Pathology of lupus nephritis
Reading File
Finding Sources
Searching PubMed
"lupus nephritis" AND pathology
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I have comprehensive content from multiple authoritative textbooks. Now I'll compile the full pathology response.
Pathology of Lupus Nephritis
Lupus nephritis (LN) is the renal manifestation of systemic lupus erythematosus (SLE). It is the prototype human systemic immune complex disease (type III hypersensitivity), in which autoantibodies against nuclear antigens — most specifically anti-double-stranded DNA (anti-dsDNA) — form immune complexes that deposit predominantly in the glomeruli. The kidney bears the brunt of the lesions and LN is the greatest determinant of morbidity and mortality in SLE patients. It is most common in Black females aged 15–45.
Pathogenesis
The central mechanism involves:
- Autoantibody production — Autoantibodies to nuclear antigens (ANAs), especially anti-dsDNA, anti-histones, anti-Sm, anti-RNP, anti-C1q, and anti-endothelial antigens
- Immune complex deposition in glomeruli → complement activation (classical pathway) → inflammatory cell recruitment → glomerular injury
- Genetic predisposition — >50 polymorphisms associated with susceptibility, including defects in apoptotic debris clearance, innate/adaptive immunity, and toll-like receptor signaling
- NETs (neutrophil extracellular traps) and abnormal apoptosis contribute to nuclear antigen availability
- Tubuloreticular inclusions (TRIs) — Characteristic ultrastructural finding in endothelial cytoplasm, reflecting high interferon-α activity (also seen in HIV)
ISN/RPS Classification (2003, revised 2018)
