concepts and criteria for diagnosis of brain death
Reading File
Finding Sources
Searching PubMed
"brain death" AND diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading Article
PMID: 37821233
I now have comprehensive material from multiple authoritative textbooks and the latest 2023 AAN guideline. Let me compile the full response.
Brain Death: Concepts and Criteria for Diagnosis
Historical Background
The concept of brain death emerged in the 1950s when European neurologists, notably Mollaret and Goulon, described coma dépassé - a state "beyond coma" in which the brain had irreversibly ceased to function while cardiac and pulmonary activity could be sustained artificially. The landmark formalization came from the Harvard Medical School Ad Hoc Committee (1968), chaired by Henry Beecher, which established the first clinical criteria. This redefinition of death was partly prompted by the advent of cardiac transplantation (Barnard, 1967), as it enabled organ retrieval from patients with irreversible neurological destruction.
The concept was later incorporated into the Uniform Determination of Death Act (UDDA), adopted into state laws, and forms the legal standard for declaration of death in most of the United States. The American Academy of Neurology (AAN) published guidelines in 1995, refined them in 2010, and issued the most current Pediatric and Adult Consensus Guideline in 2023 (Greer et al., PMID 37821233).
Definition
Brain death (also called Death by Neurologic Criteria, BD/DNC) is defined as:
The irreversible cessation of all functions of the entire brain, including the brainstem.
This encompasses:
- All cerebral (cortical) functions
- All brainstem functions, including the drive to breathe
- Irreversibility of the state
Note: The British and some Scandinavian criteria accept brainstem death alone as sufficient, without requiring evidence of cortical death - a recognized but minority position.
Prerequisites (Must ALL Be Met Before Examination)
Before the clinical evaluation is conducted, several confounding factors must be excluded:
| Prerequisite | Requirement |
|---|---|
| Cause established | Irreversible structural brain injury identified on neuroimaging (history + CT/MRI) |
| Hypothermia excluded | Core body temperature ≥ 36°C |
| Drug/toxin effect excluded | No sedatives, analgesics, neuromuscular blockers; toxicology screen if indicated |
| Metabolic disturbances excluded | No severe acid-base, electrolyte, or endocrine abnormalities |
| Hemodynamic stability | Systolic BP ≥ 90-100 mmHg |
| Observation period | Several hours must have passed since onset; brain death should not be declared within hours of emergency presentation or transfer |
The most common causes leading to brain death are: severe traumatic brain injury (TBI), aneurysmal subarachnoid hemorrhage, massive intraparenchymal hemorrhage, and anoxic-ischemic brain injury.
The Three Central Clinical Criteria
1. Absence of All Cerebral (Cortical) Functions
- Deep coma - unresponsive to all stimuli (visual, auditory, cutaneous)
- No spontaneous movements
- No motor or vocal responses to any stimulation
- Deep pressure applied to condyles at the temporomandibular joint, supraorbital notch, fingernail beds, or sternal rub elicits no grimacing, no motor response
- Decerebrate or decorticate posturing - considered incompatible with brain death (reflects intact brainstem centers); the physician should wait and re-examine if posturing is present
- Note: Spinal reflexes may persist (deep tendon reflexes, slow plantar flexion); these are spinally mediated and do not exclude brain death
- The "Lazarus sign" (arms rising and crossing at midline when ventilator is disconnected) is a spinal reflex and does not indicate brain function
2. Absence of All Brainstem Reflexes
A detailed examination covering all brainstem levels:
| Reflex / Response | Finding in Brain Death |
|---|---|
| Pupils | Fixed, dilated or mid-position (4-9 mm); no response to bright light in either eye. Constricted pupils should raise concern for opioid effect |
| Corneal reflexes | Absent bilaterally |
| Oculocephalic reflex (Doll's eyes) | Absent - eyes remain fixed, do not move with head turning |
| Oculovestibular reflex (Caloric testing) | Absent - no eye movement after ice-water irrigation of each tympanum (60 mL ice water, head elevated 30°, observe 1 min per side, wait 5 min between sides) |
| Gag reflex | Absent - no contraction on stimulation of posterior oropharynx |
| Cough reflex | Absent - suction catheter passed to carina produces no cough |
| Facial movement | None to deep painful stimulation |
| Motor response to stimulation | Absent in all extremities |
3. Apnea Test - Absence of Spontaneous Respiration
This is the most critical test, demonstrating failure of the medullary respiratory centers:
Procedure:
- Preoxygenate with 100% O₂ for ≥ 10 minutes (PaO₂ ≥ 200 mmHg)
- Obtain baseline ABG: confirm normocapnia (PaCO₂ 35-45 mmHg)
- Disconnect from ventilator; deliver O₂ via insufflation catheter to the level of the carina at 6 L/min (or T-piece with CPAP)
- Observe for 8-10 minutes for any breathing efforts (chest expansion, abdominal excursion, gasping)
- Repeat ABG at the end
Positive apnea test (supports brain death): No spontaneous respirations despite PaCO₂ rising to ≥ 60 mmHg, OR an increase of ≥ 20 mmHg from a normal baseline
Why PaCO₂ 60 mmHg? This represents a maximal physiological stimulus to the medullary respiratory centers. CO₂ rises approximately 2.5 mmHg/min at normal body temperature (slower if hypothermic).
Contraindications/precautions: The test must be aborted if significant hypotension, severe hypoxemia, or cardiac arrhythmias develop. Peripheral causes of respiratory failure (e.g., neuromuscular blockade, Guillain-Barré syndrome) must be absent.
Irreversibility
The diagnosis requires demonstrating an irrefutable cause of catastrophic brain damage (trauma, hemorrhage, cardiac arrest) and excluding all reversible causes:
- Drug overdose or poisoning
- Severe hypothermia
- Metabolic encephalopathies
- Neuromuscular blocking agents
Repeat examination: Most U.S. guidelines do not mandate a second examination, but a waiting period of ~24 hours is advisable when the cause is unclear, cardiac arrest was the antecedent event, or drug/alcohol intoxication cannot be ruled out. Studies have shown that no patient who met brain death criteria ever regained brainstem function on repeat testing.
Confirmatory (Ancillary) Tests
These are not required in most U.S. states if the clinical examination (including apnea test) can be fully completed. They are used when:
- Facial trauma or bilateral eye injury prevent brainstem reflex assessment
- The apnea test cannot be completed safely
- Drug levels remain uncertain
| Test | Finding in Brain Death |
|---|---|
| EEG | Electrocerebral silence (isoelectric/flat EEG) - no electrical potentials > 2 mV during a 30-min recording with ≥ 8 scalp electrodes, interelectrode distance ≥ 10 cm |
| Radionuclide brain scan (SPECT/Technetium) | "Hollow skull" sign - absent intracranial blood flow; specificity ~100%, sensitivity ~75% |
| 4-vessel cerebral angiography | Absence of intracranial blood flow (gold standard for flow) |
| Transcranial Doppler (TCD) | To-and-fro (pendular/Pendelfluss) pattern in basal vessels; reverberant flow |
| CT angiography | Absent intracranial arterial filling |
| Auditory & somatosensory evoked potentials | Absent cerebral responses; variable - not primary diagnostic tool |
| Atropine test | No tachycardia after atropine IV - reflects loss of medullary vagal cardiac innervation |
EEG caveat: An isoelectric EEG with preserved brainstem reflexes does not equal brain death. Electrocerebral silence is also reversible in profound hypothermia, sedative-hypnotic overdose, and immediately post-cardiac arrest.
2023 AAN Consensus Guideline Updates
The 2023 Greer et al. guideline (PMID 37821233) - published in Neurology - is the most current authority. It unifies adult and pediatric criteria for the first time and provides 85 recommendations covering:
- General principles for BD/DNC evaluation
- Qualifications of the examiner
- Prerequisites for determination
- Components of the neurological examination
- Apnea testing protocol
- Ancillary testing
- Special considerations including:
- Patients on extracorporeal membrane oxygenation (ECMO)
- Patients under targeted temperature management (TTM)
- Primary infratentorial injury (posterior fossa/brainstem lesions)
⚠️ Note: The guideline was published with an erratum (PMID 38175986); the core diagnostic framework remains intact.
