Brachial plexus
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Here is a thorough overview of the Brachial Plexus based on Gray's Anatomy for Students and Miller's Review of Orthopaedics.
Brachial Plexus
Overview
The brachial plexus is a somatic nerve plexus formed by the anterior rami of C5 to C8 and most of T1. It originates in the neck, passes laterally and inferiorly over rib I, and enters the axilla. All major nerves innervating the upper limb originate from it.
- Gray's Anatomy for Students, p. 858
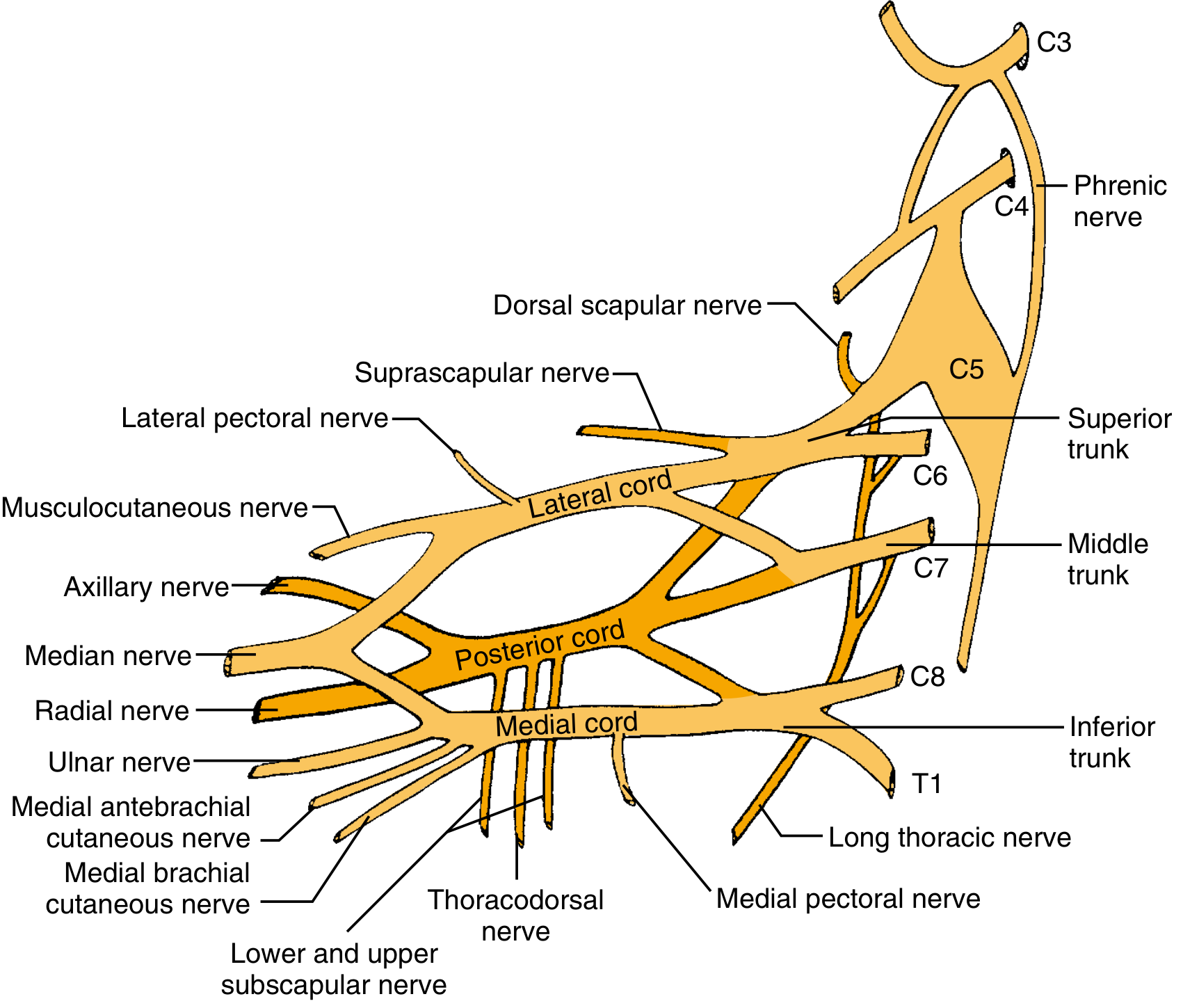
Structure: Roots → Trunks → Divisions → Cords → Branches
The classic mnemonic is "Robert Taylor Drinks Cold Beer" (Roots, Trunks, Divisions, Cords, Branches).

