Anemia – Complete Diagnostic Approach (Stepwise) Also extract high quality images wherever necessary for showcasing any clinical findings
anemia blood smear peripheral smear microcytic hypochromic iron deficiency
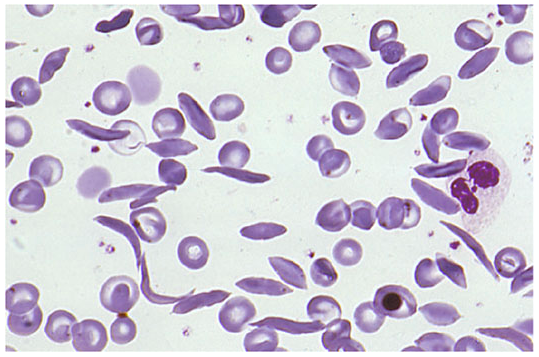
sickle cell anemia target cells schistocytes spherocytes blood smear morphology
Anemia — Complete Diagnostic Approach (Stepwise)
Physiologic Basis
Definition: Normal Hemoglobin/Hematocrit Values
| Population | Hemoglobin (g/dL) | Hematocrit (%) |
|---|---|---|
| Adult man | 16 (±2) | 47 (±6) |
| Adult woman (menstruating) | 13 (±2) | 40 (±6) |
| Adult woman (postmenopausal) | 14 (±2) | 42 (±6) |
| Pregnancy | 12 (±2) | 37 (±6) |
| Childhood | 12 | 36 |
| Newborn | 17 | 52 |
Step 1 — History
- Previous episodes of anemia, prior iron pills or transfusions
- Family history (hemoglobinopathies, hereditary spherocytosis)
- Menstrual history: duration of periods, number of pads/tampons, large clots
- Blood donation
- Dietary history (vegetarian/vegan → B12 risk; poor diet → folate risk)
- Alcohol use, liver disease, hypothyroidism
- Symptoms pointing to underlying cause: diarrhea (celiac, IBD), bone pain (myeloma), weight loss (malignancy), neurological symptoms (B12 deficiency)
- Medications (chemotherapy, methotrexate, antiseizure drugs, ACE inhibitors, NSAIDs → GI blood loss)
- Geography/ethnicity (sickle cell, thalassemia in relevant populations)
Step 2 — Physical Examination
- Consequences of anemia: pallor of mucosa/conjunctiva, resting tachycardia, cardiac flow murmur, dyspnea
- Clues to cause:
- Splenomegaly → hemolysis, lymphoma, portal hypertension
- Lymphadenopathy → lymphoma, leukemia
- Hepatomegaly/jaundice → hemolytic anemia, liver disease
- Glossitis, angular cheilitis, koilonychia → iron deficiency
- Neurologic signs (subacute combined degeneration) → B12 deficiency
- Petechiae/bleeding → aplastic anemia, thrombocytopenia
- Rectal exam/occult blood → GI blood loss
Step 3 — Initial Laboratory Work-Up
Complete Blood Count (CBC) with Differential
| Index | Normal Range | Significance |
|---|---|---|
| Hemoglobin/Hematocrit | See above | Defines severity |
| MCV (Mean Corpuscular Volume) | 80–100 fL | Size classification |
| MCH | 27–33 pg | Hemoglobin content per cell |
| MCHC | 32–36 g/dL | Hemoglobin concentration |
| RDW (Red Cell Distribution Width) | 11.5–14.5% | Anisocytosis |
| WBC + differential | — | Pancytopenia, leukocytosis |
| Platelet count | — | Bone marrow function |
Reticulocyte Count — The Critical Branching Point
- Elevated ARC (>100,000/μL) → Bone marrow is responding → anemia due to increased loss or destruction (bleeding or hemolysis)
- Low/normal ARC (<50,000/μL) → Bone marrow is failing to respond → anemia due to impaired production (hypoproliferative)
The reticulocyte production index (RPI) = [reticulocyte % × Hct/45] / maturation factor. An RPI <2 indicates hypoproliferation; RPI >3 indicates hyperproliferation.
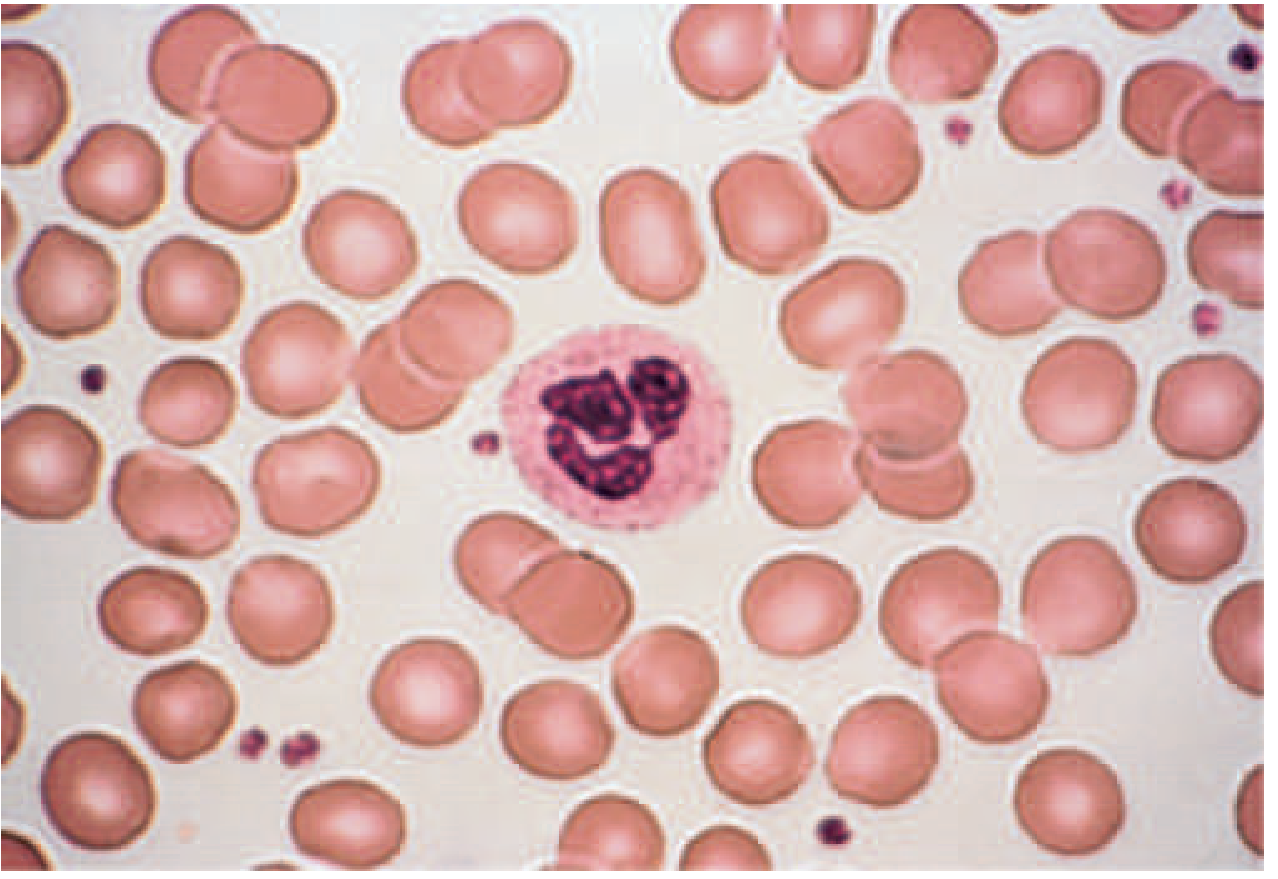
Step 4 — Peripheral Blood Smear (MANDATORY)
"A review of the blood smear is a crucial part of any evaluation for anemia as changes in red cell morphology can point to specific causes of anemia." — Harrison's 22E
Normal Blood Smear (Reference)
Key Red Cell Morphology and Diagnostic Significance
| Morphology | Pathophysiology | Disease States |
|---|---|---|
| Microcytosis / Hypochromia | Inadequate hemoglobinization | Iron deficiency, thalassemia, sideroblastic anemia, anemia of chronic disease |
| Macro-ovalocytes | Nuclear-cytoplasmic dyssynchrony | B12 / folate deficiency, myelodysplasia, chemotherapy |
| Spherocytes | Loss of red cell membrane | Hereditary spherocytosis, autoimmune hemolytic anemia |
| Schistocytes | Mechanical fragmentation | TTP/HUS, DIC, prosthetic heart valve hemolysis, march hemoglobinuria |
| Sickle cells | Hemoglobin polymerization | Sickle cell disease (HbSS, HbSC) |
| Target cells | Relative membrane excess | Liver disease, thalassemia, hemoglobinopathies |
| Polychromasia | Persistence of RNA in reticulocytes | Hemolytic anemia, blood loss |
| Basophilic stippling | Pathologic polyribosome precipitation | Thalassemia, lead poisoning |
| Howell-Jolly bodies | Nuclear remnants | Asplenia, functional hyposplenism |
| Teardrop cells + nucleated RBCs | Marrow architecture disruption | Myelofibrosis, myelophthisic anemia |
| Hypersegmented neutrophils | Impaired DNA synthesis | B12/folate deficiency (megaloblastic anemia) |
Step 5 — MCV-Based Classification and Targeted Workup
5A — Microcytic Anemia (MCV < 80 fL)
Peripheral Smear: Severe Iron Deficiency Anemia
| Test | Iron Deficiency | Anemia of Inflammation | Thalassemia | Sideroblastic Anemia |
|---|---|---|---|---|
| Smear | Micro/hypo | Normal or micro/hypo | Micro/hypo + targeting | Variable |
| Serum iron (μg/dL) | <30 | <50 | Normal–high | Normal–high |
| TIBC (μg/dL) | >360 | <300 | Normal | Normal |
| Transferrin saturation | <10% | 10–20% | 30–80% | 30–80% |
| Ferritin (μg/L) | <15 | 30–200 | 50–300 | 50–300 |
| Hb electrophoresis | Normal | Normal | Abnormal (β-thal); may be normal (α-thal) | Normal |
| RDW | High (anisocytosis) | Normal | Low (homogeneous cells) | Variable |
Key distinguishing clue: RDW is high in iron deficiency (anisocytosis) but low in thalassemia (uniform microcytosis). — Harrison's 22E
Ferritin <30 μg/L = depleted iron stores. Ferritin >200 μg/L = some tissue stores remain. However, ferritin is an acute-phase reactant — it may be falsely elevated in inflammation even with concurrent iron deficiency.