Philosophical and Ethical Dimensions
- The philosophical equivalence of brain death with somatic death remains contested in some religious communities (Orthodox Jewish, some Asian cultures) and philosophical circles
- New York State requires reasonable accommodation for religious objections; New Jersey allows declaration of cardiac death if brain death violates religious beliefs
- Cases of prolonged survival after meeting brain death criteria have been documented (Shewmon), raising questions about the concept of the brain as the sole integrator of "somatic unity"
- The disconnect between clinical appearance (warm, perfused, heartbeat visible) and neuroimaging (absent brain perfusion) makes brain death paradoxical to lay observers and even some clinicians
Summary: The Three-Part Diagnosis
Brain Death = (1) + (2) + (3), with irreversibility confirmed
(1) Deep unresponsive coma (known irreversible cause)
(2) Absent all brainstem reflexes
(3) Positive apnea test (PaCO₂ ≥ 60 mmHg, no breathing effort)
All confounders excluded (drugs, hypothermia, metabolic, NMB)
Sources: Adams and Victor's Principles of Neurology, 12th Ed. - Plum and Posner's Diagnosis and Treatment of Stupor and Coma - Bradley and Daroff's Neurology in Clinical Practice - Greer DM et al., Neurology 2023 (PMID 37821233, AAN Consensus Guideline)
can you make a seminar ppt on the same topic for 1st year mbbs physiology
Reading File
Reading File
Running Command
mkdir -p /home/daytona/workspace/brain-death-ppt && ls /home/daytona/workspace/brain-death-ppt
Writing File
~/brain-death-ppt/generate.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Brain Death - Concepts and Criteria for Diagnosis";
pres.author = "Department of Physiology";
pres.subject = "1st Year MBBS Physiology Seminar";
// ─── COLOUR PALETTE ───────────────────────────────────────────────
const C = {
navy: "0D1B3E", // deep navy - dominant background
teal: "0A7E8C", // teal accent
lightTeal: "12B5C4", // lighter teal for highlights
white: "FFFFFF",
offWhite: "E8F4F6",
gold: "F2A71B", // warm gold accent for emphasis
darkGray: "2D3142",
midGray: "5C6580",
lightGray: "C8D6DA",
red: "D62839", // alert/danger color
green: "2E9E6B", // positive/present color
bgLight: "F0F7F9", // light slide background
};
// ─── HELPER: SECTION DIVIDER SLIDES ──────────────────────────────
function sectionDivider(title, subtitle) {
const s = pres.addSlide();
// Full background gradient-like shape
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
// Accent bar
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: C.teal } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 2.4, w: 10, h: 0.06, fill: { color: C.teal } });
s.addText(title, {
x: 0.5, y: 1.6, w: 9, h: 1.0,
fontSize: 40, bold: true, color: C.white, align: "center",
fontFace: "Calibri"
});
if (subtitle) {
s.addText(subtitle, {
x: 0.5, y: 2.7, w: 9, h: 0.8,
fontSize: 20, color: C.lightTeal, align: "center",
fontFace: "Calibri"
});
}
return s;
}
// ─── HELPER: CONTENT SLIDE HEADER ────────────────────────────────
function contentSlide(title) {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.bgLight } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.9, fill: { color: C.navy } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0.9, w: 10, h: 0.06, fill: { color: C.teal } });
s.addText(title, {
x: 0.3, y: 0.1, w: 9.4, h: 0.7,
fontSize: 22, bold: true, color: C.white,
fontFace: "Calibri", valign: "middle", margin: 0
});
return s;
}
// ─── HELPER: BULLET TEXT ─────────────────────────────────────────
function bullets(items, options = {}) {
return items.map((item, i) => {
const isLast = i === items.length - 1;
return {
text: item,
options: {
bullet: { type: "bullet", code: "25B6", color: C.teal },
breakLine: !isLast,
...options
}
};
});
}
// ─── HELPER: NUMBERED LIST ────────────────────────────────────────
function numbered(items, options = {}) {
return items.map((item, i) => {
const isLast = i === items.length - 1;
return {
text: item,
options: {
bullet: { type: "number" },
breakLine: !isLast,
...options
}
};
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 1 — TITLE SLIDE
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
// Background
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
// Decorative teal band
s.addShape(pres.ShapeType.rect, { x: 0, y: 3.5, w: 10, h: 0.5, fill: { color: C.teal } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 4.0, w: 10, h: 1.625, fill: { color: C.darkGray } });
// Brain silhouette-style accent circle
s.addShape(pres.ShapeType.ellipse, {
x: 7.0, y: 0.3, w: 2.8, h: 2.8,
fill: { color: "12294A" }, line: { color: C.teal, width: 2 }
});
s.addShape(pres.ShapeType.ellipse, {
x: 7.2, y: 0.5, w: 2.4, h: 2.4,
fill: { color: "0D1B3E" }, line: { color: C.lightTeal, width: 1 }
});
// Institution tag
s.addText("1st Year MBBS | Physiology Seminar", {
x: 0.5, y: 0.2, w: 6.2, h: 0.4,
fontSize: 12, color: C.lightTeal, fontFace: "Calibri",
charSpacing: 3
});
// Main title
s.addText("BRAIN DEATH", {
x: 0.5, y: 0.9, w: 7, h: 1.2,
fontSize: 54, bold: true, color: C.white, fontFace: "Calibri"
});
s.addText("Concepts & Criteria for Diagnosis", {
x: 0.5, y: 2.0, w: 6.8, h: 0.7,
fontSize: 22, color: C.gold, fontFace: "Calibri", italic: true
});
// Teal band text
s.addText("Physiology • Neuroscience • Clinical Application", {
x: 0.5, y: 3.55, w: 9, h: 0.4,
fontSize: 13, color: C.white, fontFace: "Calibri", align: "center", charSpacing: 2
});
// Bottom bar
s.addText("Department of Physiology", {
x: 0.5, y: 4.1, w: 5, h: 0.35,
fontSize: 13, color: C.lightGray, fontFace: "Calibri"
});
s.addText("References: Adams & Victor's Neurology 12e | AAN Guidelines 2023", {
x: 0.5, y: 4.5, w: 9, h: 0.3,
fontSize: 9, color: C.midGray, fontFace: "Calibri", italic: true
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 2 — OVERVIEW / ROADMAP
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("Seminar Overview");
const topics = [
{ num: "01", label: "Historical Background" },
{ num: "02", label: "Definition of Brain Death" },
{ num: "03", label: "Physiological Basis" },
{ num: "04", label: "Prerequisites Before Examination" },
{ num: "05", label: "Clinical Criteria (3 Core Tests)" },
{ num: "06", label: "Apnea Test - Detailed Protocol" },
{ num: "07", label: "Brainstem Reflexes - Anatomy" },
{ num: "08", label: "Confirmatory Ancillary Tests" },
{ num: "09", label: "Ethical & Legal Dimensions" },
{ num: "10", label: "Summary & Key Take-aways" },
];
// Two columns
const col1 = topics.slice(0, 5);
const col2 = topics.slice(5);
col1.forEach((t, i) => {
const y = 1.1 + i * 0.77;
s.addShape(pres.ShapeType.roundRect, {
x: 0.3, y, w: 4.3, h: 0.62,
fill: { color: C.navy }, rectRadius: 0.08,
line: { color: C.teal, width: 1 }
});
s.addText(t.num, {
x: 0.35, y: y + 0.05, w: 0.6, h: 0.52,
fontSize: 16, bold: true, color: C.gold, fontFace: "Calibri", valign: "middle", align: "center"