1. Roots (Anterior Rami)
| Root | Contribution |
|---|---|
| C5 | Superior trunk (with C6) |
| C6 | Superior trunk (with C5) |
| C7 | Middle trunk (alone) |
| C8 | Inferior trunk (with T1) |
| T1 | Inferior trunk (with C8) |
- Roots lie between anterior and middle scalene muscles, behind the subclavian artery.
- Each root receives gray rami communicantes from the sympathetic trunk, carrying postganglionic sympathetic fibers.
Branches from roots:
- Dorsal scapular nerve (C5) - rhomboid major and minor
- Long thoracic nerve (C5, C6, C7) - serratus anterior
- Small contribution to the phrenic nerve (C5)
2. Trunks
| Trunk | Formed By | Position |
|---|---|---|
| Superior | C5 + C6 | Superior |
| Middle | C7 alone | Middle |
| Inferior | C8 + T1 | Lies on rib I, posterior to subclavian artery |
Branches from trunks (only from the superior trunk):
- Suprascapular nerve (C5, C6) - supraspinatus and infraspinatus
- Nerve to subclavius (C5, C6) - subclavius muscle
3. Divisions
Each trunk divides into an anterior and posterior division:
- Anterior divisions → eventually supply the flexor (anterior) compartments
- Posterior divisions → eventually supply the extensor (posterior) compartments
- No peripheral nerves arise directly from divisions.