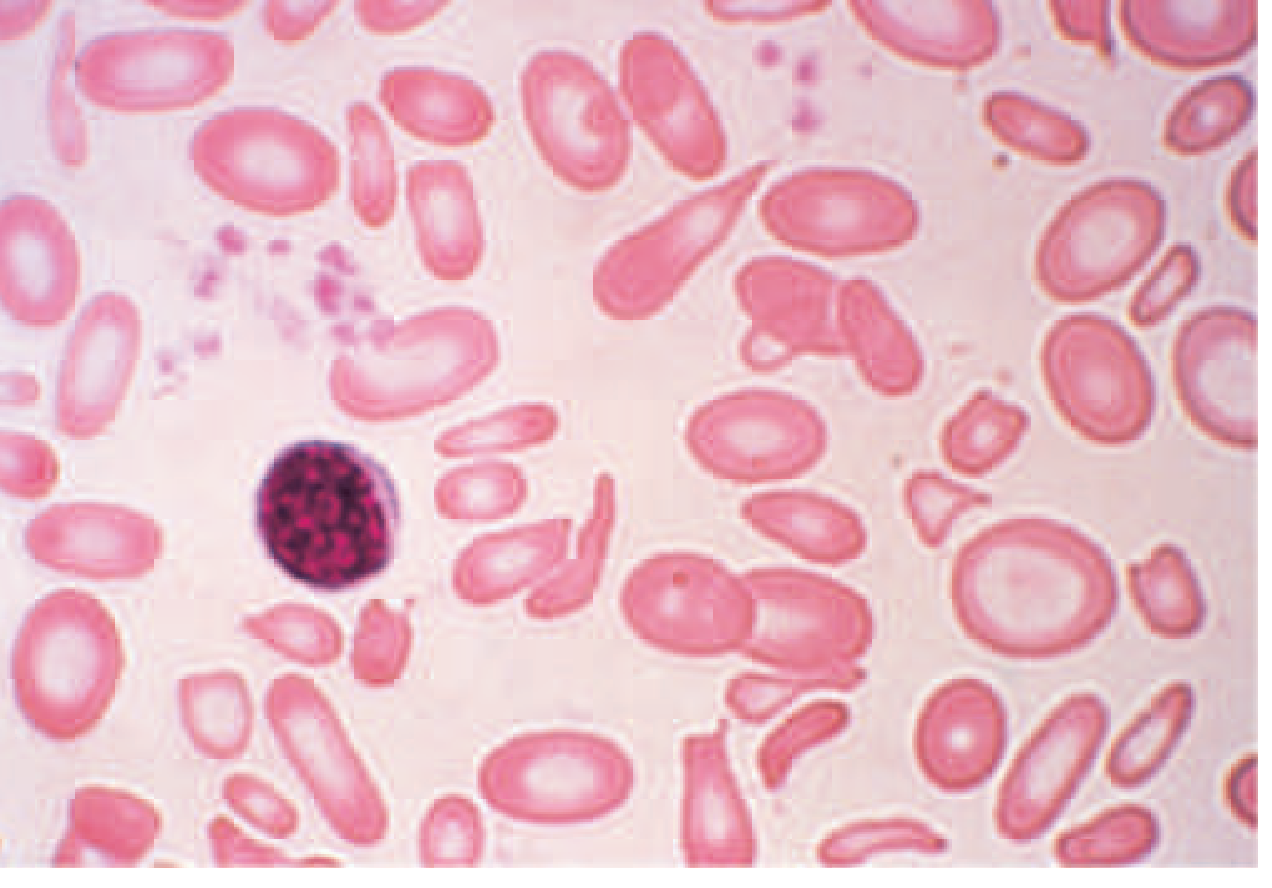
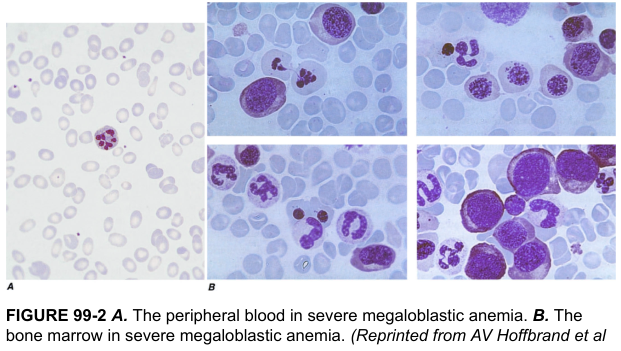
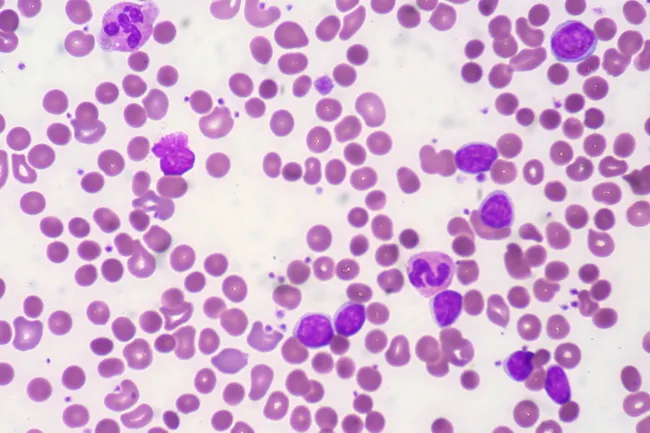
5B — Macrocytic Anemia (MCV > 100 fL)
Oval Macrocytes (Megaloblastic pattern)
- Causes: Vitamin B12 deficiency · Folate deficiency · Chemotherapy agents (hydroxyurea, methotrexate) · Myelodysplastic syndrome (MDS)
Round Macrocytes (Non-megaloblastic)
- Causes: Alcohol use · Liver disease · Hypothyroidism · Reticulocytosis · Dysproteinemia · Smoking · Hypoxia
Peripheral Smear + Bone Marrow: Severe Megaloblastic Anemia
- Blood smear — oval vs. round macrocytes? Hypersegmented neutrophils?