});
s.addText(t.label, {
x: 0.95, y: y + 0.05, w: 3.5, h: 0.52,
fontSize: 14, color: C.white, fontFace: "Calibri", valign: "middle"
});
});
col2.forEach((t, i) => {
const y = 1.1 + i * 0.77;
s.addShape(pres.ShapeType.roundRect, {
x: 5.2, y, w: 4.5, h: 0.62,
fill: { color: C.navy }, rectRadius: 0.08,
line: { color: C.teal, width: 1 }
});
s.addText(t.num, {
x: 5.25, y: y + 0.05, w: 0.6, h: 0.52,
fontSize: 16, bold: true, color: C.gold, fontFace: "Calibri", valign: "middle", align: "center"
});
s.addText(t.label, {
x: 5.85, y: y + 0.05, w: 3.7, h: 0.52,
fontSize: 14, color: C.white, fontFace: "Calibri", valign: "middle"
});
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 3 — SECTION DIVIDER: History
// ═══════════════════════════════════════════════════════════════════
sectionDivider("01 Historical Background", "How 'brain death' came to be defined");
// ═══════════════════════════════════════════════════════════════════
// SLIDE 4 — HISTORICAL TIMELINE
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("Historical Milestones");
const events = [
{ yr: "1950s", color: C.teal, text: "Mollaret & Goulon describe 'coma dépassé' (beyond coma) - brain destroyed but heart/lungs maintained by machine" },
{ yr: "1967", color: C.gold, text: "First cardiac transplant by Dr. Christian Barnard, South Africa - urgency for donor organ criteria" },
{ yr: "1968", color: C.lightTeal, text: "Harvard Ad Hoc Committee (Beecher) publishes first formal brain death criteria - deep coma, absent reflexes, flat EEG for 24 h" },
{ yr: "1981", color: C.teal, text: "Uniform Determination of Death Act (UDDA) - legal definition of death includes 'irreversible cessation of all brain functions'" },
{ yr: "1995", color: C.gold, text: "AAN publishes first neurological guidelines for brain death in adults" },
{ yr: "2010", color: C.lightTeal, text: "AAN updates guidelines with evidence-based refinements" },
{ yr: "2023", color: C.red, text: "AAN Consensus Guideline unifies adult & pediatric criteria - 85 recommendations (Greer et al., Neurology)" },
];
events.forEach((e, i) => {
const y = 1.05 + i * 0.63;
// Year badge
s.addShape(pres.ShapeType.roundRect, {
x: 0.25, y, w: 0.8, h: 0.5,
fill: { color: e.color }, rectRadius: 0.06
});
s.addText(e.yr, {
x: 0.25, y, w: 0.8, h: 0.5,
fontSize: 11, bold: true, color: C.navy, align: "center", valign: "middle", fontFace: "Calibri"
});
// connector dot
s.addShape(pres.ShapeType.ellipse, {
x: 1.12, y: y + 0.18, w: 0.14, h: 0.14, fill: { color: e.color }
});
// Line
if (i < events.length - 1) {
s.addShape(pres.ShapeType.line, {
x: 1.18, y: y + 0.32, w: 0, h: 0.45,
line: { color: C.lightGray, width: 1 }
});
}
s.addText(e.text, {
x: 1.35, y: y + 0.02, w: 8.4, h: 0.46,
fontSize: 12, color: C.darkGray, fontFace: "Calibri", valign: "middle"
});
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 5 — SECTION DIVIDER: Definition
// ═══════════════════════════════════════════════════════════════════
sectionDivider("02 Definition", "What exactly is brain death?");
// ═══════════════════════════════════════════════════════════════════
// SLIDE 6 — DEFINITION
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("Definition of Brain Death");
// Big definition box
s.addShape(pres.ShapeType.roundRect, {
x: 0.4, y: 1.05, w: 9.2, h: 1.1,
fill: { color: C.navy }, rectRadius: 0.12,
line: { color: C.teal, width: 2 }
});
s.addText([
{ text: "Brain Death ", options: { bold: true, color: C.gold } },
{ text: "= Irreversible cessation of ALL functions of the ENTIRE brain,\nincluding the brainstem", options: { color: C.white } }
], {
x: 0.55, y: 1.1, w: 9.0, h: 1.0,
fontSize: 17, fontFace: "Calibri", valign: "middle"
});
// Also known as box
s.addShape(pres.ShapeType.roundRect, {
x: 0.4, y: 2.3, w: 4.4, h: 0.5,
fill: { color: C.teal }, rectRadius: 0.08
});
s.addText("Also called: Death by Neurologic Criteria (BD/DNC)", {
x: 0.4, y: 2.3, w: 4.4, h: 0.5,
fontSize: 13, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri"
});
// Three components
const comps = [
{ icon: "1", title: "Absent Cerebral Functions", desc: "No response to any stimulus; deep coma" },
{ icon: "2", title: "Absent Brainstem Functions", desc: "Loss of all brainstem reflexes" },
{ icon: "3", title: "Irreversibility", desc: "Permanent, cannot recover with any intervention" },
];
comps.forEach((c, i) => {
const x = 0.3 + i * 3.25;
s.addShape(pres.ShapeType.roundRect, {
x, y: 3.0, w: 3.05, h: 2.3,
fill: { color: C.darkGray }, rectRadius: 0.1,
line: { color: C.teal, width: 1 }
});
s.addShape(pres.ShapeType.ellipse, {
x: x + 1.1, y: 3.1, w: 0.7, h: 0.7,
fill: { color: C.teal }
});
s.addText(c.icon, {
x: x + 1.1, y: 3.1, w: 0.7, h: 0.7,
fontSize: 18, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri"
});
s.addText(c.title, {
x: x + 0.1, y: 3.9, w: 2.8, h: 0.55,
fontSize: 14, bold: true, color: C.gold, align: "center", fontFace: "Calibri"
});
s.addText(c.desc, {
x: x + 0.1, y: 4.5, w: 2.8, h: 0.65,
fontSize: 12, color: C.lightGray, align: "center", fontFace: "Calibri"
});
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 7 — SECTION DIVIDER: Physiological Basis
// ═══════════════════════════════════════════════════════════════════
sectionDivider("03 Physiological Basis", "Why the brainstem is the key organ of survival");
// ═══════════════════════════════════════════════════════════════════
// SLIDE 8 — PHYSIOLOGICAL BASIS
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("Physiological Basis of Brain Death");
// Left panel - brainstem functions
s.addShape(pres.ShapeType.roundRect, {
x: 0.25, y: 1.05, w: 4.6, h: 4.3,
fill: { color: C.navy }, rectRadius: 0.12,
line: { color: C.teal, width: 1.5 }
});
s.addText("Vital Brainstem Functions", {
x: 0.3, y: 1.1, w: 4.5, h: 0.5,
fontSize: 16, bold: true, color: C.gold, align: "center", fontFace: "Calibri"
});
const bsFunctions = [
"Respiratory drive (medullary respiratory center)",
"Cardiovascular control (vasomotor center)",
"Consciousness & arousal (reticular activating system - RAS)",
"Cranial nerve reflexes (pupillary, gag, corneal, oculovestibular)",
"Swallowing, coughing, vomiting",
"Thermoregulation (hypothalamus input)",
"Sleep-wake cycle regulation",
];
s.addText(bullets(bsFunctions, { fontSize: 12, color: C.offWhite, fontFace: "Calibri", paraSpaceAfter: 4 }),
{ x: 0.35, y: 1.7, w: 4.4, h: 3.5, valign: "top" });
// Right panel - why brain death = death
s.addShape(pres.ShapeType.roundRect, {
x: 5.1, y: 1.05, w: 4.6, h: 2.0,
fill: { color: C.darkGray }, rectRadius: 0.12,
line: { color: C.gold, width: 1.5 }
});
s.addText("Why Brain Death = Death?", {
x: 5.15, y: 1.1, w: 4.5, h: 0.45,
fontSize: 15, bold: true, color: C.gold, align: "center", fontFace: "Calibri"
});
s.addText([
{ text: "When the entire brain (cortex + brainstem) permanently ceases function:\n", options: { color: C.lightGray, fontSize: 12 } },