4. Cords (named by relation to the 2nd part of the axillary artery)
| Cord | Origin | Roots | Position |
|---|---|---|---|
| Lateral | Anterior divisions of superior + middle trunks | C5-C7 | Lateral to axillary artery |
| Medial | Anterior division of inferior trunk | C8-T1 | Medial to axillary artery |
| Posterior | All three posterior divisions | C5-T1 | Posterior to axillary artery |
5. Terminal Branches
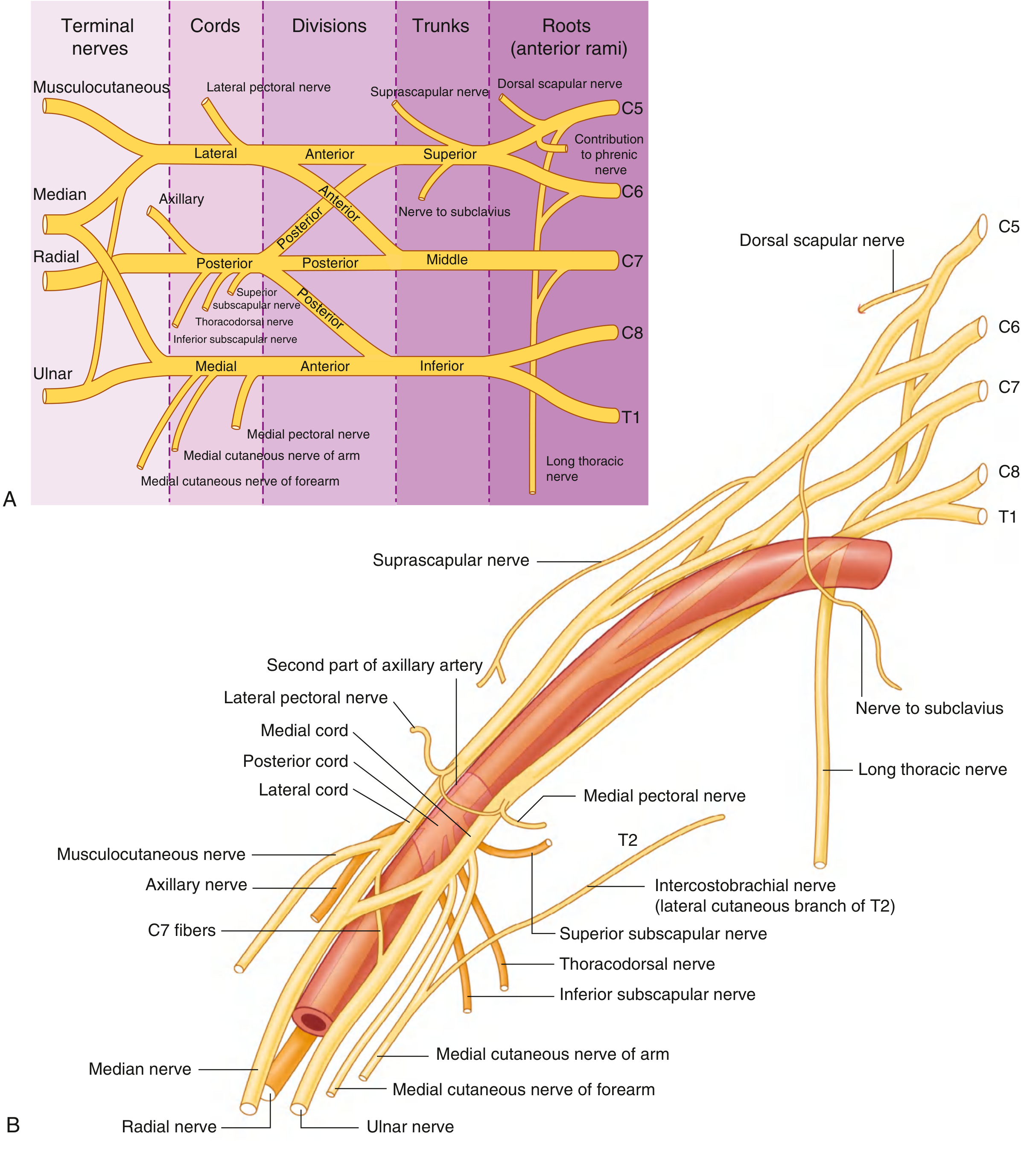
From the Lateral Cord:
- Lateral pectoral nerve - pectoralis major
- Musculocutaneous nerve (C5-C7) - coracobrachialis, biceps, brachialis; becomes lateral cutaneous nerve of forearm
- Lateral root of the median nerve
From the Medial Cord:
- Medial pectoral nerve - pectoralis minor (and minor)
- Medial cutaneous nerve of the arm
- Medial cutaneous nerve of the forearm
- Ulnar nerve (C8-T1)
- Medial root of the median nerve
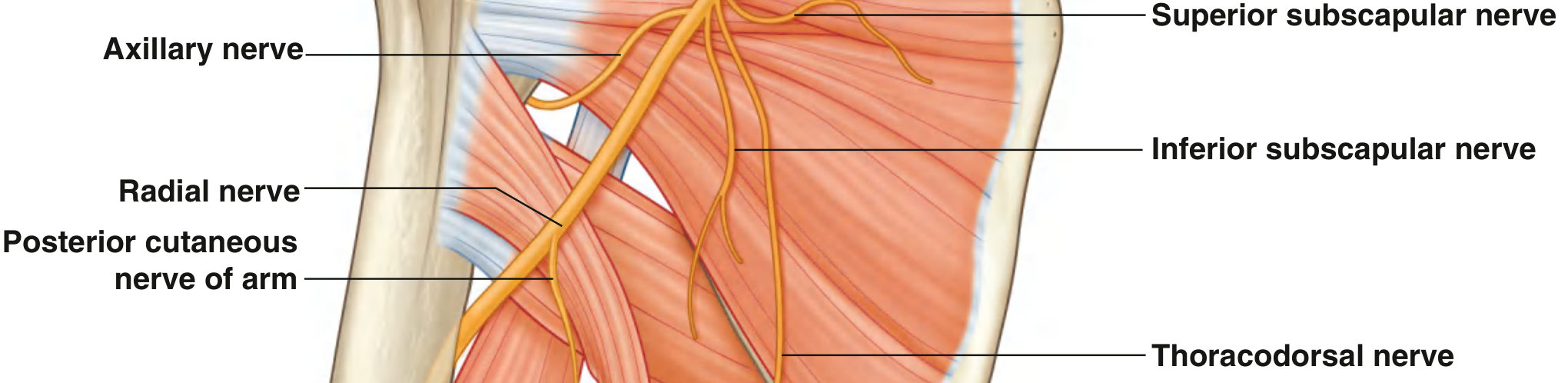
From the Posterior Cord:
- Upper subscapular nerve - subscapularis
- Thoracodorsal nerve - latissimus dorsi
- Lower subscapular nerve - subscapularis and teres major
- Axillary nerve (C5-C6) - deltoid and teres minor
- Radial nerve (C5-T1) - all posterior compartment muscles of arm and forearm
Note: The median nerve (C5-T1) is formed from contributions of both the lateral and medial cords.