The International Society of Nephrology / Renal Pathology Society (ISN/RPS) classification recognizes six classes based primarily on light microscopy (LM), with immunofluorescence (IF) and electron microscopy (EM) for confirmation. Class IV is the most common in renal biopsy registries.
Class I — Minimal Mesangial LN
- LM: Normal glomeruli (no structural abnormality)
- IF: Mesangial deposits (IgG, IgM, IgA, C3, C1q)
- EM: Small electron-dense deposits in mesangium only
- Clinical: Asymptomatic; normal urinalysis; rarely biopsied
Class I: Normal-appearing glomerulus on PAS with only mesangial IF deposits (Henry's Clinical Diagnosis, Fig. 55.59)
Class II — Mesangial Proliferative LN
- LM: Mesangial hypercellularity ± mesangial matrix expansion
- IF: Mesangial granular deposits (IgG pattern)
- EM: Electron-dense deposits confined to mesangium
- Clinical: Mild proteinuria or microscopic hematuria; almost never nephrotic syndrome or renal failure
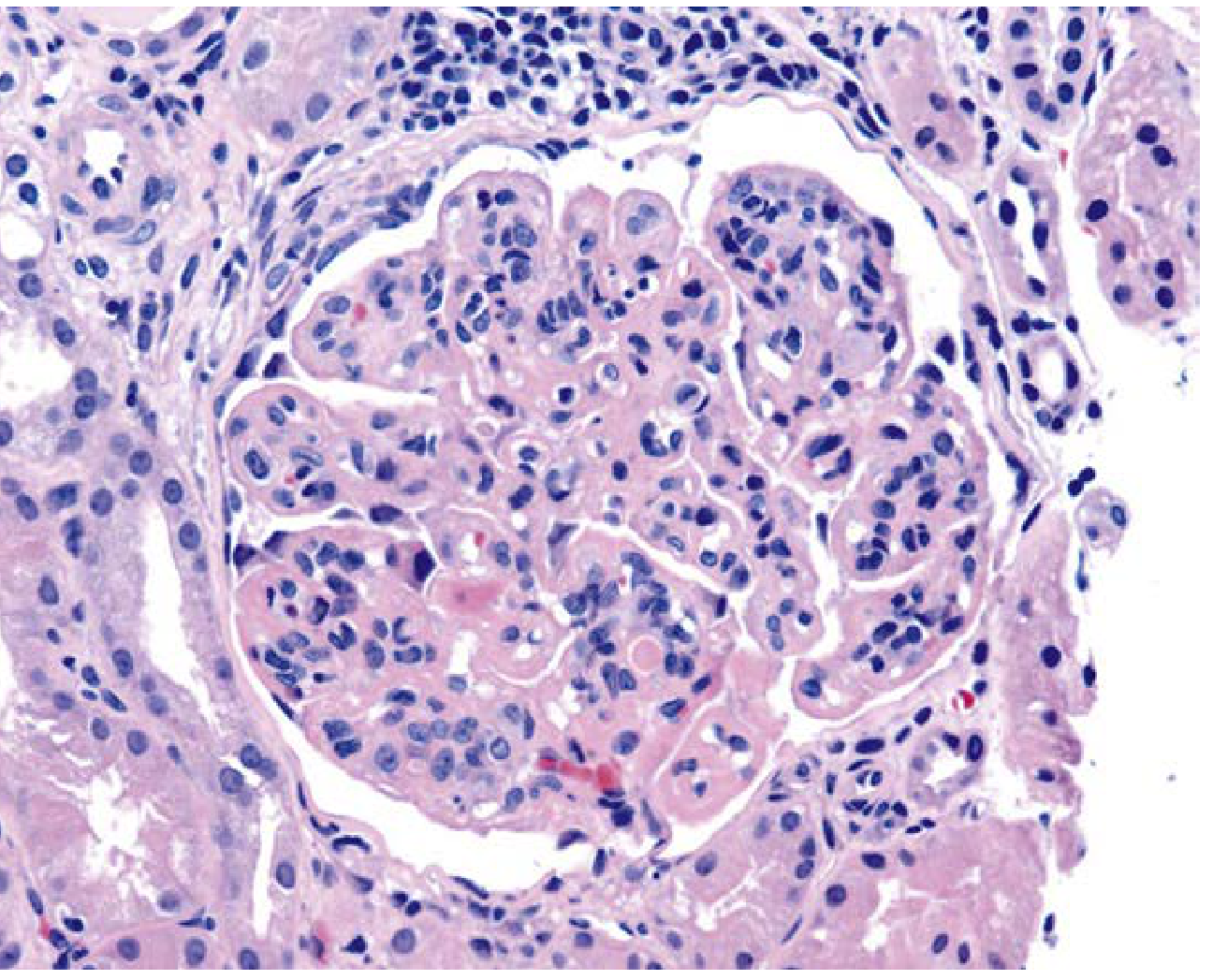
Class III — Focal LN
Defined as involvement of <50% of glomeruli
- LM: Segmental (or global) endocapillary hypercellularity, often with:
- Fibrinoid necrosis and karyorrhectic debris
- Occasional crescents (extracapillary proliferation)
- Leukocyte accumulation
- IF: Strong staining in mesangium and capillary walls/lumina (IgG, C3, C1q)
- EM: Mesangial and subendothelial deposits; podocyte foot processes generally intact
- Clinical: Hematuria, proteinuria, RBC casts; may progress to class IV
Class III: Segmental endocapillary hypercellularity with fibrinoid necrosis and karyorrhectic nuclear debris (Henry's Clinical Diagnosis, Fig. 55.62)
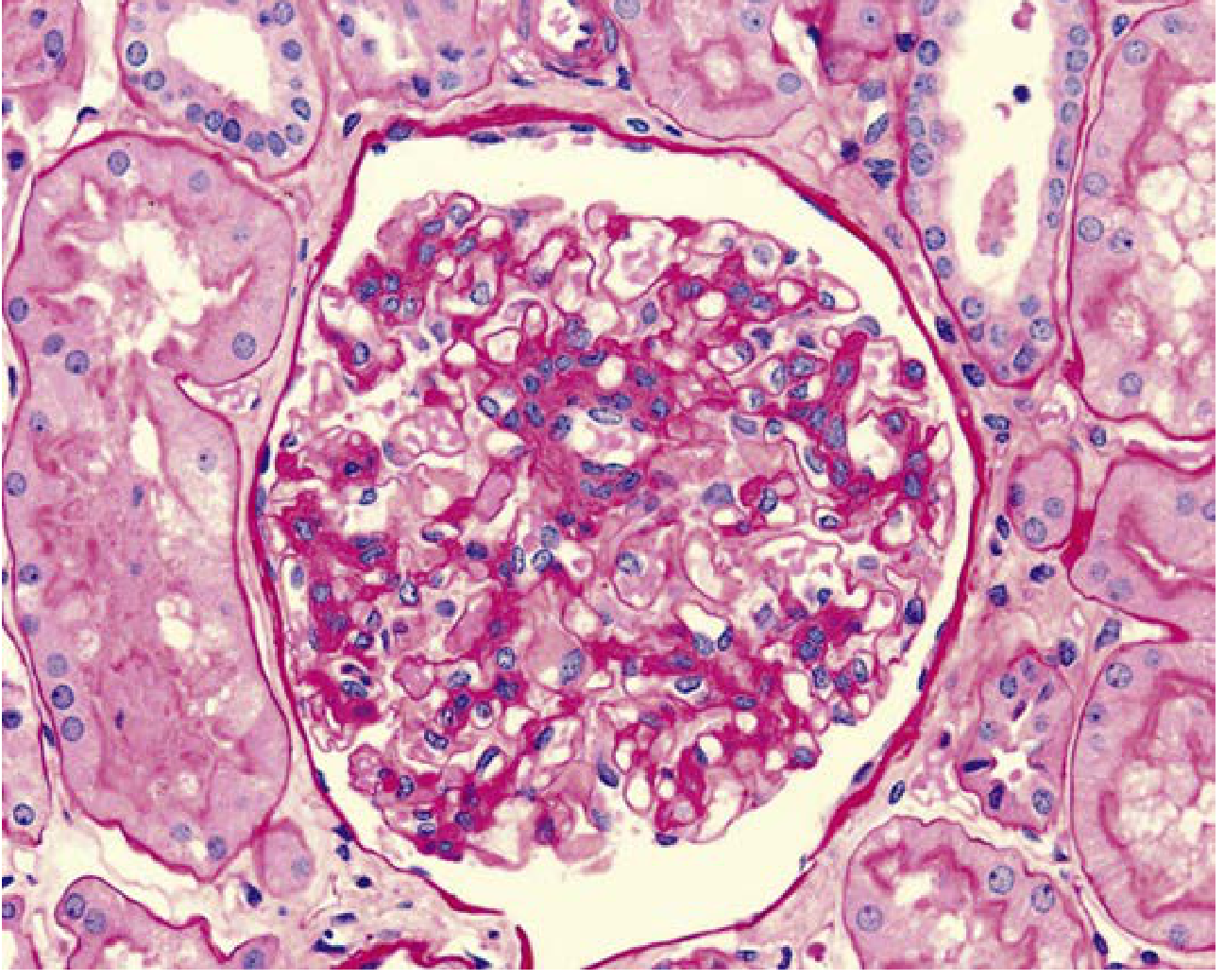
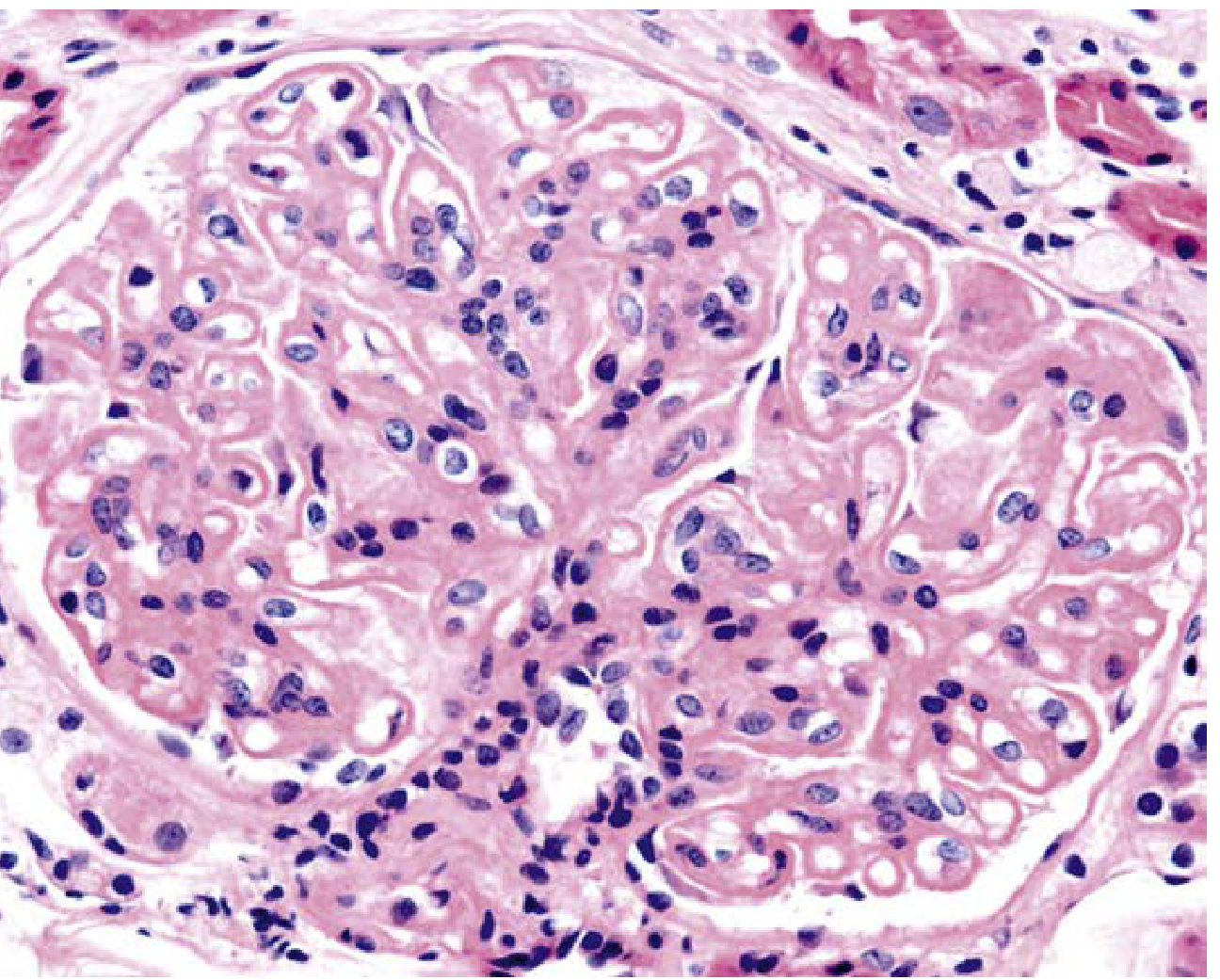
Class IV — Diffuse LN