- If megaloblastic pattern: Serum B12 + serum folate / RBC folate
- If B12 low: anti-intrinsic factor antibodies (pernicious anemia), Schilling test if needed
- If B12/folate normal with macro-ovalocytes: bone marrow biopsy (suspect MDS)
- If round macrocytes: check TSH, LFTs, alcohol history
5C — Normocytic Anemia (MCV 80–100 fL)
- Aplastic anemia · Pure red cell aplasia
- Renal disease (EPO deficiency)
- Anemia of inflammation/chronic disease
- Endocrinopathies (hypothyroidism, Addison's)
- Marrow infiltration (myeloma, metastases, granulomas)
- Stem cell defects (leukemia, MDS)
- Acute blood loss/early iron deficiency
- Reticulocyte count (see Step 4 above)
- Renal function (Cr/eGFR), EPO level
- TSH, cortisol (endocrine causes)
- Serum protein electrophoresis (SPEP) for myeloma
- LDH, haptoglobin, bilirubin (if hemolysis suspected)
- Consider bone marrow exam if no clear cause found
Step 6 — Reticulocyte-Guided Mechanistic Workup
6A — High Reticulocyte Count → Hemolysis / Blood Loss
Hemolysis Workup:
| Test | Finding in Hemolysis |
|---|---|
| LDH | Elevated (abundant in RBCs) |
| Serum haptoglobin | Low (binds free Hb; consumed) |
| Indirect bilirubin | Elevated |
| Urine hemoglobin/hemosiderin | Positive in intravascular hemolysis |
| Direct Antiglobulin Test (DAT/Coombs) | Positive → immune-mediated (AIHA) |
| Peripheral smear | Spherocytes (AIHA, HS), schistocytes (TTP/HUS), sickle cells |
| Osmotic fragility | Increased in hereditary spherocytosis |
| G6PD assay | Low in G6PD deficiency |
| Hb electrophoresis | Abnormal in hemoglobinopathies |
| Flow cytometry (CD55/CD59) | Absent in PNH |
Autoimmune Hemolytic Anemia — Peripheral Smear
Sickle Cell Disease — Peripheral Smear
6B — Low Reticulocyte Count → Hypoproliferative (Underproduction)
"At least 75% of all cases of anemia are hypoproliferative in nature." — Harrison's 22E
Sub-classification by mechanism:
| Mechanism | Key Features | Diagnostic Test |
|---|---|---|
| Nutritional (Iron) | Microcytic, low ferritin, high TIBC | Ferritin, serum iron, TIBC |
| Nutritional (B12/Folate) | Macrocytic, hypersegmented PMNs | Serum B12, folate, MMA, homocysteine |
| Renal (EPO deficiency) | Normocytic, eGFR <30–60 | Creatinine, eGFR, EPO level |
| Anemia of inflammation | Normocytic or mild microcytic; high ferritin, low TIBC | CRP, ESR, ferritin, underlying disease |
| Marrow replacement | Myelophthisic picture (teardrops, nRBCs, leukoerythroblastosis) | BM biopsy |
| Aplastic anemia | Pancytopenia, hypocellular marrow | BM biopsy (hypocellular) |
| Pure red cell aplasia | Very low retics, normal WBC/plt, absent erythroid precursors | BM biopsy, parvovirus B19 serology |
| MDS | Macro-ovalocytes, dysplastic WBCs/platelets | BM biopsy + cytogenetics |
| Leukemia | Pancytopenia, blasts on smear | BM biopsy + molecular testing |
Anemia of Chronic Inflammation — Mechanism
- Iron absorption from the gut
- Iron release from macrophages/stores → Functional iron deficiency despite normal/high stores. EPO levels are also suppressed by cytokines. Laboratory: normocytic or mild microcytic anemia; ferritin high (acute-phase reactant); serum iron low; TIBC low (distinguishes from true iron deficiency where TIBC is high). — Harrison's 22E, Robbins & Kumar
Step 7 — Bone Marrow Examination
- Unexplained severe anemia
- Abnormal peripheral blood smear morphology suggesting marrow pathology
- Suspected aplastic anemia, MDS, or leukemia
- Circulating nucleated red blood cells
- Myelophthisic picture (teardrop cells + leukoerythroblastosis)
- Staging of lymphoma or certain malignancies
- Macro-ovalocytes with normal B12/folate (suspect MDS)
- Marrow infiltration suspected (myeloma, metastases, granulomas)
Step 8 — Additional Targeted Tests by Clinical Context
| Clinical Suspicion | Additional Tests |
|---|---|
| Pernicious anemia | Anti-intrinsic factor Ab, anti-parietal cell Ab |
| Thalassemia | Hb electrophoresis, α-gene deletion (PCR), family study |
| Hemoglobinopathy | Hb electrophoresis, sickling test |
| PNH | Flow cytometry (CD55, CD59 deficiency) |
| TTP/HUS | ADAMTS13 activity, schistocytes, platelet count, creatinine |
| Lead poisoning | Blood lead level, basophilic stippling on smear |
| Liver disease | LFTs, coagulation panel |
| Hypothyroidism | TSH |
| Myeloma | SPEP, UPEP, serum free light chains, BM biopsy |
| Autoimmune | ANA, RF (underlying connective tissue disease) |
Summary Algorithm
Hemoglobin low?
│
▼
History + Physical → Severity, Symptoms, Clues to Cause
│
▼
CBC + Reticulocyte Count + Peripheral Blood Smear
│
├── Retic ↑ (>100K) ─── Bleeding? ── YES → GI workup, imaging
│ │
│ NO → Hemolysis workup:
│ LDH ↑, Haptoglobin ↓, Indirect bili ↑
│ DAT (Coombs), smear morphology
│ G6PD, Hb electrophoresis, PNH screen
│
└── Retic ↓ / normal ── MCV?
│
┌───────────┼──────────────┐
▼ ▼ ▼
Microcytic Normocytic Macrocytic
(MCV <80) (MCV 80–100) (MCV >100)
│ │ │
Ferritin + Renal Fn, Smear →
Serum Fe + EPO level, Oval macros?
TIBC + TSH, SPEP, → B12/Folate
Hb electro BM if needed Round macros?
RDW → Alcohol/Liver/
(↑ IDA, Thyroid
↓ Thal) Normal B12/folate
+ oval macros?
→ BM (MDS)
Comparison: Iron Deficiency vs. Anemia of Inflammation (Common Clinical Dilemma)
| Feature | Iron Deficiency | Anemia of Inflammation |
|---|---|---|
| Ferritin | ↓ (<15 μg/L) | Normal to ↑ (30–200) |
| Serum iron | ↓ | ↓ |
| TIBC | ↑ (>360) | ↓ (<300) |
| Transferrin sat | <10% | 10–20% |
| Hepcidin | ↓ | ↑ |
| RBC morphology | Micro/hypo | Normocytic or mildly micro |
| Cause | Blood loss, malabsorption, poor intake | Infection, cancer, RA, IBD |
Macrocytic Anemia: B12 vs. Folate vs. MDS
| Feature | B12 Deficiency | Folate Deficiency | MDS |
|---|---|---|---|
| Smear | Oval macrocytes, hyperseg PMNs | Same | Oval macrocytes ± dysplasia |
| Serum B12 | Low (<200 pg/mL) | Normal | Normal |
| Serum folate | Normal | Low | Normal |
| Homocysteine | ↑ | ↑ | Normal |
| Methylmalonic acid (MMA) | ↑ (B12-specific) | Normal | Normal |
| Neurological signs | YES (posterior column) | No | No |
| Bone marrow | Megaloblastic | Megaloblastic | Dysplastic (ringed sideroblasts, etc.) |
Severity Classification
| Severity | Hemoglobin |
|---|---|
| Mild | 10–12 g/dL (women) / 10–13 g/dL (men) |
| Moderate | 8–10 g/dL |
| Severe | 6–8 g/dL |
| Very severe / life-threatening | <6 g/dL |
Key Points
- Reticulocyte count is the single most important test after the CBC — it divides anemia into hyperproliferative (hemolysis/bleeding) vs. hypoproliferative (underproduction).
- Peripheral blood smear is mandatory and often diagnostic without further testing.
- MCV classifies by morphology and drives targeted testing in hypoproliferative anemia.
- RDW distinguishes iron deficiency (high, anisocytosis) from thalassemia (low, uniform cells).
- Ferritin is an acute-phase reactant — it can be normal or high in combined iron deficiency + inflammation.
- Hepcidin is the master iron regulator — elevated in anemia of inflammation; suppressed in iron deficiency.
- Bone marrow biopsy is reserved for unexplained anemia with myelophthisic features, pancytopenia, suspected malignancy, or when initial workup is unrevealing.
- At least 75% of all anemia is hypoproliferative; the most common cause globally is iron deficiency.