Clinical Injuries
Supraclavicular vs. Infraclavicular Lesions
Brachial plexus injuries are classified as preganglionic (avulsion) or postganglionic. Preganglionic injuries have the worst prognosis because the cell body is intact but the nerve root is avulsed from the spinal cord.
Clues to preganglionic injury:
- Horner syndrome (ptosis, miosis, anhidrosis) - sympathetic chain involvement
- Winged scapula - long thoracic nerve involvement
- Weak rhomboids - dorsal scapular nerve involvement
- Normal sensory nerve action potentials (SNAPs) despite sensory loss on exam (cell bodies in dorsal root ganglia are intact)
- EMG: denervation of paraspinal muscles
- Elevated hemidiaphragm (phrenic nerve involvement)
- Miller's Review of Orthopaedics, p. 697-698
Common Injury Patterns
| Pattern | Roots | Mechanism | Classic Deficit |
|---|---|---|---|
| Erb's palsy (upper trunk) | C5-C6 | Downward traction on shoulder; obstetric | "Waiter's tip" - arm adducted, IR, elbow extended, forearm pronated |
| Klumpke's palsy (lower trunk) | C8-T1 | Upward traction on arm | Intrinsic hand muscles, + Horner if T1 root avulsed |
| Burners/Stingers | Upper plexus | Football - compression at Erb's point | Transient burning pain, unilateral only |
| Obstetric brachial plexopathy | Variable | Shoulder dystocia, forceps delivery | Variable; high birth weight risk factor |
Investigations
- CT myelography - detects nerve root avulsions (pseudomeningoceles)
- MRI - peripheral neuroma, mass lesions
- EMG/NCS - extent of denervation; must be done 4-6 weeks post-injury (Wallerian degeneration)
- SNAPs - normal in preganglionic lesions despite clinical sensory loss
- Chest X-ray (inspiratory + expiratory) - elevated hemidiaphragm = phrenic nerve involvement
- Cervical spine X-ray: transverse process fracture suggests root avulsion
Treatment
| Timing | Indication |
|---|---|
| Immediate | Penetrating trauma, iatrogenic injury, vascular injury, progressive deficits |
| 3-12 weeks | Incomplete/near-complete injury from high-energy mechanism |
| 3-6 months | Incomplete upper plexus lesion from low-energy; plateau in recovery |
| >6 months | Less predictable; muscle fibrosis begins at 18-24 months |
Key surgical options:
- Neuroma excision + cable grafting (sural nerve, medial brachial/antebrachial cutaneous nerves as donors)
- Nerve transfers when insufficient proximal axons (avulsions):
- Oberlin transfer: ulnar nerve fascicle to FCU → musculocutaneous nerve (restores elbow flexion)
- Spinal accessory (CN XI) → suprascapular nerve (shoulder abduction)
- Triceps branch of radial nerve → axillary nerve (Leechavengvong procedure)
- Priorities: elbow flexion > shoulder stabilization > hand function
- Best results in young patients treated within 3 months
- Miller's Review of Orthopaedics, pp. 697-699
Obstetric Brachial Plexopathy (neonatal)
- Risk factors: high birth weight, cephalopelvic disproportion, shoulder dystocia, forceps delivery
- Good prognosis: biceps + deltoid = M1 by 2 months → complete recovery possible
- Poor prognosis: no biceps contraction by 3-6 months
- Nerve grafting results are better in infants than adults; hand intrinsic reinnervation is possible
Proceed
Asking for Preferences
Brachial plexus
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, exam-focused anatomy of the brachial plexus - roots to terminal branches.