{ text: "• No consciousness possible (cortex gone)\n", options: { color: C.offWhite, fontSize: 12 } },
{ text: "• No spontaneous breathing (medulla gone)\n", options: { color: C.offWhite, fontSize: 12 } },
{ text: "• Cardiac arrest inevitable without support\n", options: { color: C.offWhite, fontSize: 12 } },
{ text: "→ The organism as a whole cannot survive", options: { color: C.lightTeal, fontSize: 12, bold: true } },
], { x: 5.2, y: 1.6, w: 4.4, h: 1.35, valign: "top", fontFace: "Calibri" });
// Right lower - Common causes
s.addShape(pres.ShapeType.roundRect, {
x: 5.1, y: 3.2, w: 4.6, h: 2.15,
fill: { color: C.darkGray }, rectRadius: 0.12,
line: { color: C.teal, width: 1.5 }
});
s.addText("Common Causes of Brain Death", {
x: 5.15, y: 3.25, w: 4.5, h: 0.45,
fontSize: 15, bold: true, color: C.teal, align: "center", fontFace: "Calibri"
});
const causes = ["Severe Traumatic Brain Injury (TBI)", "Aneurysmal Subarachnoid Hemorrhage (aSAH)", "Massive Intraparenchymal Hemorrhage", "Anoxic-Ischemic Brain Injury (cardiac arrest)", "Severe cerebral edema with herniation"];
s.addText(bullets(causes, { fontSize: 12, color: C.offWhite, fontFace: "Calibri", paraSpaceAfter: 2 }),
{ x: 5.2, y: 3.75, w: 4.4, h: 1.5, valign: "top" });
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 9 — SECTION DIVIDER: Prerequisites
// ═══════════════════════════════════════════════════════════════════
sectionDivider("04 Prerequisites", "Before the clinical examination begins");
// ═══════════════════════════════════════════════════════════════════
// SLIDE 10 — PREREQUISITES
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("Prerequisites - Must ALL Be Met Before Examination");
const prereqs = [
{ num: "1", title: "Known, Irreversible Cause", desc: "Neuroimaging (CT/MRI) confirms catastrophic structural brain injury. Cause must be established.", color: C.teal },
{ num: "2", title: "No Hypothermia", desc: "Core body temperature must be ≥ 36°C. Hypothermia mimics brain death (cold suppresses all CNS activity).", color: C.gold },
{ num: "3", title: "No Drug / Toxin Effect", desc: "Sedatives, opioids, NMBAs, alcohol must be absent. Toxicology screen if in doubt.", color: C.teal },
{ num: "4", title: "No Severe Metabolic Disorder", desc: "Rule out severe electrolyte, acid-base, endocrine (e.g. severe hypoglycemia, Na+ disorders) abnormalities.", color: C.gold },
{ num: "5", title: "Hemodynamic Stability", desc: "Systolic BP ≥ 90-100 mmHg needed before apnea test. Vasopressors may be needed.", color: C.teal },
{ num: "6", title: "Observation Period", desc: "Several hours must pass after brain injury. Do NOT declare brain death within hours of ER arrival.", color: C.gold },
];
prereqs.forEach((p, i) => {
const row = Math.floor(i / 2);
const col = i % 2;
const x = 0.25 + col * 4.9;
const y = 1.1 + row * 1.45;
s.addShape(pres.ShapeType.roundRect, {
x, y, w: 4.6, h: 1.3,
fill: { color: C.darkGray }, rectRadius: 0.1,
line: { color: p.color, width: 1.5 }
});
s.addShape(pres.ShapeType.ellipse, {
x: x + 0.12, y: y + 0.28, w: 0.55, h: 0.55,
fill: { color: p.color }
});
s.addText(p.num, {
x: x + 0.12, y: y + 0.28, w: 0.55, h: 0.55,
fontSize: 15, bold: true, color: C.navy, align: "center", valign: "middle", fontFace: "Calibri"
});
s.addText(p.title, {
x: x + 0.75, y: y + 0.08, w: 3.7, h: 0.4,
fontSize: 13, bold: true, color: p.color, fontFace: "Calibri", valign: "middle"
});
s.addText(p.desc, {
x: x + 0.75, y: y + 0.48, w: 3.7, h: 0.75,
fontSize: 11, color: C.lightGray, fontFace: "Calibri", valign: "top"
});
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 11 — SECTION DIVIDER: 3 Clinical Criteria
// ═══════════════════════════════════════════════════════════════════
sectionDivider("05 The Three Clinical Criteria", "The core diagnostic triad");
// ═══════════════════════════════════════════════════════════════════
// SLIDE 12 — THREE CRITERIA OVERVIEW
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("The Three Core Clinical Criteria");
// Equation display
s.addShape(pres.ShapeType.roundRect, {
x: 0.3, y: 1.05, w: 9.4, h: 0.75,
fill: { color: C.navy }, rectRadius: 0.1,
line: { color: C.teal, width: 1 }
});
s.addText([
{ text: "Brain Death = ", options: { color: C.lightGray, bold: false } },
{ text: "(1) Unresponsive Coma", options: { color: C.gold, bold: true } },
{ text: " + ", options: { color: C.white } },
{ text: "(2) Absent Brainstem Reflexes", options: { color: C.lightTeal, bold: true } },
{ text: " + ", options: { color: C.white } },
{ text: "(3) Absent Respiratory Drive", options: { color: C.red, bold: true } },
], { x: 0.3, y: 1.05, w: 9.4, h: 0.75, align: "center", valign: "middle", fontSize: 17, fontFace: "Calibri" });
// Three criteria cards
const criteria = [
{
num: "01",
title: "Deep Unresponsive\nComa",
color: C.gold,
points: [
"No response to any stimulation",
"No spontaneous movements",
"No motor / vocal responses",
"Glasgow Coma Score = 3",
"Spinal reflexes MAY persist\n(do not exclude brain death)"
]
},
{
num: "02",
title: "Absent All\nBrainstem Reflexes",
color: C.lightTeal,
points: [
"Fixed dilated pupils (4-9 mm)",
"No corneal reflexes (bilateral)",
"No oculocephalic reflex",
"No caloric (oculovestibular) reflex",
"No gag / cough reflex",
"No facial response to pain"
]
},
{
num: "03",
title: "Positive Apnea\nTest",
color: C.red,
points: [
"No spontaneous breaths",
"despite PaCO₂ ≥ 60 mmHg",
"OR rise of ≥ 20 mmHg from",
"normal baseline PaCO₂",
"Medullary respiratory center\nhas completely failed"
]
},
];
criteria.forEach((c, i) => {
const x = 0.25 + i * 3.25;
// Card background
s.addShape(pres.ShapeType.roundRect, {
x, y: 1.95, w: 3.1, h: 3.45,
fill: { color: C.darkGray }, rectRadius: 0.12,
line: { color: c.color, width: 2 }
});
// Number badge
s.addShape(pres.ShapeType.ellipse, {
x: x + 1.1, y: 2.0, w: 0.9, h: 0.9,
fill: { color: c.color }
});
s.addText(c.num, {
x: x + 1.1, y: 2.0, w: 0.9, h: 0.9,
fontSize: 20, bold: true, color: C.navy, align: "center", valign: "middle", fontFace: "Calibri"
});
// Title
s.addText(c.title, {
x: x + 0.1, y: 3.0, w: 2.9, h: 0.75,
fontSize: 14, bold: true, color: c.color, align: "center", fontFace: "Calibri"
});
// Points
s.addText(bullets(c.points, { fontSize: 11, color: C.offWhite, fontFace: "Calibri", paraSpaceAfter: 2 }),
{ x: x + 0.1, y: 3.75, w: 2.9, h: 1.55, valign: "top" });
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 13 — SECTION DIVIDER: Apnea Test
// ═══════════════════════════════════════════════════════════════════
sectionDivider("06 The Apnea Test", "Detailed protocol & physiological rationale");
// ═══════════════════════════════════════════════════════════════════
// SLIDE 14 — APNEA TEST PROTOCOL
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("Apnea Test — Step-by-Step Protocol");
const steps = [
{ n: "1", text: "Preoxygenate with 100% O₂ for ≥ 10 minutes", sub: "Target: PaO₂ ≥ 200 mmHg", color: C.teal },