Create a single page note taking like image of this content and add infographics and illustrations wherever needed for quick understanding
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or does not exist"
mkdir -p /home/daytona/workspace/anemia-note && python3 -c "from PIL import Image; print('PIL ok')" && python3 -c "import cairo; print('cairo ok')" 2>/dev/null; python3 -c "import reportlab; print('reportlab ok')"
~/anemia-note/generate_note.py
#!/usr/bin/env python3
"""
Anemia – Complete Diagnostic Approach
Single-page note-taking style infographic using Pillow
"""
from PIL import Image, ImageDraw, ImageFont
import math, os, textwrap
# ── Canvas ────────────────────────────────────────────────────────────────────
W, H = 3200, 4800
img = Image.new("RGB", (W, H), "#FAFAF8")
draw = ImageDraw.Draw(img)
# ── Colour palette ────────────────────────────────────────────────────────────
C = {
"bg": "#FAFAF8",
"header_bg": "#1A2B4A", # deep navy
"micro_bg": "#FFF3E0", # warm orange tint
"macro_bg": "#E8F5E9", # green tint
"normo_bg": "#E3F2FD", # blue tint
"hemo_bg": "#FCE4EC", # pink tint
"box_bg": "#FFFFFF",
"border": "#CFD8DC",
"step_blue": "#1565C0",
"step_text": "#FFFFFF",
"navy": "#1A2B4A",
"orange": "#E65100",
"green": "#2E7D32",
"teal": "#00695C",
"red": "#C62828",
"purple": "#6A1B9A",
"text": "#1C1C1E",
"subtext": "#455A64",
"arrow": "#37474F",
"retic_hi": "#D32F2F",
"retic_lo": "#1565C0",
"micro_c": "#E65100",
"macro_c": "#2E7D32",
"normo_c": "#0277BD",
"gold": "#F9A825",
"light_line":"#B0BEC5",
}
# ── Font loader ───────────────────────────────────────────────────────────────
def font(size, bold=False, italic=False):
candidates = []
if bold and italic:
candidates = ["/usr/share/fonts/truetype/dejavu/DejaVuSans-BoldOblique.ttf"]
elif bold:
candidates = ["/usr/share/fonts/truetype/dejavu/DejaVuSans-Bold.ttf",
"/usr/share/fonts/truetype/liberation/LiberationSans-Bold.ttf"]
elif italic:
candidates = ["/usr/share/fonts/truetype/dejavu/DejaVuSans-Oblique.ttf"]
else:
candidates = ["/usr/share/fonts/truetype/dejavu/DejaVuSans.ttf",
"/usr/share/fonts/truetype/liberation/LiberationSans-Regular.ttf"]
for p in candidates:
if os.path.exists(p):
return ImageFont.truetype(p, size)
return ImageFont.load_default()
# ── Drawing helpers ───────────────────────────────────────────────────────────
def rrect(draw, xy, radius=18, fill="#FFF", outline=None, width=2):
x0,y0,x1,y1 = xy
r = radius
draw.rounded_rectangle([x0,y0,x1,y1], radius=r, fill=fill,
outline=outline, width=width)
def text_c(draw, xy, txt, fnt, color="#1C1C1E", anchor="mm"):
draw.text(xy, txt, font=fnt, fill=color, anchor=anchor)
def wrap_text(draw, x, y, txt, fnt, max_w, color="#1C1C1E", line_gap=6, anchor="la"):
words = txt.split()
lines, cur = [], ""
for w in words:
test = (cur + " " + w).strip()
bb = draw.textbbox((0,0), test, font=fnt)
if bb[2]-bb[0] <= max_w:
cur = test
else:
if cur: lines.append(cur)
cur = w
if cur: lines.append(cur)
lh = draw.textbbox((0,0),"Ag",font=fnt)[3] + line_gap
for i,ln in enumerate(lines):
draw.text((x, y+i*lh), ln, font=fnt, fill=color, anchor=anchor)
return y + len(lines)*lh
def arrow(draw, x1,y1,x2,y2, color="#37474F", w=4, head=18):
draw.line([(x1,y1),(x2,y2)], fill=color, width=w)
angle = math.atan2(y2-y1, x2-x1)
for da in [0.45, -0.45]:
ax = x2 - head*math.cos(angle-da)
ay = y2 - head*math.sin(angle-da)
draw.line([(x2,y2),(ax,ay)], fill=color, width=w)
def badge(draw, cx, cy, r, fill, text, fnt, tcol="white"):
draw.ellipse([cx-r,cy-r,cx+r,cy+r], fill=fill)
draw.text((cx,cy), text, font=fnt, fill=tcol, anchor="mm")
def step_pill(draw, x, y, w, h, num, label, bg, fg="white"):
rrect(draw, [x,y,x+w,y+h], radius=h//2, fill=bg)
f_num = font(32, bold=True)
f_lbl = font(28, bold=True)
badge(draw, x+h//2, y+h//2, h//2-4, "#FFFFFF44", str(num), f_num, tcol="white")
draw.text((x+h+14, y+h//2), label, font=f_lbl, fill=fg, anchor="lm")
def divider(draw, y, color="#B0BEC5", pad=60):
draw.line([(pad,y),(W-pad,y)], fill=color, width=2)
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 1 – HEADER
# ═══════════════════════════════════════════════════════════════════════════════
rrect(draw, [0,0,W,170], radius=0, fill=C["header_bg"])
draw.text((W//2, 58), "ANEMIA", font=font(86,bold=True), fill="#FFFFFF", anchor="mm")
draw.text((W//2, 128), "Complete Diagnostic Approach – Stepwise Reference",
font=font(34), fill="#90CAF9", anchor="mm")
# red bar accent
draw.rectangle([0,170,W,182], fill="#EF5350")
# ── Hb normal values strip ──
yy = 196
rrect(draw, [40,yy,W-40,yy+80], radius=14, fill="#E3F2FD", outline="#1565C0", width=2)
vals = [
("Adult ♂", "≥13 g/dL"),
("Adult ♀", "≥12 g/dL"),
("Pregnant", "≥11 g/dL"),
("Child", "≥11 g/dL"),
("Newborn", "17 g/dL"),
]
col_w = (W-80) // len(vals)
for i,(lbl,val) in enumerate(vals):
cx = 40 + i*col_w + col_w//2
draw.text((cx, yy+22), lbl, font=font(24, bold=True), fill=C["step_blue"], anchor="mm")
draw.text((cx, yy+56), val, font=font(28, bold=True), fill=C["red"], anchor="mm")
if i < len(vals)-1:
draw.line([(40+i*col_w+col_w, yy+8),(40+i*col_w+col_w, yy+72)], fill=C["light_line"], width=2)
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 2 – STEPS 1-2 (History + Physical) side by side
# ═══════════════════════════════════════════════════════════════════════════════
y0 = 300
step_pill(draw, 40, y0, 420, 48, 1, "HISTORY", C["step_blue"])
step_pill(draw, 1640, y0, 520, 48, 2, "PHYSICAL EXAM", C["teal"])
# history box
rrect(draw, [40,y0+56,1580,y0+56+260], radius=14, fill="#E8EAF6", outline="#3949AB", width=2)
hist = [
"• Prior anemia, iron pills, transfusions, blood donation",
"• Menstrual hx: duration, pads/clots (premenopausal ♀)",
"• Family hx: hemoglobinopathy, hereditary spherocytosis",
"• Diet: vegan/vegetarian (B12↓), poor diet (folate↓), alcohol",
"• GI: diarrhea (celiac/IBD), melena, NSAID use → occult loss",
"• Meds: chemo, methotrexate, antiseizure, ACE inhibitors",
"• Ethnicity/geography: sickle cell, thalassemia",
]
fy = y0+76
for h in hist:
draw.text((60, fy), h, font=font(24), fill=C["text"]); fy+=34
# physical box
rrect(draw, [1640,y0+56,W-40,y0+56+260], radius=14, fill="#E0F2F1", outline="#00695C", width=2)
phys = [
"• Pallor: conjunctiva, mucosa, nail beds",
"• Tachycardia, flow murmur, dyspnoea",
"• Splenomegaly → hemolysis / lymphoma",
"• Koilonychia, glossitis → iron deficiency",
"• Neuro signs (posterior column) → B12↓",
"• Lymphadenopathy → lymphoma/leukemia",
"• Rectal exam / FOBT → GI blood loss",
]
fy = y0+76
for p in phys:
draw.text((1660, fy), p, font=font(24), fill=C["text"]); fy+=34
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 3 – STEP 3: CBC indices
# ═══════════════════════════════════════════════════════════════════════════════
y0 = 640