Most common and most severe form; involves ≥50% of glomeruli
- Subtypes: IV-S (segmental) vs. IV-G (global)
- LM hallmarks:
- Global endocapillary hypercellularity with near-obliteration of capillary lumina
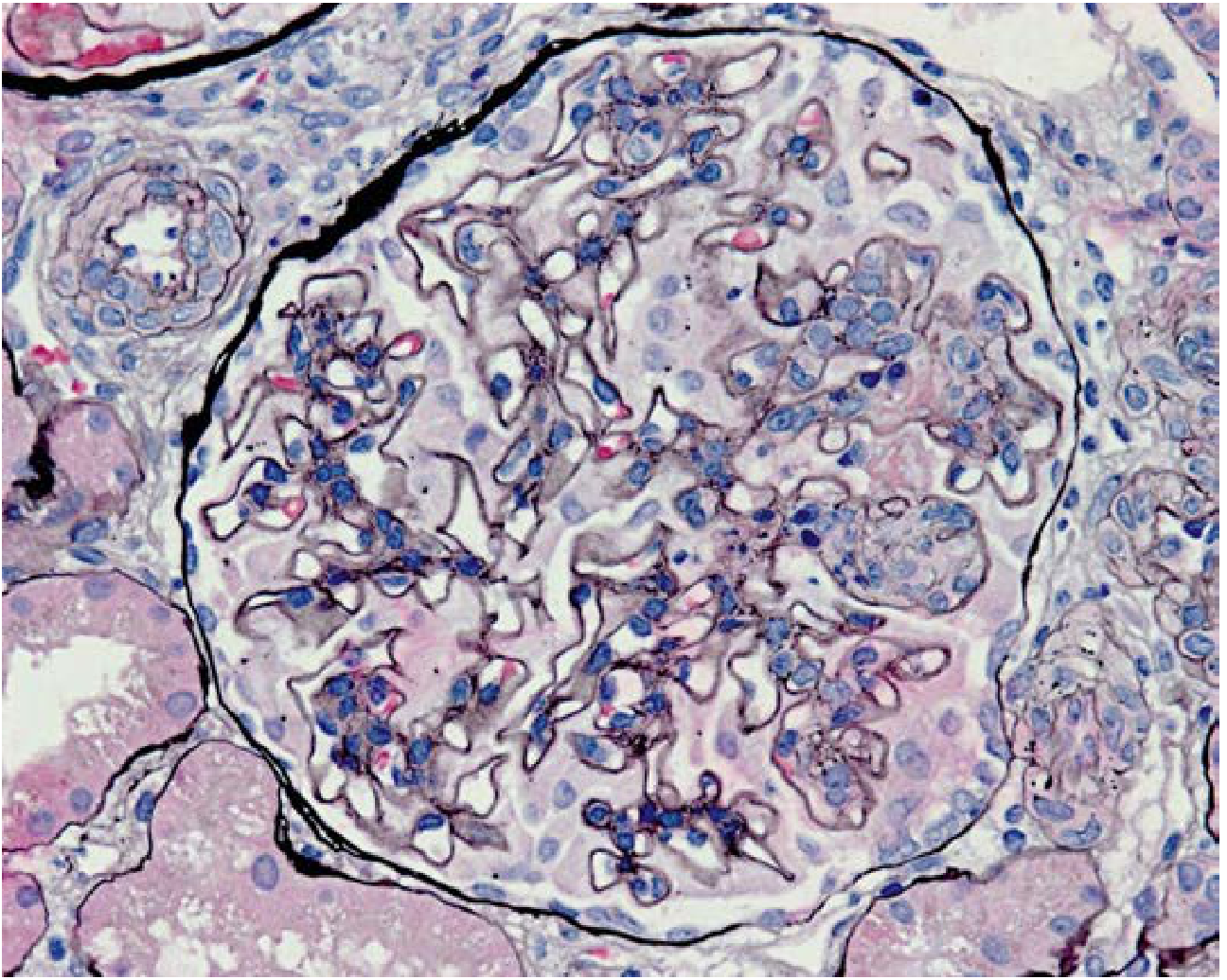
- "Wire-loop" lesions — circumferential eosinophilic thickening of peripheral capillary walls due to massive subendothelial immune deposits (enclosed by silver-positive GBM on Jones silver stain)
- "Hyaline thrombi" — intraluminal capillary deposits (misnomer; actually immune complexes, not true thrombi)
- Fibrinoid necrosis and karyorrhexis (× 2 score on activity index)
- Crescents (cellular/fibrocellular)
- Intraglomerular monocyte accumulation
Class IV: Severe global endocapillary hypercellularity near-occluding capillary lumina (Henry's Clinical Diagnosis, Fig. 55.65)