{ n: "2", text: "Ensure hemodynamic stability", sub: "Systolic BP ≥ 90-100 mmHg; increase vasopressors if needed", color: C.teal },
{ n: "3", text: "Baseline ABG confirming normocapnia", sub: "PaCO₂ = 35-45 mmHg; adjust ventilator if needed", color: C.teal },
{ n: "4", text: "Disconnect from ventilator", sub: "Deliver O₂ via catheter at carina at 6 L/min", color: C.gold },
{ n: "5", text: "Observe for 8-10 minutes", sub: "Watch for any chest expansion, abdominal excursion, or gasping", color: C.gold },
{ n: "6", text: "Repeat ABG at the end", sub: "Positive test: PaCO₂ ≥ 60 mmHg OR ↑ ≥ 20 mmHg from baseline, with NO breathing", color: C.red },
];
steps.forEach((step, i) => {
const x = (i < 3) ? 0.25 : 5.1;
const row = i % 3;
const y = 1.1 + row * 1.45;
s.addShape(pres.ShapeType.roundRect, {
x, y, w: 4.6, h: 1.3,
fill: { color: C.navy }, rectRadius: 0.1,
line: { color: step.color, width: 1.5 }
});
s.addShape(pres.ShapeType.ellipse, {
x: x + 0.12, y: y + 0.28, w: 0.55, h: 0.55,
fill: { color: step.color }
});
s.addText(step.n, {
x: x + 0.12, y: y + 0.28, w: 0.55, h: 0.55,
fontSize: 16, bold: true, color: C.navy, align: "center", valign: "middle", fontFace: "Calibri"
});
s.addText(step.text, {
x: x + 0.75, y: y + 0.08, w: 3.7, h: 0.45,
fontSize: 13, bold: true, color: step.color, fontFace: "Calibri", valign: "middle"
});
s.addText(step.sub, {
x: x + 0.75, y: y + 0.55, w: 3.7, h: 0.65,
fontSize: 11, color: C.lightGray, fontFace: "Calibri", valign: "top"
});
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 15 — APNEA TEST PHYSIOLOGY
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("Apnea Test — Physiological Rationale");
// Left: explanation
s.addShape(pres.ShapeType.roundRect, {
x: 0.25, y: 1.1, w: 4.6, h: 4.25,
fill: { color: C.navy }, rectRadius: 0.12,
line: { color: C.teal, width: 1.5 }
});
s.addText("Why CO₂ is the trigger?", {
x: 0.3, y: 1.15, w: 4.5, h: 0.45,
fontSize: 16, bold: true, color: C.gold, align: "center", fontFace: "Calibri"
});
const rationale = [
"CO₂ is the most potent physiological stimulus to breathe",
"Central chemoreceptors in the medulla oblongata respond to rising PaCO₂ → H⁺ ions",
"In a living brainstem: rising CO₂ triggers inspiratory neurons → breathing",
"In brain death: no respiratory response regardless of CO₂ level",
"CO₂ rises ~2.5 mmHg/min at normothermia (slower if hypothermic)",
"Target PaCO₂ ≥ 60 mmHg is an unambiguous maximal stimulus",
"Also confirms medullary center destruction"
];
s.addText(bullets(rationale, { fontSize: 12, color: C.offWhite, fontFace: "Calibri", paraSpaceAfter: 5 }),
{ x: 0.3, y: 1.7, w: 4.5, h: 3.5, valign: "top" });
// Right: abort criteria
s.addShape(pres.ShapeType.roundRect, {
x: 5.1, y: 1.1, w: 4.6, h: 2.0,
fill: { color: C.darkGray }, rectRadius: 0.12,
line: { color: C.red, width: 1.5 }
});
s.addText("ABORT Test Immediately If:", {
x: 5.2, y: 1.15, w: 4.4, h: 0.45,
fontSize: 15, bold: true, color: C.red, align: "center", fontFace: "Calibri"
});
s.addText(bullets(["SpO₂ drops below safe levels (severe hypoxemia)", "Significant hypotension despite vasopressors", "Cardiac arrhythmias develop"],
{ fontSize: 12, color: C.offWhite, fontFace: "Calibri", paraSpaceAfter: 4 }),
{ x: 5.2, y: 1.65, w: 4.4, h: 1.35, valign: "top" });
// Right: confounders
s.addShape(pres.ShapeType.roundRect, {
x: 5.1, y: 3.25, w: 4.6, h: 2.1,
fill: { color: C.darkGray }, rectRadius: 0.12,
line: { color: C.gold, width: 1.5 }
});
s.addText("Important Exclusions:", {
x: 5.2, y: 3.3, w: 4.4, h: 0.45,
fontSize: 15, bold: true, color: C.gold, align: "center", fontFace: "Calibri"
});
s.addText(bullets(["Neuromuscular blocking agents (e.g. vecuronium) - peripheral cause of apnea", "Guillain-Barré syndrome - peripheral respiratory failure", "Severe hypothermia - reduces CO₂ sensitivity"],
{ fontSize: 12, color: C.offWhite, fontFace: "Calibri", paraSpaceAfter: 4 }),
{ x: 5.2, y: 3.8, w: 4.4, h: 1.45, valign: "top" });
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 16 — SECTION DIVIDER: Brainstem Reflexes
// ═══════════════════════════════════════════════════════════════════
sectionDivider("07 Brainstem Reflexes in Detail", "Anatomy and testing of each reflex");
// ═══════════════════════════════════════════════════════════════════
// SLIDE 17 — BRAINSTEM REFLEXES TABLE
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("Brainstem Reflexes — Testing & Anatomy");
const rows = [
["Pupillary Light Reflex", "CN II (afferent) → CN III (efferent)", "Bright light in each eye; no constriction", "Fixed, dilated or mid-position (4-9 mm)", "CN III nucleus - midbrain"],
["Corneal Reflex", "CN V (afferent) → CN VII (efferent)", "Cotton wisp on cornea; no blink", "Absent bilaterally", "Pons"],
["Oculocephalic (Doll's Eyes)", "CN VIII → CN III, VI", "Brisk head rotation; eyes stay fixed", "Absent; eyes move with head", "Pontine gaze center"],
["Oculovestibular (Caloric)", "CN VIII → CN III, VI", "60 mL ice-water in ear; no eye movement", "Absent - in living coma, eyes deviate toward cold", "Pons - medulla junction"],
["Gag Reflex", "CN IX (afferent) → CN X (efferent)", "Stimulate posterior pharynx; no contraction", "Absent", "Medulla"],
["Cough Reflex", "CN X", "Suction catheter to carina; no cough", "Absent", "Medulla"],
];
// Table
const colW = [2.2, 2.1, 2.1, 1.9, 1.55];
const colX = [0.15, 2.35, 4.45, 6.55, 8.45];
const headers = ["Reflex", "Cranial Nerves", "Test", "Finding in Brain Death", "Level"];
// Header row
headers.forEach((h, ci) => {
s.addShape(pres.ShapeType.rect, {
x: colX[ci], y: 1.05, w: colW[ci], h: 0.45,
fill: { color: C.teal }
});
s.addText(h, {
x: colX[ci], y: 1.05, w: colW[ci], h: 0.45,
fontSize: 11, bold: true, color: C.navy, align: "center", valign: "middle", fontFace: "Calibri"
});
});
rows.forEach((row, ri) => {
const y = 1.5 + ri * 0.67;
const bg = ri % 2 === 0 ? "1E2D48" : C.darkGray;
row.forEach((cell, ci) => {
s.addShape(pres.ShapeType.rect, {
x: colX[ci], y, w: colW[ci], h: 0.65,
fill: { color: bg },
line: { color: "2D4070", width: 0.5 }
});
s.addText(cell, {
x: colX[ci] + 0.05, y: y + 0.02, w: colW[ci] - 0.1, h: 0.61,
fontSize: 10, color: ci === 3 ? C.red : C.offWhite,
fontFace: "Calibri", valign: "middle",
bold: ci === 3
});
});
});
// Note
s.addText("Note: Constricted (pinpoint) pupils should raise suspicion of opioid effect — not compatible with brain death", {
x: 0.15, y: 5.3, w: 9.7, h: 0.25,
fontSize: 9.5, color: C.gold, italic: true, fontFace: "Calibri"
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 18 — LAZARUS SIGN & SPINAL REFLEXES
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("Spinal Reflexes in Brain Death — Do NOT Confuse!");
s.addShape(pres.ShapeType.roundRect, {
x: 0.25, y: 1.1, w: 9.5, h: 0.75,
fill: { color: C.red }, rectRadius: 0.1
});
s.addText("IMPORTANT: Spinal reflexes are PRESERVED in brain death — they do NOT indicate brain function!", {