step_pill(draw, 40, y0, 620, 48, 3, "CBC + RETICULOCYTE COUNT", C["purple"])
rrect(draw, [40,y0+56,W-40,y0+56+110], radius=14, fill="#F3E5F5", outline="#7B1FA2", width=2)
indices = [
("MCV", "80–100 fL", "Size classification"),
("MCH", "27–33 pg", "Hb per cell"),
("MCHC", "32–36 g/dL","Hb concentration"),
("RDW", "11.5–14.5%","Anisocytosis"),
("Retic","0.5–1.5%", "Marrow output"),
]
cw = (W-80)//len(indices)
for i,(nm,nrm,desc) in enumerate(indices):
cx = 40 + i*cw + cw//2
draw.text((cx, y0+76), nm, font=font(28,bold=True), fill=C["purple"], anchor="mm")
draw.text((cx, y0+106), nrm, font=font(24,bold=True), fill=C["red"], anchor="mm")
draw.text((cx, y0+134), desc, font=font(20), fill=C["subtext"], anchor="mm")
if i < len(indices)-1:
draw.line([(40+i*cw+cw,y0+62),(40+i*cw+cw,y0+154)], fill=C["light_line"], width=2)
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 4 – RETICULOCYTE BRANCH (big infographic)
# ═══════════════════════════════════════════════════════════════════════════════
y0 = 820
step_pill(draw, 40, y0, 820, 48, 4, "RETICULOCYTE COUNT – MASTER BRANCH POINT", C["red"])
# Central retic box
cx_retic = W//2
rrect(draw, [cx_retic-280, y0+60, cx_retic+280, y0+138], radius=20,
fill="#B71C1C", outline="#FFCDD2", width=3)
draw.text((cx_retic, y0+99), "ABSOLUTE RETICULOCYTE COUNT",
font=font(28,bold=True), fill="white", anchor="mm")
# LEFT branch – HIGH
lx = 240
rrect(draw, [40, y0+164, 980, y0+164+90], radius=16,
fill=C["retic_hi"], outline="#EF9A9A", width=3)
draw.text((510, y0+164+30), "RETIC HIGH (>100K/μL)",
font=font(30,bold=True), fill="white", anchor="mm")
draw.text((510, y0+164+62), "Bone marrow IS responding → Loss/Destruction",
font=font(22), fill="#FFCDD2", anchor="mm")
arrow(draw, cx_retic-280, y0+99, 980, y0+164+45, color=C["retic_hi"], w=5)
# RIGHT branch – LOW
rrect(draw, [W-980, y0+164, W-40, y0+164+90], radius=16,
fill=C["retic_lo"], outline="#90CAF9", width=3)
draw.text((W-510, y0+164+30), "RETIC LOW (<50K/μL)",
font=font(30,bold=True), fill="white", anchor="mm")
draw.text((W-510, y0+164+62), "Bone marrow NOT responding → Underproduction",
font=font(22), fill="#BBDEFB", anchor="mm")
arrow(draw, cx_retic+280, y0+99, W-980, y0+164+45, color=C["retic_lo"], w=5)
# Sub-boxes HIGH
yh = y0+280
hboxes = [
("BLEEDING?", "GI loss, menstrual\noccult blood, trauma", "#FF8F00"),
("HEMOLYSIS", "LDH↑, Haptoglobin↓\nIndir. bili↑", "#C62828"),
("IMMUNE", "DAT+ → AIHA\nanti-IgG/complement", "#AD1457"),
("NON-IMMUNE", "G6PD, HS, PNH\nHb electrophoresis", "#6A1B9A"),
]
bw = 930//len(hboxes)
for i,(t,d,col) in enumerate(hboxes):
bx = 40 + i*bw
rrect(draw, [bx, yh, bx+bw-10, yh+110], radius=12, fill=col, outline=None)
draw.text((bx+bw//2-5, yh+26), t, font=font(22,bold=True), fill="white", anchor="mm")
wrap_text(draw, bx+12, yh+44, d, font(19), bw-24, color="#FFECB3")
# Sub-boxes LOW
lboxes = [
("MICROCYTIC\nMCV<80", "Fe def · Thal\nACD · Sideroblastic", C["micro_c"]),
("NORMOCYTIC\nMCV80-100","Renal · Inflam\nAplastic · Endocrine",C["normo_c"]),
("MACROCYTIC\nMCV>100", "B12/Folate def\nAlcohol · MDS", C["macro_c"]),
("BONE MARROW\n(if unclear)", "Aplastic · MDS\nLeukemia · Myeloma","#4A148C"),
]
bw2 = 930//len(lboxes)
for i,(t,d,col) in enumerate(lboxes):
bx = W-980 + i*bw2
rrect(draw, [bx, yh, bx+bw2-10, yh+110], radius=12, fill=col, outline=None)
for j,ln in enumerate(t.split("\n")):
draw.text((bx+bw2//2-5, yh+22+j*26), ln, font=font(21,bold=True), fill="white", anchor="mm")
wrap_text(draw, bx+12, yh+74, d, font(19), bw2-24, color="#FFFFFF")
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 5 – MCV CLASSIFICATION (3 columns)
# ═══════════════════════════════════════════════════════════════════════════════
y0 = 1100
step_pill(draw, 40, y0, 700, 48, 5, "MCV-BASED CLASSIFICATION", C["navy"])
col_w3 = (W-80)//3
titles = ["MICROCYTIC (MCV < 80 fL)", "NORMOCYTIC (MCV 80–100 fL)", "MACROCYTIC (MCV > 100 fL)"]
colors = [C["micro_bg"], C["normo_bg"], C["macro_bg"]]
borders = [C["micro_c"], C["normo_c"], C["macro_c"]]
hdr_cols= [C["micro_c"], C["normo_c"], C["macro_c"]]
micro_content = [
("Iron Deficiency", "Ferritin↓, TIBC↑\nSat <10%, RDW↑"),
("Thalassemia", "Ferritin N/↑, TIBC N\nRDW LOW, Hb electro"),
("Anemia of Inflam.", "Ferritin↑, TIBC↓\nhepcidin↑, Fe↓"),
("Sideroblastic", "Ring sideroblasts\nFe↑, saturation↑"),
]
normo_content = [
("Renal disease", "eGFR<60, EPO↓\nNormocytic, EPO Rx"),
("Anemia of Inflam.", "If early/mild\nCRP/ESR↑"),
("Aplastic anemia", "Pancytopenia\nBM hypocellular"),
("Endocrinopathy", "TSH, cortisol\nHypothyroid/Addison"),
("Marrow invasion", "Teardrops, nRBCs\nBM biopsy"),
]
macro_content = [
("B12 deficiency", "Oval macros\nHyperseg PMNs, MMA↑"),
("Folate deficiency", "Oval macros\nHomocysteine↑"),
("Alcohol/Liver", "Round macros\nLFT abnormal"),
("Hypothyroidism", "Round macros\nTSH↑"),
("MDS", "Oval macros\nNormal B12/folate\n→ BM biopsy"),
]
all_content = [micro_content, normo_content, macro_content]
box_top = y0+56
for col,(title,bg,bord,hc,content) in enumerate(zip(titles,colors,borders,hdr_cols,all_content)):
x0c = 40 + col*col_w3
rrect(draw, [x0c, box_top, x0c+col_w3-12, box_top+580], radius=16, fill=bg, outline=bord, width=3)
# header
rrect(draw, [x0c, box_top, x0c+col_w3-12, box_top+46], radius=14, fill=hc)
draw.text((x0c+(col_w3-12)//2, box_top+23), title, font=font(24,bold=True),
fill="white", anchor="mm")
iy = box_top+60
for (nm,details) in content:
# sub-item
rrect(draw, [x0c+12, iy, x0c+col_w3-24, iy+90], radius=10,
fill="white", outline=bord, width=1)
draw.text((x0c+22, iy+14), "▶ "+nm, font=font(22,bold=True), fill=hc)
wrap_text(draw, x0c+22, iy+40, details, font(19), col_w3-60, color=C["subtext"])
iy += 100
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 6 – IRON STUDIES TABLE + DIFFERENTIAL
# ═══════════════════════════════════════════════════════════════════════════════
y0 = 1730
step_pill(draw, 40, y0, 820, 48, 6, "IRON STUDIES: KEY DIFFERENTIAL", C["orange"])
# table
table_y = y0+60
cols_t = ["TEST", "IRON DEFICIENCY", "ANEMIA OF INFLAM.", "THALASSEMIA", "SIDEROBLASTIC"]
col_ws = [340, 480, 480, 380, 380]
col_xs = [40]
for w in col_ws[:-1]: col_xs.append(col_xs[-1]+w)
# header row
hrow_y = table_y
total_w = sum(col_ws)
rrect(draw, [40, hrow_y, 40+total_w, hrow_y+52], radius=10, fill=C["navy"])
for i,(c,cw,cx) in enumerate(zip(cols_t,col_ws,col_xs)):
draw.text((cx+cw//2, hrow_y+26), c, font=font(22,bold=True), fill="white", anchor="mm")
rows = [
("Smear", "Micro/hypo", "Normal or micro/hypo", "Micro+targeting", "Variable"),
("Serum Fe", "↓ (<30 μg/dL)", "↓ (<50)", "Normal–High", "Normal–High"),
("TIBC", "↑ (>360 μg/dL)", "↓ (<300)", "Normal", "Normal"),
("Sat%", "< 10%", "10–20%", "30–80%", "30–80%"),
("Ferritin", "↓ (<15 μg/L) ⚠", "↑ (30–200)", "↑ (50–300)", "↑ (50–300)"),
