTs and a meta-analysis of 12 studies (1388 patients) found no significant difference in stability or hearing outcomes between titanium and non-titanium prostheses. The underlying middle ear pathology has more influence on outcome than prosthesis material.
Surgical Technique - Key Principles (TRACS Mnemonic)
- T - Tension: The prosthesis must be placed under appropriate minimal tension from the TM. Too lax = sound energy loss. Too tight = TM erosion and extrusion. The prosthesis should spontaneously return to position when displaced with gentle pressure.
- R - Rigidity: Higher rigidity = better high-frequency transmission. Titanium is optimal.
- A - Angulation: The TORP must be placed as close to perpendicular to the stapes footplate as possible. Angulation reduces efficiency of piston motion.
- C - Contact: The base must maintain secure stable contact with the footplate center.
- S - Surface (Cartilage interposition): A 0.5-0.7 mm conchal or tragal cartilage graft is always interposed between the TORP headplate and the TM undersurface. This:
- Prevents direct TM-prosthesis contact
- Reduces TM erosion and implant extrusion
- Has minimal acoustic transmission effect when matched to prosthesis head diameter (shown in cadaver studies)
Placement Requirements for TORP
- Mobile footplate preferred - TORP on a fixed footplate gives worse results
- Healthy, well-aerated middle ear mucosa
- Normal middle ear pressure / functional Eustachian tube
- Stable tympanic membrane graft (second-stage TORP placement recommended if TM graft done simultaneously to reduce displacement risk)
Outcomes
| Measure | PORP | TORP |
|---|---|---|
| Air-bone gap < 20 dB | 50-85% of cases | 40-50% of cases |
| 5-year success rate | ~2/3 (67%) | ~1/3 (33%) |
| Extrusion rate (Kurz titanium, 5-yr) | ~5% | ~5% |
TORP outcomes are consistently inferior to PORP because:
- Longer column = less stable; more likely to displace
- No stapes superstructure to provide medial support
- Greater distance to bridge = harder to achieve optimal tension
- Relies entirely on the footplate as the medial anchor
Factors Affecting TORP Success
- Eustachian tube dysfunction (major risk for displacement)
- Chronic infection / mucosal adhesions
- Atelectasis of the middle ear
- Intraoperative stability at time of surgery
- Open vs. closed mastoidectomy technique
- Cartilage cap size and placement
Sources:
- Cummings Otolaryngology Head and Neck Surgery (9780323612173), pp. 2733-2773 - Materials and TORP outcomes
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2 (9781138094634), p. 1076 - TORP terminology and technique
This is a shared conversation. Sign in to Orris to start your own chat.