x: 0.3, y: 1.1, w: 9.4, h: 0.75,
fontSize: 15, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri"
});
const reflexes = [
{ name: "Deep Tendon Reflexes", desc: "Knee jerk, biceps, etc. can persist. Mediated entirely at spinal cord level. Do NOT exclude brain death." },
{ name: "Plantar Reflex", desc: "Toes may flex slowly. A Babinski sign is unusual but does not exclude brain death if present." },
{ name: "The Lazarus Sign", desc: "Arms rise off the bed and cross at the midline as if in prayer, when ventilator is disconnected. Spinally mediated. First described by Ropper in 1984. Can be very disturbing to observers — family should not be present during ventilator disconnection." },
{ name: "Opisthotonos-like movements", desc: "Chest expansion mimicking a breath, shoulder shrugging. All spinal / autonomic. Do NOT indicate brain activity." },
];
reflexes.forEach((r, i) => {
const y = 2.05 + i * 0.84;
s.addShape(pres.ShapeType.roundRect, {
x: 0.25, y, w: 9.5, h: 0.75,
fill: { color: C.darkGray }, rectRadius: 0.08,
line: { color: C.midGray, width: 0.5 }
});
s.addText(r.name + ": ", {
x: 0.35, y: y + 0.03, w: 2.0, h: 0.68,
fontSize: 13, bold: true, color: C.gold, fontFace: "Calibri", valign: "middle"
});
s.addText(r.desc, {
x: 2.25, y: y + 0.03, w: 7.3, h: 0.68,
fontSize: 12, color: C.offWhite, fontFace: "Calibri", valign: "middle"
});
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 19 — SECTION DIVIDER: Confirmatory Tests
// ═══════════════════════════════════════════════════════════════════
sectionDivider("08 Ancillary / Confirmatory Tests", "When extra confirmation is needed");
// ═══════════════════════════════════════════════════════════════════
// SLIDE 20 — CONFIRMATORY TESTS
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("Ancillary (Confirmatory) Tests");
// When needed box
s.addShape(pres.ShapeType.roundRect, {
x: 0.25, y: 1.05, w: 9.5, h: 0.7,
fill: { color: C.navy }, rectRadius: 0.1,
line: { color: C.teal, width: 1.5 }
});
s.addText([
{ text: "These are NOT required ", options: { bold: true, color: C.gold } },
{ text: "in most US states if the full clinical exam + apnea test can be completed. Used when exam is incomplete (e.g. severe facial trauma, bilateral eye injury, drug levels unclear).", options: { color: C.offWhite } }
], { x: 0.35, y: 1.07, w: 9.2, h: 0.65, fontSize: 12, fontFace: "Calibri", valign: "middle" });
const tests = [
{ name: "EEG (Electroencephalography)", finding: "Electrocerebral silence — no potentials >2 mV during 30-min recording. Caveat: flat EEG alone does not = brain death; also seen in hypothermia, drug overdose.", color: C.teal },
{ name: "Radionuclide Brain Scan (SPECT)", finding: '"Hollow skull" sign — absent cerebral blood flow. Specificity ~100%, sensitivity ~75%. False negatives if posterior fossa vessels show minimal flow.', color: C.gold },
{ name: "4-Vessel Cerebral Angiography", finding: "Gold standard for absent intracranial blood flow. No contrast beyond circle of Willis.", color: C.teal },
{ name: "CT Angiography (CTA)", finding: "Absent intracranial arterial filling. Increasingly used as non-invasive alternative.", color: C.gold },
{ name: "Transcranial Doppler (TCD)", finding: "To-and-fro (Pendelfluss / reverberant) flow pattern in basal cerebral vessels.", color: C.teal },
{ name: "Evoked Potentials (AEP / SSEP)", finding: "Absent cerebral responses. Variable — not the primary diagnostic tool. Only used in specialized settings.", color: C.gold },
];
tests.forEach((t, i) => {
const row = Math.floor(i / 2);
const col = i % 2;
const x = 0.25 + col * 4.9;
const y = 1.9 + row * 1.18;
s.addShape(pres.ShapeType.roundRect, {
x, y, w: 4.6, h: 1.05,
fill: { color: C.darkGray }, rectRadius: 0.08,
line: { color: t.color, width: 1 }
});
s.addText(t.name, {
x: x + 0.12, y: y + 0.05, w: 4.35, h: 0.35,
fontSize: 12, bold: true, color: t.color, fontFace: "Calibri", valign: "middle"
});
s.addText(t.finding, {
x: x + 0.12, y: y + 0.4, w: 4.35, h: 0.6,
fontSize: 10, color: C.lightGray, fontFace: "Calibri", valign: "top"
});
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 21 — SECTION DIVIDER: Ethics & Legal
// ═══════════════════════════════════════════════════════════════════
sectionDivider("09 Ethical & Legal Dimensions", "Societal, cultural and religious considerations");
// ═══════════════════════════════════════════════════════════════════
// SLIDE 22 — ETHICS & LAW
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("Ethical, Legal & Cultural Considerations");
const topics = [
{
title: "Legal Status",
icon: "⚖",
color: C.teal,
points: [
"Brain death is legally equated with cardiorespiratory death in most countries",
"Incorporated in the Uniform Determination of Death Act (UDDA), USA",
"Forms the basis for organ donation (deceased donor transplantation)",
"Declared by a qualified physician after complete evaluation",
]
},
{
title: "Religious & Cultural Objections",
icon: "✦",
color: C.gold,
points: [
"Some Orthodox Jewish communities and certain Asian cultures reject brain death",
"Japan only recently legalized brain death determinations",
"New York State: requires reasonable accommodation for religious objections",
"New Jersey: allows declaration of cardiac death if family objects on religious grounds",
]
},
{
title: "Philosophical Issues",
icon: "?",
color: C.lightTeal,
points: [
"Shewmon documented rare cases of prolonged survival after meeting brain death criteria",
"Live births from brain-dead mothers challenge 'somatic integration' argument",
"British/Scandinavian criteria: brainstem death alone = death (minority view)",
"Most authorities: operational construct serves patients & society well",
]
},
];
topics.forEach((t, i) => {
const x = 0.2 + i * 3.27;
s.addShape(pres.ShapeType.roundRect, {
x, y: 1.1, w: 3.1, h: 4.25,
fill: { color: C.navy }, rectRadius: 0.12,
line: { color: t.color, width: 2 }
});
s.addShape(pres.ShapeType.ellipse, {
x: x + 1.07, y: 1.2, w: 0.9, h: 0.9,
fill: { color: t.color }
});
s.addText(t.icon, {
x: x + 1.07, y: 1.2, w: 0.9, h: 0.9,
fontSize: 18, bold: true, color: C.navy, align: "center", valign: "middle", fontFace: "Calibri"
});
s.addText(t.title, {
x: x + 0.1, y: 2.2, w: 2.9, h: 0.6,
fontSize: 14, bold: true, color: t.color, align: "center", fontFace: "Calibri"
});
s.addText(bullets(t.points, { fontSize: 11, color: C.offWhite, fontFace: "Calibri", paraSpaceAfter: 5 }),
{ x: x + 0.1, y: 2.85, w: 2.9, h: 2.4, valign: "top" });
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 23 — SECTION DIVIDER: Summary
// ═══════════════════════════════════════════════════════════════════
sectionDivider("10 Summary & Key Take-aways", "What every 1st Year MBBS student must remember");
// ═══════════════════════════════════════════════════════════════════
// SLIDE 24 — SUMMARY
// ═══════════════════════════════════════════════════════════════════
{