("RDW", "↑ HIGH", "Normal", "↓ LOW", "Variable"),
("Hb Electro", "Normal", "Normal", "Abnormal (β-thal)", "Normal"),
]
row_colors = ["#FFF8E1","#FFF3E0","#FFF8E1","#FFF3E0","#FFEBEE","#FFF8E1","#FFF3E0"]
highlight_cols = {"↓ (<15 μg/L) ⚠": "#EF5350", "↑ HIGH":"#E65100", "↓ LOW":"#1565C0",
"< 10%":"#C62828"}
for ri,(row) in enumerate(rows):
ry = table_y + 52 + ri*54
rrect(draw, [40, ry, 40+total_w, ry+54], radius=0, fill=row_colors[ri])
for ci,(cell,cw,cx) in enumerate(zip(row,col_ws,col_xs)):
clr = C["text"]
for k,v in highlight_cols.items():
if k in cell: clr=v; break
fw = font(21,bold=(ci==0))
draw.text((cx+cw//2, ry+27), cell, font=fw, fill=clr, anchor="mm")
draw.line([(40,ry),(40+total_w,ry)], fill=C["light_line"], width=1)
# border around table
draw.rectangle([40, table_y, 40+total_w, table_y+52+len(rows)*54], outline=C["orange"], width=2)
# ferritin note
note_y = table_y + 52 + len(rows)*54 + 10
draw.text((60, note_y), "⚠ Ferritin is an acute-phase reactant — may be falsely NORMAL/HIGH in combined iron deficiency + inflammation. Use sTfR/log ferritin index to distinguish.",
font=font(21,italic=True), fill=C["red"])
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 7 – PERIPHERAL SMEAR MORPHOLOGY TABLE (visual icons)
# ═══════════════════════════════════════════════════════════════════════════════
y0 = 2310
step_pill(draw, 40, y0, 820, 48, 7, "PERIPHERAL BLOOD SMEAR – MORPHOLOGY GUIDE", C["teal"])
morph_data = [
("Microcytic\nHypochromic", "Small cells, large central pallor\n>1/3 diameter", "Iron def · Thalassemia · ACD", "#FF8F00"),
("Macro-ovalocytes\n+ Hyperseg PMNs", "Large oval cells, PMN >5 lobes\n(megaloblastic)", "B12 / Folate deficiency · MDS", "#2E7D32"),
("Spherocytes", "No central pallor\n(sphere, not biconcave disc)", "AIHA · Hereditary spherocytosis", "#C62828"),
("Schistocytes", "Red cell fragments\n(helmet cells, triangles)", "TTP · HUS · DIC · Valve hemolysis", "#AD1457"),
("Sickle cells", "Elongated, crescent-shaped\ncells", "Sickle cell disease (HbSS/HbSC)", "#4A148C"),
("Target cells", "Bulls-eye/shooting-target\nappearance", "Thalassemia · Liver disease · HbC", "#1565C0"),
("Teardrop cells\n+ nRBCs", "Teardrop shape + nucleated RBCs\n+ immature WBCs", "Myelofibrosis · Marrow infiltration", "#37474F"),
("Basophilic\nStippling", "Blue dots in RBCs\n(precipitated ribosomes)", "Thalassemia · Lead poisoning", "#6A1B9A"),
]
cols_m = 4
rows_m = math.ceil(len(morph_data)/cols_m)
bw_m = (W-80)//cols_m
bh_m = 140
my_start = y0+60
for idx,(nm,desc,dx,col) in enumerate(morph_data):
mc = idx % cols_m
mr = idx // cols_m
mx = 40 + mc*bw_m
my = my_start + mr*(bh_m+12)
rrect(draw, [mx, my, mx+bw_m-10, my+bh_m], radius=12, fill="#FFFFFF", outline=col, width=3)
# coloured left accent
draw.rectangle([mx, my, mx+10, my+bh_m], fill=col)
for j,ln in enumerate(nm.split("\n")):
draw.text((mx+22, my+16+j*28), ln, font=font(22,bold=True), fill=col)
wrap_text(draw, mx+22, my+66, desc, font(19), bw_m-50, color=C["subtext"])
wrap_text(draw, mx+22, my+104, "→ "+dx, font(19,italic=True), bw_m-50, color=C["text"])
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 8 – HEMOLYSIS WORKUP
# ═══════════════════════════════════════════════════════════════════════════════
y0 = 2680
step_pill(draw, 40, y0, 620, 48, 8, "HEMOLYSIS WORKUP", C["red"])
hemo_tests = [
("LDH", "↑ (RBC enzyme released)", "#EF5350"),
("Haptoglobin", "↓ (binds free Hb)", "#C62828"),
("Indirect bili","↑ (Hb breakdown)", "#FF8F00"),
("Urine Hb/Hemosidin","+ (intravascular)", "#AD1457"),
("DAT (Coombs)", "+ → immune AIHA", "#1565C0"),
("G6PD assay", "Low → G6PD def", "#2E7D32"),
("Hb electrophoresis","Abnormal → hemoglobinopathy","#6A1B9A"),
("Flow cytometry","CD55/CD59 absent → PNH","#00695C"),
]
bw_h = (W-80)//4
for i,(nm,val,col) in enumerate(hemo_tests):
hx = 40 + (i%4)*bw_h
hy = y0+60 + (i//4)*90
rrect(draw, [hx, hy, hx+bw_h-10, hy+82], radius=12, fill="#FFF",
outline=col, width=2)
draw.rectangle([hx, hy, hx+bw_h-10, hy+8], fill=col)
draw.text((hx+16, hy+18), nm, font=font(22,bold=True), fill=col)
draw.text((hx+16, hy+48), val, font=font(20), fill=C["text"])
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 9 – B12 vs FOLATE vs MDS
# ═══════════════════════════════════════════════════════════════════════════════
y0 = 2940
step_pill(draw, 40, y0, 820, 48, 9, "MACROCYTIC: B12 vs FOLATE vs MDS", C["green"])
macro_cols = ["FEATURE", "B12 DEFICIENCY", "FOLATE DEFICIENCY", "MDS"]
macro_rows = [
("Serum B12", "LOW (<200 pg/mL)", "Normal", "Normal"),
("Serum Folate", "Normal", "LOW", "Normal"),
("Homocysteine", "↑↑", "↑↑", "Normal"),
("MMA", "↑↑ (B12-specific)","Normal", "Normal"),
("Neurology", "YES (post. column)","No", "No"),
("Bone marrow", "Megaloblastic", "Megaloblastic", "Dysplastic\n± ring sideroblasts"),
("Treatment", "B12 IM/oral", "Folic acid oral", "Supportive / azacitidine"),
]
col_ws_m = [380, 520, 520, 460]
col_xs_m = [40];
for w in col_ws_m[:-1]: col_xs_m.append(col_xs_m[-1]+w)
t_total = sum(col_ws_m)
th = y0+60
rrect(draw, [40, th, 40+t_total, th+50], radius=10, fill=C["green"])
for c,cw,cx in zip(macro_cols, col_ws_m, col_xs_m):
draw.text((cx+cw//2, th+25), c, font=font(22,bold=True), fill="white", anchor="mm")
for ri,row in enumerate(macro_rows):
ry = th+50+ri*60
fill = "#F1F8E9" if ri%2==0 else "#FFFFFF"
draw.rectangle([40,ry,40+t_total,ry+60], fill=fill)
for ci,(cell,cw,cx) in enumerate(zip(row,col_ws_m,col_xs_m)):
clr = C["red"] if "LOW" in cell and ci<2 else (C["green"] if ci==0 else C["text"])
if "↑↑" in cell: clr=C["red"]
wrap_text(draw, cx+8, ry+12, cell, font(20,bold=(ci==0)), cw-16, color=clr)
draw.line([(40,ry),(40+t_total,ry)], fill=C["light_line"],width=1)
draw.rectangle([40,th,40+t_total,th+50+len(macro_rows)*60], outline=C["green"],width=2)
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 10 – BONE MARROW INDICATIONS
# ═══════════════════════════════════════════════════════════════════════════════
y0 = 3400
step_pill(draw, 40, y0, 620, 48, 10, "BONE MARROW BIOPSY – INDICATIONS", "#4A148C")
bm_indications = [
"Unexplained severe / refractory anemia",
"Pancytopenia",
"Myelophthisic picture (teardrops + nRBCs + leukoerythroblastosis)",
"Macro-ovalocytes with normal B12 / folate → suspect MDS",
"Suspected aplastic anemia",
"Staging of lymphoma, myeloma, other malignancies",
"Unexplained circulating blasts or nucleated RBCs",
]
rrect(draw, [40, y0+60, W//2-20, y0+60+270], radius=14, fill="#EDE7F6", outline="#4A148C", width=2)
for i,ind in enumerate(bm_indications):
draw.text((70, y0+84+i*36), f"{'①②③④⑤⑥⑦'[i]} {ind}", font=font(22), fill=C["text"])
# BM findings box
rrect(draw, [W//2+20, y0+60, W-40, y0+60+270], radius=14, fill="#EDE7F6", outline="#4A148C", width=2)
draw.text((W//2+40, y0+82), "BM FINDINGS:", font=font(24,bold=True), fill="#4A148C")