Brachial Plexus - Full Anatomy (Exam Prep)
The Big Picture
The brachial plexus forms from anterior rami of C5-T1, originates between the anterior and middle scalene muscles in the neck, crosses rib I, and enters the axilla to supply the entire upper limb.
Mnemonic for structure: Robert Taylor Drinks Cold Beer = Roots, Trunks, Divisions, Cords, Branches
Complete Schematic
Step 1: Roots (Anterior Rami)
The roots lie between the anterior scalene and middle scalene muscles, posterior to the subclavian artery. They receive gray rami communicantes from the sympathetic trunk.
| Root | Joins to Form |
|---|---|
| C5 + C6 | Superior (upper) trunk |
| C7 | Middle trunk (alone) |
| C8 + T1 | Inferior (lower) trunk |
Branches off the roots (pre-trunk):
| Nerve | Root Origin | Muscle Supplied | Exam Clue |
|---|---|---|---|
| Dorsal scapular nerve | C5 | Rhomboid major + minor, levator scapulae | Medial scapular winging |
| Long thoracic nerve | C5, C6, C7 | Serratus anterior | Lateral/anterior scapular winging ("wings" on push-up) |
| Contribution to phrenic | C5 (small) | Diaphragm | Elevated hemidiaphragm = root avulsion clue |
Mnemonic for long thoracic: C5, 6, 7 keep the wing off heaven (serratus anterior keeps scapula flat)
Step 2: Trunks
Trunks cross the posterior triangle of the neck and the base of rib I.
Branches off the trunks (only from the superior trunk):
| Nerve | Root | Supplies | Lesion |
|---|---|---|---|
| Suprascapular nerve | C5, C6 | Supraspinatus + infraspinatus | Passes through suprascapular foramen; ganglion here causes isolated infraspinatus/supraspinatus wasting |
| Nerve to subclavius | C5, C6 | Subclavius | Rarely clinically significant |
Step 3: Divisions
Each trunk splits into an anterior and a posterior division - 6 divisions total. No branches arise from divisions. This is the crossroads that separates flexor-supply from extensor-supply.
- Anterior divisions → Lateral + Medial cords (supply flexor/anterior compartments)
- Posterior divisions → Posterior cord (supply extensor/posterior compartments)
Step 4: Cords (named by position relative to the 2nd part of the axillary artery)
| Cord | Formed From | Roots | Position |
|---|---|---|---|
| Lateral | Ant. div. superior + middle trunks | C5-C7 | Lateral to axillary artery |
| Medial | Ant. div. inferior trunk | C8-T1 | Medial to axillary artery |
| Posterior | All 3 posterior divisions | C5-T1 | Posterior to axillary artery |
Step 5: Branches (Terminal + Collateral)
From the Lateral Cord (C5-C7)
| Branch | Root Values | Motor Supply | Sensory Supply |
|---|---|---|---|
| Lateral pectoral nerve | C5-C7 | Pectoralis major (primarily) | None |
| Musculocutaneous nerve | C5-C7 | Coracobrachialis, biceps brachii, brachialis | Lateral forearm (as lateral cutaneous nerve of forearm) |
| Lateral root of median nerve | C5-C7 | - contributes to median nerve - | - |
The musculocutaneous nerve pierces coracobrachialis, runs between biceps and brachialis, and becomes the lateral cutaneous nerve of the forearm. Loss = weak elbow flexion + supination; sensory loss over lateral forearm.