const s = contentSlide("Summary — Brain Death Diagnosis at a Glance");
// Formula box
s.addShape(pres.ShapeType.roundRect, {
x: 0.25, y: 1.05, w: 9.5, h: 0.8,
fill: { color: C.navy }, rectRadius: 0.1,
line: { color: C.gold, width: 2 }
});
s.addText([
{ text: "BRAIN DEATH = ", options: { color: C.white } },
{ text: "Known cause + Unresponsive coma + Absent brainstem reflexes + Positive apnea test\n", options: { color: C.gold, bold: true } },
{ text: "WITH all confounders excluded (drugs • hypothermia • metabolic • NMBAs)", options: { color: C.lightTeal, italic: true } },
], { x: 0.35, y: 1.07, w: 9.2, h: 0.76, fontSize: 13, fontFace: "Calibri", align: "center", valign: "middle" });
// Key points
const keys = [
{ n: "1", text: "Brain death = irreversible cessation of ALL brain + brainstem functions", c: C.gold },
{ n: "2", text: "Three clinical criteria: coma + absent brainstem reflexes + positive apnea test", c: C.lightTeal },
{ n: "3", text: "Apnea test: no breathing when PaCO₂ ≥ 60 mmHg (medullary center test)", c: C.gold },
{ n: "4", text: "Prerequisites MUST be met: exclude hypothermia, drugs, metabolic causes", c: C.lightTeal },
{ n: "5", text: "Spinal reflexes (Lazarus sign, DTRs) do NOT indicate brain function", c: C.gold },
{ n: "6", text: "Confirmatory tests (EEG, angiography) used only when exam is incomplete", c: C.lightTeal },
{ n: "7", text: "AAN 2023 Consensus Guideline is the current authority (Greer et al.)", c: C.gold },
{ n: "8", text: "Legal definition in most countries; critical foundation for organ donation", c: C.lightTeal },
];
keys.forEach((k, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
const x = 0.25 + col * 4.9;
const y = 2.05 + row * 0.84;
s.addShape(pres.ShapeType.roundRect, {
x, y, w: 4.6, h: 0.7,
fill: { color: C.darkGray }, rectRadius: 0.08,
line: { color: k.c, width: 1 }
});
s.addShape(pres.ShapeType.ellipse, {
x: x + 0.1, y: y + 0.1, w: 0.5, h: 0.5,
fill: { color: k.c }
});
s.addText(k.n, {
x: x + 0.1, y: y + 0.1, w: 0.5, h: 0.5,
fontSize: 14, bold: true, color: C.navy, align: "center", valign: "middle", fontFace: "Calibri"
});
s.addText(k.text, {
x: x + 0.7, y: y + 0.05, w: 3.8, h: 0.6,
fontSize: 12, color: C.offWhite, fontFace: "Calibri", valign: "middle"
});
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 25 — REFERENCES
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.15, h: 5.625, fill: { color: C.teal } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0.85, w: 10, h: 0.05, fill: { color: C.teal } });
s.addText("References", {
x: 0.4, y: 0.1, w: 9.2, h: 0.65,
fontSize: 28, bold: true, color: C.white, fontFace: "Calibri"
});
const refs = [
"1. Adams & Victor's Principles of Neurology, 12th Edition — Ropper AH, Samuels MA, Klein JP (McGraw-Hill, 2023)",
"2. Plum and Posner's Diagnosis and Treatment of Stupor and Coma — Laureys S, Gosseries O (Oxford University Press)",
"3. Bradley and Daroff's Neurology in Clinical Practice, 8th Edition — Josephs KA (Elsevier, 2022)",
"4. Greer DM, Kirschen MP, Lewis A, et al. Pediatric and Adult Brain Death/Death by Neurologic Criteria\n Consensus Guideline. Neurology. 2023 Dec 12. PMID: 37821233",
"5. Wijdicks EFM, et al. Evidence-based guideline update: Determining brain death in adults. Neurology. 2010;74:1911–1918",
"6. Mollaret P, Goulon M. Le coma dépassé. Rev Neurol (Paris). 1959;101:3-15 [Original description]",
"7. A Definition of Irreversible Coma: Report of the Ad Hoc Committee of Harvard Medical School. JAMA. 1968;205:337–340",
];
refs.forEach((ref, i) => {
s.addText(ref, {
x: 0.4, y: 1.05 + i * 0.63, w: 9.4, h: 0.55,
fontSize: 11, color: i === 3 ? C.gold : C.offWhite,
fontFace: "Calibri", valign: "middle"
});
});
s.addShape(pres.ShapeType.rect, {
x: 0, y: 5.25, w: 10, h: 0.375, fill: { color: C.teal }
});
s.addText("Brain Death: Concepts & Criteria for Diagnosis | 1st Year MBBS Physiology Seminar", {
x: 0.3, y: 5.27, w: 9.4, h: 0.35,
fontSize: 11, color: C.navy, bold: true, fontFace: "Calibri", align: "center", valign: "middle"
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 26 — THANK YOU
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 2.2, w: 10, h: 0.08, fill: { color: C.teal } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 3.4, w: 10, h: 0.08, fill: { color: C.teal } });
s.addShape(pres.ShapeType.ellipse, {
x: 3.8, y: 0.3, w: 2.4, h: 2.4,
fill: { color: "12294A" }, line: { color: C.teal, width: 2 }
});
s.addText("THANK YOU", {
x: 0.5, y: 2.4, w: 9, h: 0.9,
fontSize: 52, bold: true, color: C.white, align: "center", fontFace: "Calibri", charSpacing: 8
});
s.addText("Questions & Discussion", {
x: 0.5, y: 3.5, w: 9, h: 0.55,
fontSize: 22, color: C.gold, align: "center", fontFace: "Calibri", italic: true
});
s.addText("Brain Death: Concepts & Criteria for Diagnosis\n1st Year MBBS — Physiology Seminar", {
x: 0.5, y: 4.2, w: 9, h: 0.8,
fontSize: 14, color: C.lightTeal, align: "center", fontFace: "Calibri"
});
}
// ── Write file ────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/brain-death-ppt/Brain_Death_Seminar.pptx" })
.then(() => console.log("SUCCESS: Brain_Death_Seminar.pptx written"))
.catch(e => { console.error("ERROR:", e); process.exit(1); });
Running Command
cd /home/daytona/workspace/brain-death-ppt && node generate.js 2>&1
Running Command
ls -lh /home/daytona/workspace/brain-death-ppt/Brain_Death_Seminar.pptx
Your seminar presentation is ready!
Brain Death Seminar
Presentation · PPTX
What's inside (26 slides, 10 sections):
| Slide(s) | Content |
|---|---|
| 1 | Title slide — bold navy/teal/gold design |
| 2 | Visual roadmap of all 10 sections |
| 3-4 | Historical Background (timeline: 1950s → 2023) |
| 5-6 | Definition & the 3-component concept |
| 7-8 | Physiological Basis — brainstem functions, why brain death = death, common causes |
| 9-10 | Prerequisites — all 6 confounders that must be excluded |
| 11-12 | Three Clinical Criteria — overview card layout |
| 13-14 | Apnea Test — step-by-step protocol (6 steps) |
| 15 | Apnea Test physiology — why CO₂, abort criteria, exclusions |
| 16-17 | Brainstem Reflexes — full table with CN pathways, test method, anatomy level |
| 18 | Spinal Reflexes & Lazarus Sign — common confusion point for 1st years |
| 19-20 | Ancillary/Confirmatory Tests (EEG, angiography, TCD, SPECT) |
| 21-22 | Ethical, Legal & Cultural Dimensions |
| 23-24 | Summary — 8-point key take-aways + diagnostic formula |
| 25 | References (Adams & Victor, Plum & Posner, AAN 2023, Harvard 1968) |
| 26 | Thank You / Q&A slide |
Design: Deep navy background dominant, teal + gold accents, red for danger/absent findings — all on 16:9 widescreen format. Calibri throughout for clean academic look.
Physiological basis of brain death
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
I now have rich content from multiple authoritative sources plus key diagrams. Let me compile the comprehensive answer.