bm_finds = [
("Hypocellular marrow", "→ Aplastic anemia"),
("Absent erythroid precursors","→ Pure red cell aplasia"),
("Ring sideroblasts", "→ Sideroblastic anemia / MDS"),
("Megaloblasts", "→ B12/Folate (if not treated)"),
("Fibrosis + teardrops", "→ Myelofibrosis"),
("Blasts >20%", "→ Acute leukemia (AML/ALL)"),
]
for i,(f,r) in enumerate(bm_finds):
fy2 = y0+114+i*34
draw.text((W//2+50, fy2), f"• {f}", font=font(21), fill=C["text"])
draw.text((W//2+50+450, fy2), r, font=font(21,bold=True), fill="#4A148C")
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 11 – SEVERITY BOX
# ═══════════════════════════════════════════════════════════════════════════════
y0 = 3720
rrect(draw, [40, y0, W-40, y0+100], radius=16, fill="#263238", outline="#37474F", width=2)
draw.text((W//2, y0+20), "SEVERITY CLASSIFICATION", font=font(26,bold=True), fill="#80CBC4", anchor="mm")
sev = [("MILD","10–12 g/dL","#4CAF50"),("MODERATE","8–10 g/dL","#FF9800"),
("SEVERE","6–8 g/dL","#F44336"),("LIFE-THREATENING","<6 g/dL","#B71C1C")]
sw = (W-80)//len(sev)
for i,(nm,rng,col) in enumerate(sev):
sx = 40 + i*sw + sw//2
draw.text((sx, y0+55), nm, font=font(24,bold=True), fill=col, anchor="mm")
draw.text((sx, y0+82), rng, font=font(22), fill="#ECEFF1",anchor="mm")
if i<len(sev)-1:
draw.line([(40+i*sw+sw, y0+30),(40+i*sw+sw, y0+95)], fill="#546E7A", width=2)
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 12 – ALGORITHM FLOWCHART (central visual)
# ═══════════════════════════════════════════════════════════════════════════════
y0 = 3860
step_pill(draw, 40, y0, 620, 48, 11, "DIAGNOSTIC ALGORITHM", C["navy"])
# flowchart nodes
def flow_box(draw, cx, cy, w, h, text, fill, text_col="white", fsize=22, radius=14):
rrect(draw, [cx-w//2, cy-h//2, cx+w//2, cy+h//2], radius=radius, fill=fill)
lines = text.split("\n")
lh = fsize+6
ty = cy - (len(lines)-1)*lh//2
for ln in lines:
draw.text((cx, ty), ln, font=font(fsize, bold=True), fill=text_col, anchor="mm")
ty += lh
def diamond(draw, cx, cy, w, h, text, fill, text_col="white"):
pts = [(cx,cy-h//2),(cx+w//2,cy),(cx,cy+h//2),(cx-w//2,cy)]
draw.polygon(pts, fill=fill)
draw.polygon(pts, outline="#FFFFFF", width=2)
draw.text((cx, cy), text, font=font(21,bold=True), fill=text_col, anchor="mm")
fa = y0+68
# Start
flow_box(draw, W//2, fa, 600, 50, "LOW HEMOGLOBIN (CBC)", C["navy"], fsize=24)
arrow(draw, W//2, fa+25, W//2, fa+80, color=C["arrow"], w=4)
# Smear + retic
flow_box(draw, W//2, fa+100, 700, 50, "Peripheral Blood Smear + Reticulocyte Count", C["teal"], fsize=22)
arrow(draw, W//2, fa+125, W//2, fa+175, color=C["arrow"], w=4)
# Diamond retic
diamond(draw, W//2, fa+210, 580, 90, "RETIC HIGH?", C["red"])
# YES left
arrow(draw, W//2-290, fa+210, W//2-560, fa+210, color=C["retic_hi"], w=4)
flow_box(draw, W//2-700, fa+210, 300, 60, "BLEEDING\nor\nHEMOLYSIS", C["retic_hi"], fsize=20)
# NO right
arrow(draw, W//2+290, fa+210, W//2+560, fa+210, color=C["retic_lo"], w=4)
flow_box(draw, W//2+700, fa+210, 300, 60, "UNDER-\nPRODUCTION", C["retic_lo"], fsize=20)
# down arrow to MCV
arrow(draw, W//2, fa+255, W//2, fa+310, color=C["arrow"], w=4)
diamond(draw, W//2, fa+345, 400, 80, "MCV?", C["purple"])
# micro
arrow(draw, W//2-200, fa+345, W//2-560, fa+345, color=C["micro_c"], w=4)
flow_box(draw, W//2-700, fa+345, 300, 60, "< 80 fL\nMICROCYTIC", C["micro_c"], fsize=20)
arrow(draw, W//2-700, fa+375, W//2-700, fa+430, color=C["micro_c"], w=3)
flow_box(draw, W//2-700, fa+465, 300, 60, "Ferritin · Fe ·\nTIBC · RDW\nHb Electro", C["micro_c"], fsize=18)
# normo
arrow(draw, W//2, fa+385, W//2, fa+430, color=C["normo_c"], w=4)
flow_box(draw, W//2, fa+465, 300, 60, "80–100 fL\nNORMOCYTIC", C["normo_c"], fsize=20)
arrow(draw, W//2, fa+495, W//2, fa+540, color=C["normo_c"], w=3)
flow_box(draw, W//2, fa+580, 300, 80, "eGFR · EPO\nTSH · SPEP\nBM biopsy?", C["normo_c"], fsize=18)
# macro
arrow(draw, W//2+200, fa+345, W//2+560, fa+345, color=C["macro_c"], w=4)
flow_box(draw, W//2+700, fa+345, 300, 60, "> 100 fL\nMACROCYTIC", C["macro_c"], fsize=20)
arrow(draw, W//2+700, fa+375, W//2+700, fa+430, color=C["macro_c"], w=3)
flow_box(draw, W//2+700, fa+465, 300, 60, "B12 · Folate\nTSH · LFTs\nBM if normal", C["macro_c"], fsize=18)
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 13 – KEY PEARLS
# ═══════════════════════════════════════════════════════════════════════════════
y0 = 4620
rrect(draw, [40, y0, W-40, y0+120], radius=16, fill="#1A237E", outline="#3F51B5", width=2)
draw.text((W//2, y0+22), "⚡ KEY DIAGNOSTIC PEARLS",
font=font(30,bold=True), fill="#FFD54F", anchor="mm")
pearls = [
"Retic count = Master branch point",
"Ferritin <15 = Iron-depleted stores",
"RDW HIGH + micro = IDA | RDW LOW + micro = Thalassemia",
"Haptoglobin LOW = Hemolysis",
"Hyperseg PMNs + oval macros = Megaloblastic",
"MMA↑ (normal folate) = B12-specific",
"Teardrops + nRBCs = Myelophthisic → Bone marrow biopsy",
"≥75% anemia = Hypoproliferative",
]
px = 60; py = y0+52
for i,p in enumerate(pearls):
col = "#FFD54F" if i%2==0 else "#80CBC4"
draw.text((px, py), f"✦ {p}", font=font(21), fill=col)
px += (W-80)//4
if (i+1)%4==0: px=60; py+=36
# ═══════════════════════════════════════════════════════════════════════════════
# FOOTER
# ═══════════════════════════════════════════════════════════════════════════════
rrect(draw, [0,H-52,W,H], radius=0, fill=C["navy"])
draw.text((W//2, H-26),
"Harrison's 22E (2025) | Robbins & Kumar Pathologic Basis of Disease | Goldman-Cecil Medicine | Tintinalli's Emergency Medicine",
font=font(20), fill="#90CAF9", anchor="mm")
# ── Save ──────────────────────────────────────────────────────────────────────
out = "/home/daytona/workspace/anemia-note/Anemia_Diagnostic_Note.png"
img.save(out, "PNG", dpi=(200,200))
print(f"Saved → {out}")
print(f"Size: {W}x{H}px")
cd /home/daytona/workspace/anemia-note && python3 generate_note.py 2>&1
python3 -c " from PIL import Image img = Image.open('/home/daytona/workspace/anemia-note/Anemia_Diagnostic_Note.png') print('Size:', img.size, 'Mode:', img.mode) # make a preview thumbnail thumb = img.copy() thumb.thumbnail((800, 1200)) thumb.save('/home/daytona/workspace/anemia-note/preview.png') print('Preview saved') "
python3 -c " from PIL import Image import base64, sys img = Image.open('/home/daytona/workspace/anemia-note/preview.png') print(img.size) # encode and print first 200 chars to confirm import io buf = io.BytesIO() img.save(buf, 'PNG') b64 = base64.b64encode(buf.getvalue()).decode() print('b64 length:', len(b64)) "
ls -lh /home/daytona/workspace/anemia-note/
Anemia Diagnostic Note
Image · PNG
| # | Section | Visual Style |
|---|---|---|
| 1 | Header + Normal Hb values | Deep navy banner with colour-coded reference strip |
| 2 | History + Physical Exam | Side-by-side tinted panels |