Class IV: Prominent subendothelial deposits ("wire-loops") enclosed within silver-positive GBMs (Henry's Clinical Diagnosis, Fig. 55.68)
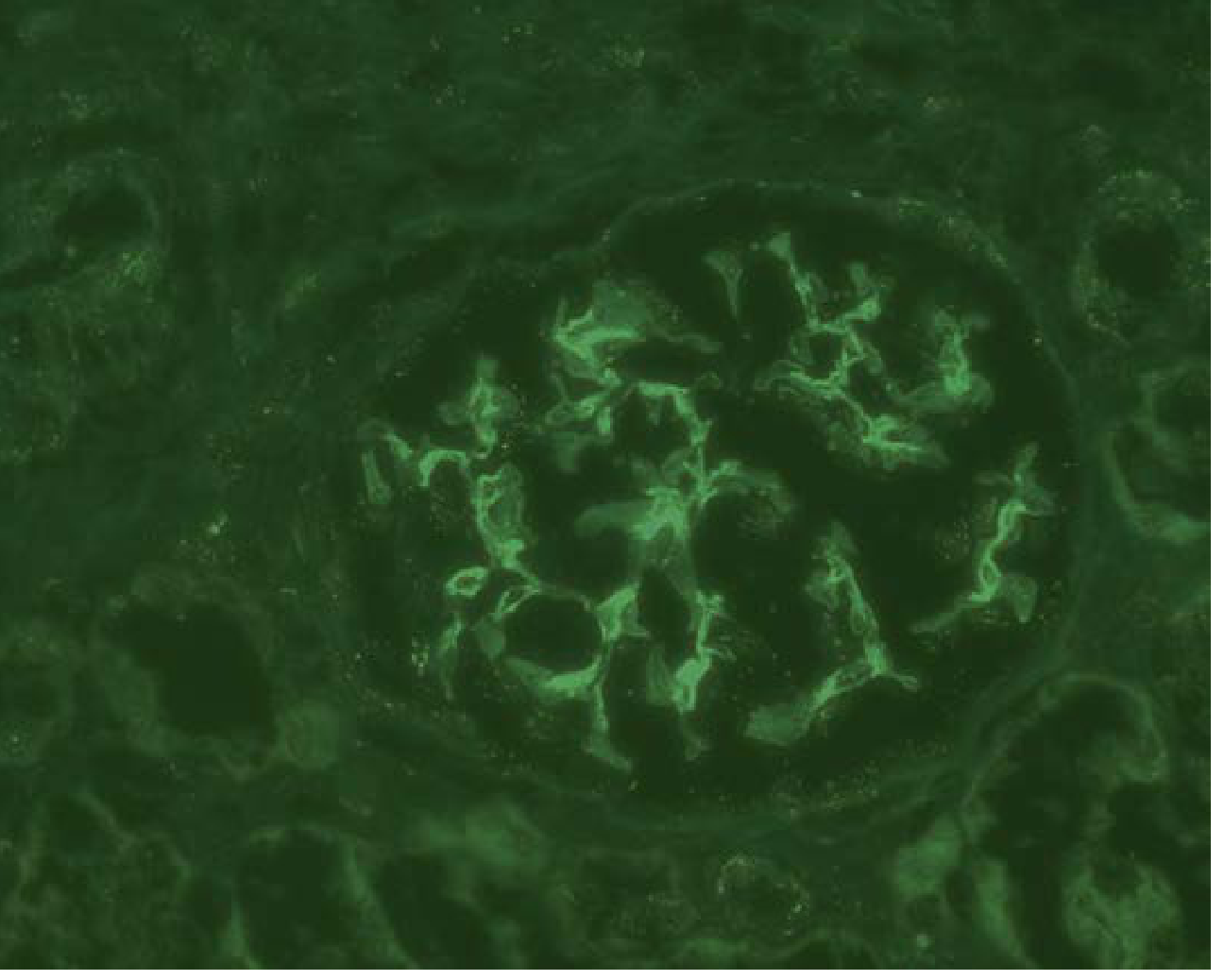
- IF: Diffuse strong staining of mesangium and all peripheral capillary loops — IgG, IgM, IgA, C3, C1q ("full-house" pattern)
- EM: Massive mesangial and subendothelial electron-dense deposits; some may have fingerprint/tubular substructure; tubuloreticular inclusions in endothelial cytoplasm
- Clinical: Hematuria + proteinuria ± nephrotic syndrome; hypertension; renal insufficiency (mild to severe)
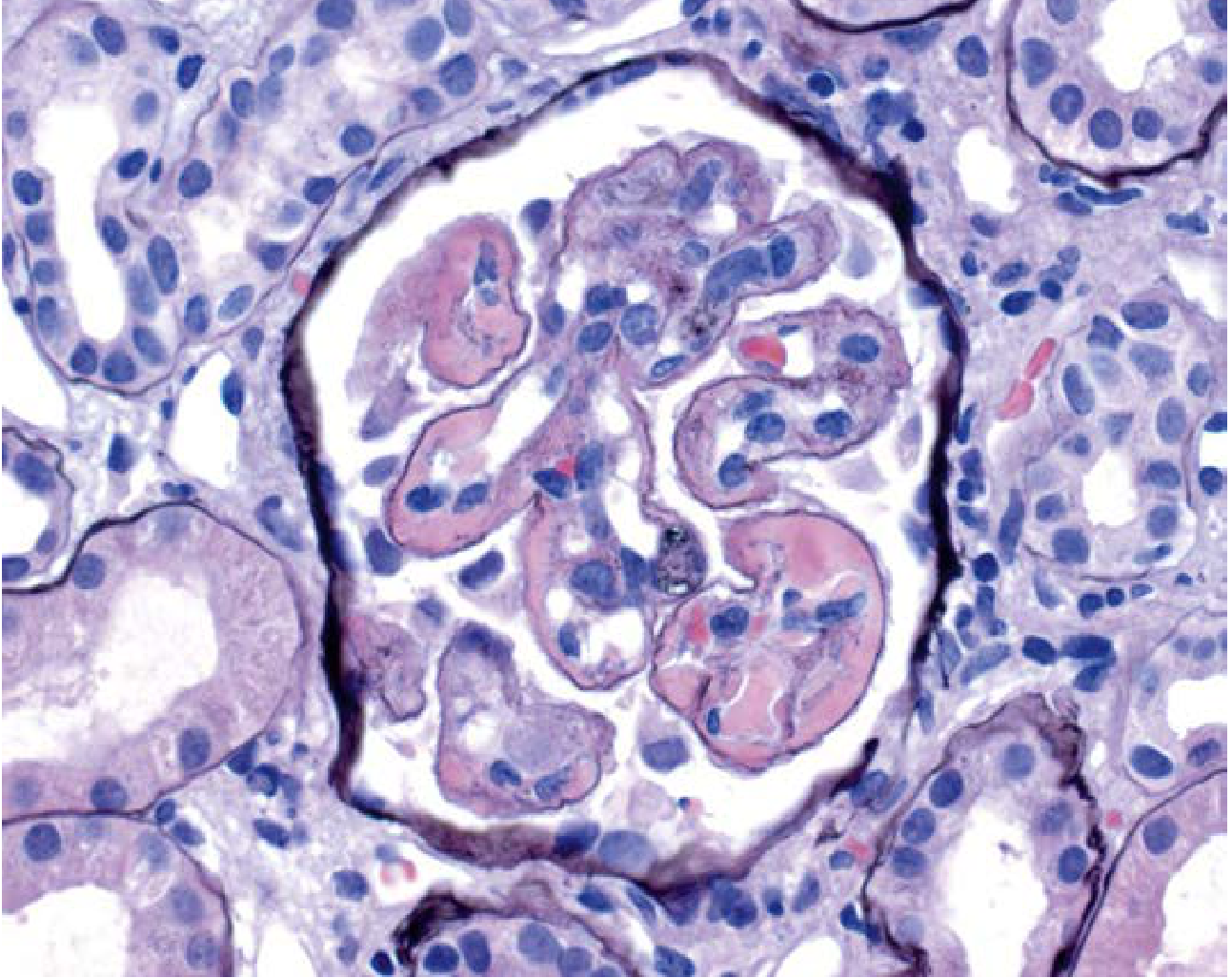
Class V — Membranous LN
- LM: Diffuse thickening of capillary walls (similar to idiopathic membranous nephropathy) ± mild mesangial hypercellularity
- Jones silver stain: GBM "spikes" projecting between subepithelial deposits
- IF: Granular subepithelial IgG along all capillary walls
- EM: Prominent subepithelial electron-dense deposits ± mesangial deposits
- Can occur concurrently with class III or IV (mixed class)
- Clinical: Severe proteinuria / nephrotic syndrome; may have preserved GFR
Class V: Spherical capillary wall thickening and mild mesangial hypercellularity (Henry's Clinical Diagnosis, Fig. 55.75)
Class VI — Advanced Sclerosing LN
- LM: >90% global glomerulosclerosis; no residual activity
- Represents end-stage disease from prior classes
- Clinical: CKD/ESKD; irreversible
Immunofluorescence: The "Full-House" Pattern
A hallmark of LN — positivity for all three immunoglobulins (IgG, IgM, IgA) plus C3 and C1q — distinguishes it from most other glomerulonephritides. This reflects the polyclonal B-cell activation and classical complement pathway activation characteristic of SLE.
