10 ecg common in day to day life in emergency with image
Reading File
Finding Sources
Searching Images
ST elevation myocardial infarction STEMI ECG
Searching Images
ventricular fibrillation ECG cardiac arrest
Searching Images
atrial fibrillation ECG irregular rhythm
Searching Images
complete heart block third degree AV block ECG
Searching Images
ventricular tachycardia ECG wide complex
Searching Images
hyperkalemia tall peaked T waves sine wave ECG
Searching Images
pulmonary embolism S1Q3T3 right heart strain ECG
Searching Images
Wolff-Parkinson-White WPW delta wave ECG
Searching Images
supraventricular tachycardia SVT narrow complex ECG
Searching Images
left bundle branch block LBBB ECG pattern
I now have excellent images for all 10 ECG patterns. Here is the comprehensive guide:
10 Common Emergency ECGs with Images
1. STEMI — ST-Elevation Myocardial Infarction
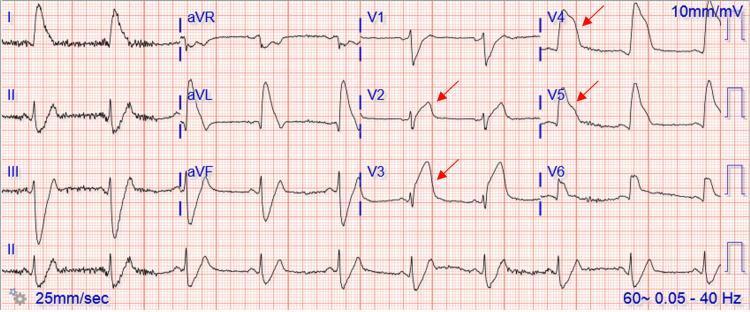
Key features:
- Convex ("tombstone") ST elevation ≥1 mm in ≥2 contiguous leads
- Reciprocal ST depression in opposite leads (e.g., inferior STEMI → depression in aVL)
- Hyperacute T waves in early phase
- Pathological Q waves in established infarction
Localisation:
| Territory | Leads with ST elevation | Culprit artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA / LCx |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | ST depression V1–V3 + tall R V1 | RCA/LCx |
Emergency action: Immediate reperfusion (PCI within 90 min, thrombolysis if PCI unavailable)
2. Ventricular Fibrillation (VF)

Key features:
- Completely chaotic, disorganised baseline
- No identifiable P waves, QRS, or T waves
- Variable amplitude oscillations — "coarse VF" (large amplitude) or "fine VF" (small amplitude)
- No cardiac output — pulseless arrest
Emergency action: Immediate defibrillation (360 J monophasic / 200 J biphasic) + CPR. Shockable rhythm — do NOT delay.
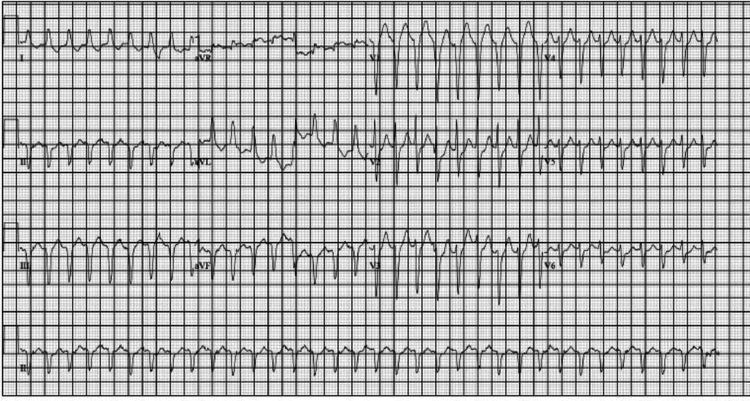
3. Ventricular Tachycardia (VT)

Key features:
- Wide QRS complex (>120 ms), regular rhythm, rate 100–250 bpm
- AV dissociation (P waves independent of QRS)
- Fusion beats and capture beats (pathognomonic)
- Positive concordance across precordial leads (all QRS same direction)
- Brugada criteria / Vereckei algorithm to distinguish from SVT with aberrancy
Emergency action: Pulseless VT → defibrillate. Stable VT → amiodarone 300 mg IV, synchronised cardioversion if haemodynamically unstable.
4. Atrial Fibrillation (AF)