| 3 | CBC Indices | Quick-reference bar with normal ranges |
| 4 | Reticulocyte Count – Master Branch Point | Central red diamond → High (red) / Low (blue) branches with sub-boxes |
| 5 | MCV Classification | 3-column colour-coded grid (micro/normo/macro) with cause + test per entry |
| 6 | Iron Studies Differential Table | 5-column table (IDA vs AoI vs Thal vs Sideroblastic) with red highlights |
| 7 | Peripheral Smear Morphology Guide | 8 morphology tiles with coloured left-accent and → diagnosis |
| 8 | Hemolysis Workup | 8 test cards (LDH, haptoglobin, DAT, G6PD, PNH screen, etc.) |
| 9 | B12 vs Folate vs MDS Table | 7-row differential with MMA/homocysteine row highlighted |
| 10 | Bone Marrow – Indications + Findings | Split box (when to do it / what it shows) |
| 11 | Diagnostic Algorithm Flowchart | Full flowchart: Hb↓ → Smear+Retic → Retic branch → MCV branch → Tests |
| — | Key Pearls footer | Dark navy strip with 8 high-yield memory anchors |
Create a single page note taking like image of this content and add infographics and illustrations wherever needed for quick understanding (Use generate poster tool)
Single-page medical note-taking style reference poster titled "ANEMIA – Complete Diagnostic Approach (Stepwise)". Dark navy and white clinical design with color-coded sections. Include: TOP HEADER: Bold title "ANEMIA – Complete Diagnostic Approach" in deep navy banner. Below: Normal Hb values strip showing Adult Male ≥13 g/dL, Adult Female ≥12 g/dL, Pregnant ≥11 g/dL, Child ≥11 g/dL in colored badges. STEP 1 – HISTORY & PHYSICAL (two side-by-side boxes): Left box (blue): History bullets: prior anemia/transfusions, menstrual history (clots, pads), family hx hemoglobinopathy, dietary hx (vegan=B12↓), GI symptoms/NSAIDs, alcohol, medications, ethnicity (sickle cell/thal). Right box (teal): Physical Exam bullets: conjunctival/mucosal pallor, tachycardia, splenomegaly→hemolysis, koilonychia+glossitis→iron def, neurological signs→B12 def, lymphadenopathy, rectal exam/FOBT. STEP 2 – CBC INDICES: Horizontal strip showing MCV (80–100 fL), MCH (27–33 pg), MCHC (32–36 g/dL), RDW (11.5–14.5%), Reticulocyte (0.5–1.5%) in colored badge boxes. STEP 3 – RETICULOCYTE MASTER BRANCH (central infographic diamond): Large red diamond labeled "RETICULOCYTE COUNT?" in center. LEFT arrow → RED box: "RETIC HIGH >100K → Hemolysis/Bleeding" with sub-boxes: Bleeding?, AIHA (DAT+), Non-immune hemolysis (G6PD/HS/PNH), LDH↑ Haptoglobin↓ Bili↑ RIGHT arrow → BLUE box: "RETIC LOW → Underproduction" with sub-boxes: Microcytic (IDA/Thal), Normocytic (Renal/Aplastic), Macrocytic (B12/Folate/MDS) STEP 4 – MCV CLASSIFICATION (3 colored columns): Orange column "MICROCYTIC MCV<80": Iron Def (ferritin↓ TIBC↑ RDW↑), Thalassemia (RDW↓ Hb electro), ACD (ferritin↑ TIBC↓ hepcidin↑), Sideroblastic (ring sideroblasts) Blue column "NORMOCYTIC MCV 80-100": Renal disease (EPO↓), Aplastic anemia (pancytopenia BM hypocellular), Endocrinopathy (TSH), Marrow invasion (teardrops+nRBCs) Green column "MACROCYTIC MCV>100": B12 def (MMA↑ neuro signs), Folate def (homocysteine↑), Alcohol/Liver (round macros), MDS (BM biopsy) STEP 5 – IRON STUDIES TABLE (color-highlighted): 5-column table: Test | Iron Deficiency | Anemia of Inflammation | Thalassemia | Sideroblastic Rows: Serum Fe, TIBC, Sat%, Ferritin, RDW, Hb Electro Key highlights: Ferritin <15=IDA (red), TIBC >360=IDA (orange), RDW HIGH=IDA, RDW LOW=Thal (blue) Footer note: ⚠ Ferritin is acute-phase reactant – may be falsely normal in combined IDA + inflammation STEP 6 – PERIPHERAL SMEAR MORPHOLOGY (8 illustrated tiles in 2 rows): Each tile has colored left border, name, description, and → diagnosis: 1. Microcytic/Hypochromic → Iron def/Thal/ACD 2. Macro-ovalocytes + Hyperseg PMNs → B12/Folate/MDS 3. Spherocytes (no central pallor) → AIHA/Hereditary spherocytosis 4. Schistocytes (helmet cells) → TTP/HUS/DIC/Valve 5. Sickle cells (crescent) → HbSS sickle cell disease 6. Target cells (bull's-eye) → Thal/Liver/HbC 7. Teardrop cells + nRBCs → Myelofibrosis/Myelophthisic 8. Basophilic stippling → Thal/Lead poisoning STEP 7 – HEMOLYSIS WORKUP (8 test cards in grid): LDH ↑, Haptoglobin ↓, Indirect bili ↑, Urine Hb/hemosiderin +, DAT+ → AIHA, G6PD assay low → G6PD def, Hb electrophoresis abnormal, Flow cytometry CD55/CD59 absent → PNH STEP 8 – MACROCYTIC DIFFERENTIAL TABLE: Feature | B12 Deficiency | Folate Deficiency | MDS B12: LOW / Normal / Normal Folate: Normal / LOW / Normal MMA: ↑↑ / Normal / Normal Neurology: YES / No / No BM: Megaloblastic / Megaloblastic / Dysplastic STEP 9 – DIAGNOSTIC ALGORITHM FLOWCHART (bottom center): Box: "Hb LOW" → Box: "PBS + Retic Count" → Diamond: "Retic HIGH?" → Yes: Hemolysis/Bleeding workup → No: Diamond "MCV?" → 3 branches: <80 Microcytic (Ferritin/TIBC/RDW), 80-100 Normocytic (eGFR/EPO/TSH), >100 Macrocytic (B12/Folate/BM) STEP 10 – BONE MARROW INDICATIONS (two boxes): Left: Indications: unexplained severe anemia, pancytopenia, teardrops+nRBCs, oval macros + normal B12/folate, suspected aplastic, staging lymphoma/myeloma Right: BM findings: hypocellular→aplastic, ring sideroblasts→MDS, megaloblasts→B12/folate, fibrosis+teardrops→myelofibrosis, blasts >20%→AML SEVERITY BAND: Mild 10-12 (green) | Moderate 8-10 (orange) | Severe 6-8 (red) | Life-threatening <6 g/dL (dark red) KEY PEARLS FOOTER (dark navy): ✦ Retic count = master branch point ✦ Ferritin <15 = iron depleted ✦ RDW HIGH+micro=IDA, RDW LOW+micro=Thal ✦ Haptoglobin LOW = hemolysis ✦ Hyperseg PMNs + oval macros = megaloblastic ✦ MMA↑ normal folate = B12-specific ✦ Teardrops+nRBCs = myelophthisic → BM biopsy ✦ 75% anemia is hypoproliferative Sources: Harrison's 22E (2025) | Robbins & Kumar | Goldman-Cecil Medicine | Tintinalli's Emergency Medicine Clean medical infographic style, professional color coding, well-organized layout, all text legible, suitable for medical students and clinicians.
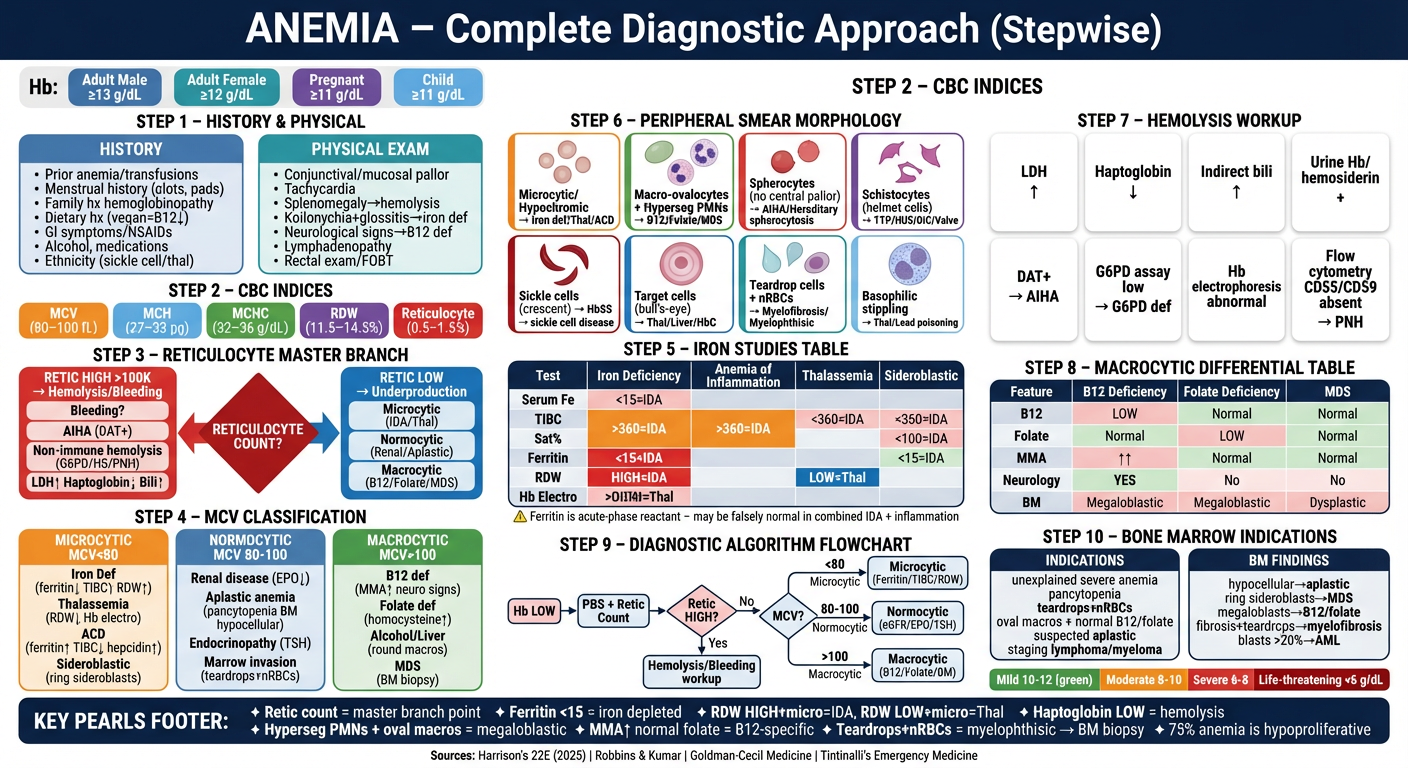
- Header — title + normal Hb reference values by population
- Steps 1–2 — History & Physical Exam side-by-side
- Step 3 — CBC indices quick-reference bar
- Step 4 — Reticulocyte count master branch diamond (High → Hemolysis/Bleeding | Low → Underproduction)
- Step 5 — MCV 3-column classification (Microcytic / Normocytic / Macrocytic) with causes and tests
- Step 6 — Iron studies differential table (IDA vs ACD vs Thal vs Sideroblastic) with key highlights
- Step 7 — Peripheral smear morphology tiles (8 RBC abnormalities → diagnoses)
- Step 8 — Hemolysis workup grid (LDH, haptoglobin, DAT, G6PD, PNH screen)
- Step 9 — B12 vs Folate vs MDS differential table
- Step 10 — Diagnostic algorithm flowchart + Bone marrow indications
- Footer — Severity band + 8 high-yield pearls