Class I: Mesangial IgG fluorescence — confined mesangial pattern (Henry's Clinical Diagnosis, Fig. 55.57)
Electron Microscopy: Deposit Locations by Class
| Class | Mesangial | Subendothelial | Subepithelial |
|---|---|---|---|
| I | + | – | – |
| II | ++ | – | – |
| III | + | + (focal) | – |
| IV | +++ | +++ | – |
| V | ± | – | +++ |
Deposits in class IV may show a fingerprint or tubular substructure, and tubuloreticular inclusions (TRIs) are a characteristic EM finding in endothelial cells (also seen in HIV and other collagen vascular diseases, reflecting interferon-α stimulation).
Extraglomerular Lesions
LN may involve all renal parenchymal compartments, and extraglomerular pathology improves predictive value for outcome:
- Vascular lesions: Immune complex vasculopathy (IF-detectable deposits in vessel walls), noninflammatory necrotizing vasculopathy, thrombotic microangiopathy (associated with antiphospholipid antibodies), and true lupus vasculitis (rare)
- Tubulointerstitial nephritis: Interstitial inflammation and tubulitis — scored in the NIH activity index; associated with worse prognosis
- Tubular atrophy and interstitial fibrosis: Scored in the NIH chronicity index
NIH Activity and Chronicity Indices
Semi-quantitative scoring (0–3+ per lesion) applied at biopsy to assess disease severity and guide therapy:
Activity Index (0–24 total):
| Lesion | Weight |
|---|---|
| Endocapillary hypercellularity | ×1 |
| Neutrophil infiltration | ×1 |
| Subendothelial hyaline deposits (wire loops) | ×1 |
| Fibrinoid necrosis / karyorrhexis | ×2 |
| Cellular crescents | ×2 |
| Interstitial inflammation | ×1 |
Chronicity Index (0–12 total):
| Lesion | Weight |
|---|---|
| Glomerulosclerosis | ×1 |
| Fibrous crescents | ×1 |
| Tubular atrophy | ×1 |
| Interstitial fibrosis | ×1 |
High activity index → aggressive immunosuppression. High chronicity index → less likely to respond to treatment; predicts progression to ESKD.
Class Transitions and Mixed Classes
Lesions are not static — they can evolve from one class to another over time (e.g., class III → IV). Mixed classes occur (most commonly class IV + V), and follow-up biopsies may show transformation. Repeat renal biopsy in complete remission may guide immunosuppression tapering and predict relapse.
Summary Table
| Class | Name | LM | IF | Deposits (EM) | Clinical |
|---|---|---|---|---|---|
| I | Minimal mesangial | Normal | Mesangial | Mesangial | Asymptomatic |
| II | Mesangial proliferative | Mesangial hypercellularity | Mesangial | Mesangial | Mild proteinuria/hematuria |
| III | Focal | <50% glomeruli involved; necrosis, crescents | Mesangial + focal capillary wall | Mesangial + subendothelial | Hematuria, proteinuria, RBC casts |
| IV | Diffuse | ≥50% glomeruli; wire loops, hyaline thrombi | "Full-house" mesangial + capillary | Massive subendothelial + mesangial | Nephritic/nephrotic, HTN, renal failure |
| V | Membranous | GBM thickening, spikes | Granular subepithelial | Subepithelial | Nephrotic syndrome |
| VI | Advanced sclerosing | >90% global sclerosis | Minimal/absent | Sclerosis | ESKD |
Sources: Robbins & Kumar Basic Pathology, p. 12.11; Henry's Clinical Diagnosis and Management by Laboratory Methods, pp. 1262–1265; Brenner and Rector's The Kidney, Ch. 44
Recent evidence note: A 2026 systematic review (PMID 41169181) in Arthritis & Rheumatology evaluates biomarkers of LN histopathology, underscoring ongoing efforts to correlate non-invasive markers with specific pathological classes — useful context for monitoring without repeat biopsy.
This is a shared conversation. Sign in to Orris to start your own chat.