Key features:
- Irregularly irregular RR intervals — the hallmark
- Absent P waves — replaced by fine fibrillatory (f) waves, best seen in V1 and inferior leads
- Narrow QRS (unless aberrant conduction/bundle branch block)
- Ventricular rate varies: controlled <100 bpm, rapid response >100 bpm
Emergency action: Rate control (metoprolol, diltiazem, digoxin), rhythm control (cardioversion if <48 h or anticoagulated), anticoagulation for stroke prevention (CHA₂DS₂-VASc score).
5. Complete (Third-Degree) AV Block

Key features:
- Complete AV dissociation — P waves and QRS have no relationship
- P waves march through at a faster atrial rate (e.g., 80 bpm)
- Slow escape rhythm: narrow QRS if junctional escape (40–60 bpm); wide QRS if ventricular escape (<40 bpm)
- Bradycardia often causes haemodynamic compromise (syncope, hypotension)
Emergency action: Atropine (1 mg IV) as temporising measure; transcutaneous pacing urgently; plan for permanent pacemaker. Treat reversible causes (inferior MI, hyperkalemia, drug toxicity).
6. Supraventricular Tachycardia (SVT / AVNRT / AVRT)
Key features:
- Narrow complex tachycardia (QRS <120 ms), regular, rate 150–250 bpm
- P waves absent or retrograde (buried in or just after QRS)
- Abrupt onset and termination
- Pseudo-R' in V1 or pseudo-S in inferior leads (hallmark of AVNRT)
- ST depression may be present (rate-related, not ischaemic)
Emergency action: Vagal manoeuvres first (Valsalva, carotid sinus massage); adenosine 6 mg rapid IV (then 12 mg if needed); synchronised DC cardioversion if haemodynamically unstable.
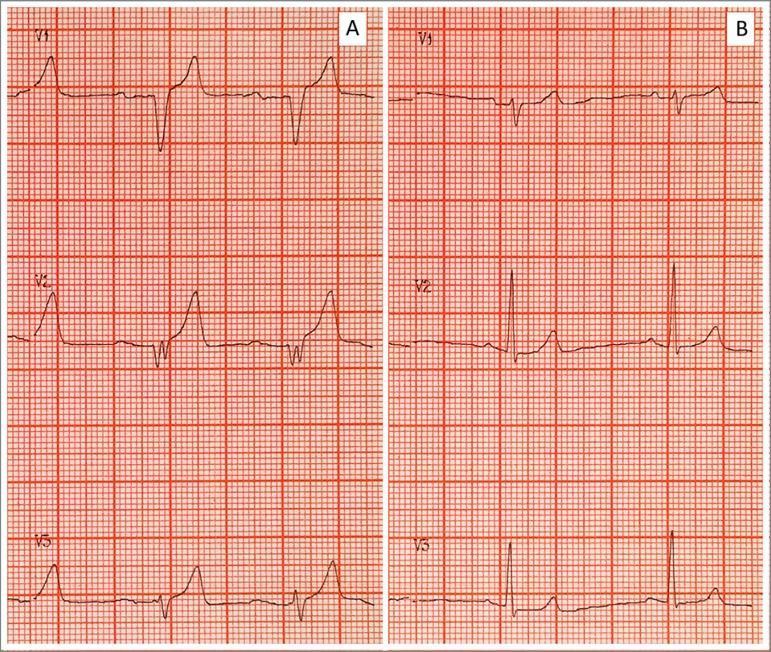
7. Pulmonary Embolism — Right Heart Strain

Key features:
- Sinus tachycardia — most common and most sensitive finding
- S1Q3T3: Deep S wave in lead I + Q wave in lead III + T-wave inversion in lead III (only 20% sensitive, but specific)
- T-wave inversion V1–V4 (right heart strain)
- Incomplete/complete RBBB (acute RV dilatation)
- Right axis deviation, P pulmonale
Emergency action: CTPA for diagnosis; anticoagulation (LMWH/UFH); thrombolysis (alteplase 100 mg IV) for massive PE with haemodynamic compromise.
8. Hyperkalemia
Progressive ECG changes with rising K⁺:
| Serum K⁺ | ECG finding |
|---|---|
| 5.5–6.5 mEq/L | Tall, narrow, peaked/tented T waves |
| 6.5–7.5 mEq/L | Prolonged PR, P wave flattening/disappearance |
| 7.5–8.5 mEq/L | Wide QRS, bundle branch block pattern |
| >8.5 mEq/L | Sine-wave pattern → VF/asystole |
Emergency action: Calcium gluconate 1g IV (membrane stabilisation, immediate); insulin + dextrose; sodium bicarbonate; salbutamol nebulisation; furosemide; haemodialysis for severe/refractory cases.
9. Wolff-Parkinson-White (WPW) Syndrome