From the Medial Cord (C8-T1)
| Branch | Root Values | Motor Supply | Sensory Supply |
|---|---|---|---|
| Medial pectoral nerve | C8-T1 | Pectoralis minor + major | None |
| Medial cutaneous nerve of arm | C8-T1 | None | Medial arm (lower 1/3) |
| Medial cutaneous nerve of forearm | C8-T1 | None | Medial forearm to wrist |
| Ulnar nerve | C8-T1 | FCU, medial FDP, all intrinsics except 3 thenar + 2 lateral lumbricals | Little finger, medial ring finger (palm + dorsum) |
| Medial root of median nerve | C8-T1 | - contributes to median nerve - | - |
From the Posterior Cord (C5-T1)
| Branch | Root Values | Motor Supply | Exam Clue |
|---|---|---|---|
| Superior subscapular nerve | C5-C6 | Subscapularis (upper) | - |
| Thoracodorsal nerve | C6-C8 | Latissimus dorsi | "Cough impulse" test for lat dorsi |
| Inferior subscapular nerve | C5-C6 | Subscapularis (lower) + teres major | - |
| Axillary nerve | C5-C6 | Deltoid + teres minor; cutaneous over "regimental badge" area | Exits via quadrangular space; damaged in shoulder dislocation or surgical neck # |
| Radial nerve | C5-T1 | ALL posterior arm + forearm muscles (triceps, brachioradialis, ECRL, ECRB, supinator, extensors) | Exits via triangular interval with profunda brachii; wrist drop with mid-shaft humerus # |
The Median Nerve - Special Case
The median nerve (C5-T1) is unique - it is formed by contributions from both the lateral cord (C5-C7) and medial cord (C8-T1), uniting anterior to the third part of the axillary artery. It supplies:
- Motor: All anterior forearm muscles except FCU and medial FDP; thenar muscles (LOAF - lateral 2 lumbricals, Opponens pollicis, Abductor pollicis brevis, Flexor pollicis brevis)
- Sensory: Lateral 3.5 fingers on palm side; lateral palm
Quick Cord-to-Branch Summary Table
| Cord | Branches | Memory Aid |
|---|---|---|
| Lateral | Lateral pectoral, Musculocutaneous, Lateral root median | "LML" |
| Medial | Medial pectoral, Med. cut. arm, Med. cut. forearm, Ulnar, Medial root median | "My Aunt Mabel Ulcerates" |
| Posterior | Upper subscapular, Thoracodorsal, Lower subscapular, Axillary, Radial | "STAR" = Subscapular (×2), Thoracodorsal, Axillary, Radial |
Injury Level - What to Expect
| Level Injured | Common Cause | Key Deficit |
|---|---|---|
| Roots (preganglionic avulsion) | High-energy motorcycle crash | Horner's syndrome, winged scapula, normal SNAPs but no sensation |
| Superior trunk (C5-C6) - Erb's | Traction on neck/shoulder; obstetric | "Waiter's tip" - arm IR, adducted, elbow extended, forearm pronated. Weak deltoid, biceps, brachioradialis |
| Inferior trunk (C8-T1) - Klumpke's | Upward arm traction; Pancoast tumour | Intrinsic hand weakness; claw hand; Horner's if T1 root avulsed |
| Posterior cord | Anterior shoulder dislocation | Axillary + radial nerve palsy - deltoid weakness + wrist drop |
| Lateral cord | Clavicle # | Musculocutaneous + lateral median root loss |
Key "In the Clinic" Points for Exams
- Cervical spine injuries affect roots
- First rib fracture/severe trauma affects trunks
- Glenohumeral joint dislocation affects divisions and cords
- Axillary nerve is the most commonly injured nerve with anterior shoulder dislocation (tests: sensation over regimental badge area and deltoid power)
- Radial nerve is at risk at the spiral groove of the humerus (mid-shaft fracture = wrist drop)
- Ulnar nerve is at risk at the medial epicondyle (cubital tunnel)
- Median nerve is at risk in the carpal tunnel (CTS) - most common entrapment neuropathy
Sources: Gray's Anatomy for Students, pp. 858-867; Miller's Review of Orthopaedics, pp. 697-699
This is a shared conversation. Sign in to Orris to start your own chat.