Key features:
- Short PR interval (<120 ms)
- Delta wave — slurred upstroke at the start of QRS
- Wide QRS (>120 ms) due to pre-excitation
- Discordant ST-T changes (secondary to pre-excitation)
- Risk of pre-excited AF → rapid ventricular rates → VF
Emergency action: Pre-excited AF (irregular wide complex tachycardia) → avoid AV nodal blockers (adenosine, digoxin, verapamil — can accelerate conduction via bypass tract → VF). Use procainamide or DC cardioversion. Refer for radiofrequency ablation.
10. Left Bundle Branch Block (LBBB) — New/Presumed New
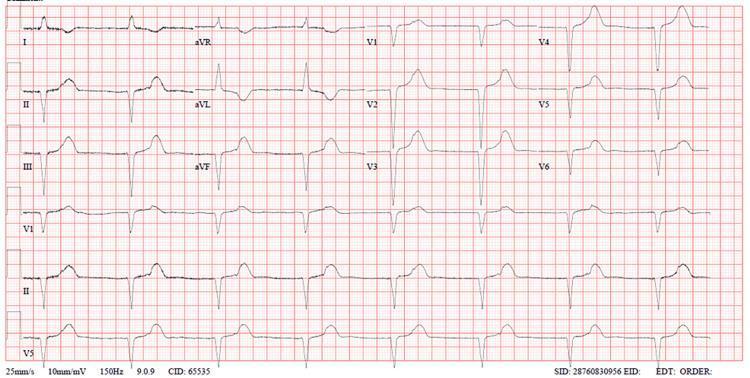
Key features (remember "WiLLiaM MaRRoW"):
- QRS ≥120 ms
- Broad, notched M-shaped R wave in I, aVL, V5–V6 (William = W in V1, M in V6)
- Deep broad W-shaped QS in V1–V3
- Discordant ST-T changes (ST elevation in V1–V3, depression/inversion laterally)
- Absence of septal Q waves in I and V6
Why it matters in ED: New LBBB with chest pain = treat as STEMI equivalent (Sgarbossa criteria help identify true STEMI within LBBB). Concordant ST elevation ≥1 mm in any lead is highly specific for MI.
Emergency action: New LBBB with ischaemic symptoms → activate cath lab. Investigate for underlying structural disease (cardiomyopathy, valvular disease).
Quick Reference Summary
| # | Rhythm/Pattern | Rate | QRS | Key Hallmark | Emergency Action |
|---|---|---|---|---|---|
| 1 | STEMI | Normal | Narrow | ST elevation + reciprocal changes | PCI/thrombolysis |
| 2 | VF | Chaotic | None | Chaotic baseline | Defibrillate NOW |
| 3 | VT | 100–250 | Wide | AV dissociation | Defib/amiodarone |
| 4 | AF | Irregular | Narrow | No P waves, irregular RR | Rate/rhythm control |
| 5 | Complete AV Block | <40–60 | Wide/narrow | P–QRS dissociation | Pacing |
| 6 | SVT | 150–250 | Narrow | Regular, no P waves | Adenosine/vagal |
| 7 | PE | Fast | Narrow | S1Q3T3, sinus tachy | Anticoagulation/thrombolysis |
| 8 | Hyperkalemia | Variable | Wide→sine | Peaked T → sine wave | Calcium/insulin |
| 9 | WPW | Variable | Wide (pre-excited) | Delta wave, short PR | Procainamide/ablation |
| 10 | New LBBB | Normal | Wide | WiLLiaM pattern | Treat as STEMI if acute |
This is a shared conversation. Sign in to Orris to start your own chat.