Physiological Basis of Brain Death
Brain death is not an arbitrary clinical label - it is the end point of a chain of well-defined physiological failures. Understanding it requires knowing how consciousness is generated and maintained, how the brain tolerates (and fails to tolerate) injury, and what happens when the brainstem's vital centers permanently cease to function.
1. Normal Physiology: How the Brain Stays Alive and Conscious
1a. The Ascending Reticular Activating System (ARAS) - The Seat of Consciousness
Consciousness has two components - arousal (wakefulness) and awareness (cortical content). Arousal depends entirely on the Ascending Reticular Activating System (ARAS), first described in animals by Moruzzi and Magoun in 1949.
The ARAS is a complex polysynaptic fiber network located in the paramedian tegmental region of the upper pons and midbrain. It extends upward through the midbrain to the posterior hypothalamus and thalamic reticular formation. From the thalamus, diffuse thalamocortical projections then regulate and coordinate cortical activity.
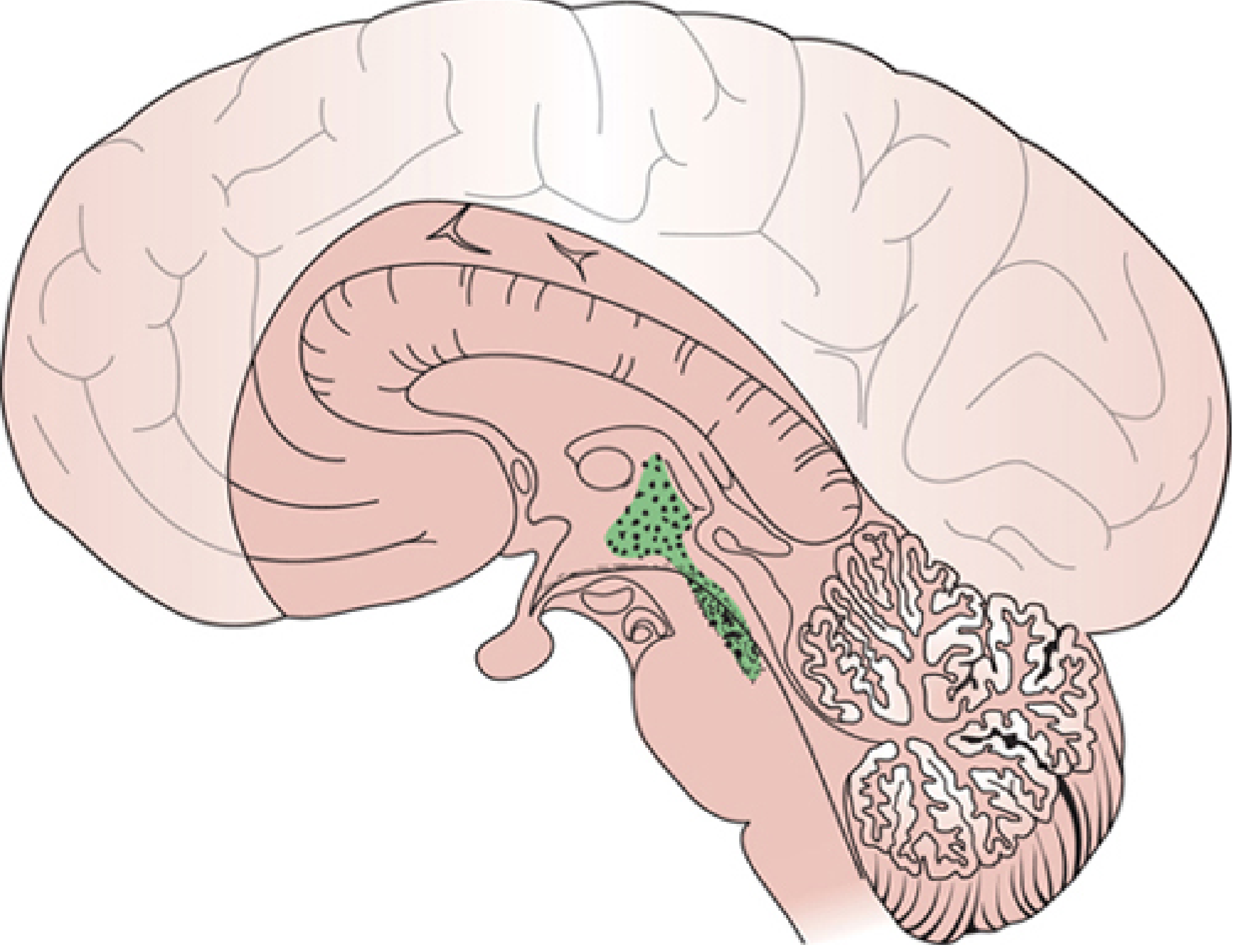
Key physiological point: Sensory stimuli "play on" this ARAS network to maintain wakefulness. Sedative drugs suppress consciousness precisely by interfering with the synaptic network of the ARAS. Destruction of the ARAS - whether from direct structural injury or ischemia - instantly abolishes arousal and produces coma.
1b. Vital Brainstem Centers
The brainstem is not merely a relay station - it houses the primary control centers for all life-sustaining autonomic and reflex functions:
| Brainstem Level | Center | Function |
|---|---|---|
| Medulla oblongata | Pre-Bötzinger complex / Respiratory rhythmicity center | Generates the rhythm of breathing (inspiratory drive) |
| Medulla | Vasomotor center (nucleus tractus solitarius, RVLM) | Controls heart rate, blood pressure, vascular tone |
| Medulla | Dorsal vagal nucleus | Parasympathetic cardiac innervation |
| Midbrain/Pons | ARAS (reticular formation) | Arousal, consciousness, sleep-wake cycle |
| Midbrain | CN III nucleus (Edinger-Westphal) | Pupillary constriction (parasympathetic) |
| Pons | Pontine gaze center (PPRF), CN VI nucleus | Horizontal eye movements |
| Medulla | Nucleus ambiguus | Gag, cough, swallowing (CN IX, X) |
| Hypothalamus | Thermoregulatory center | Body temperature control |
| Hypothalamus | Supraoptic / paraventricular nuclei | ADH release (water balance) |
The physiological reason brain death = death: When the entire brainstem is destroyed, spontaneous respiration ceases permanently. Without ventilatory support, cardiac arrest follows within minutes from hypoxia. The cortex, having lost its arousal input from the ARAS, generates no consciousness. The organism cannot survive without indefinite mechanical and pharmacological support.
2. Cerebral Blood Flow and the Brain's Vulnerability
2a. The Brain's Metabolic Demands
The brain constitutes ~2% of body weight but consumes:
- ~20% of total body oxygen (cerebral metabolic rate of O₂ = CMRO₂ ~3.5 mL O₂/100g/min)
- ~25% of total body glucose (almost exclusively oxidative phosphorylation)
- Has virtually no energy stores - no significant glycogen, no fat reserves
This makes neurons exquisitely vulnerable to any interruption of substrate delivery. Neuronal electrical activity fails within seconds of oxygen deprivation; irreversible neuronal injury begins within 4-6 minutes of complete ischemia.
2b. Cerebral Perfusion Pressure and Autoregulation
CPP (Cerebral Perfusion Pressure) = MAP (Mean Arterial Pressure) - ICP (Intracranial Pressure)
Normally, cerebral autoregulation maintains constant cerebral blood flow (CBF ~50 mL/100g/min) across a wide MAP range (~50-150 mmHg) by dynamically adjusting cerebrovascular resistance. When ICP rises severely, CPP falls and, once it exceeds the capacity of autoregulation, CBF declines proportionally - leading to global cerebral ischemia.
3. Pathophysiology - How Catastrophic Injury Leads to Brain Death
3a. The Monro-Kellie Doctrine and ICP Crisis
The skull is a rigid, closed box. Its contents - brain parenchyma, blood, and CSF - are incompressible. Any additional volume (hemorrhage, edema, tumor) must displace an equal volume of CSF or venous blood.
Three phases of ICP response to increasing mass volume:
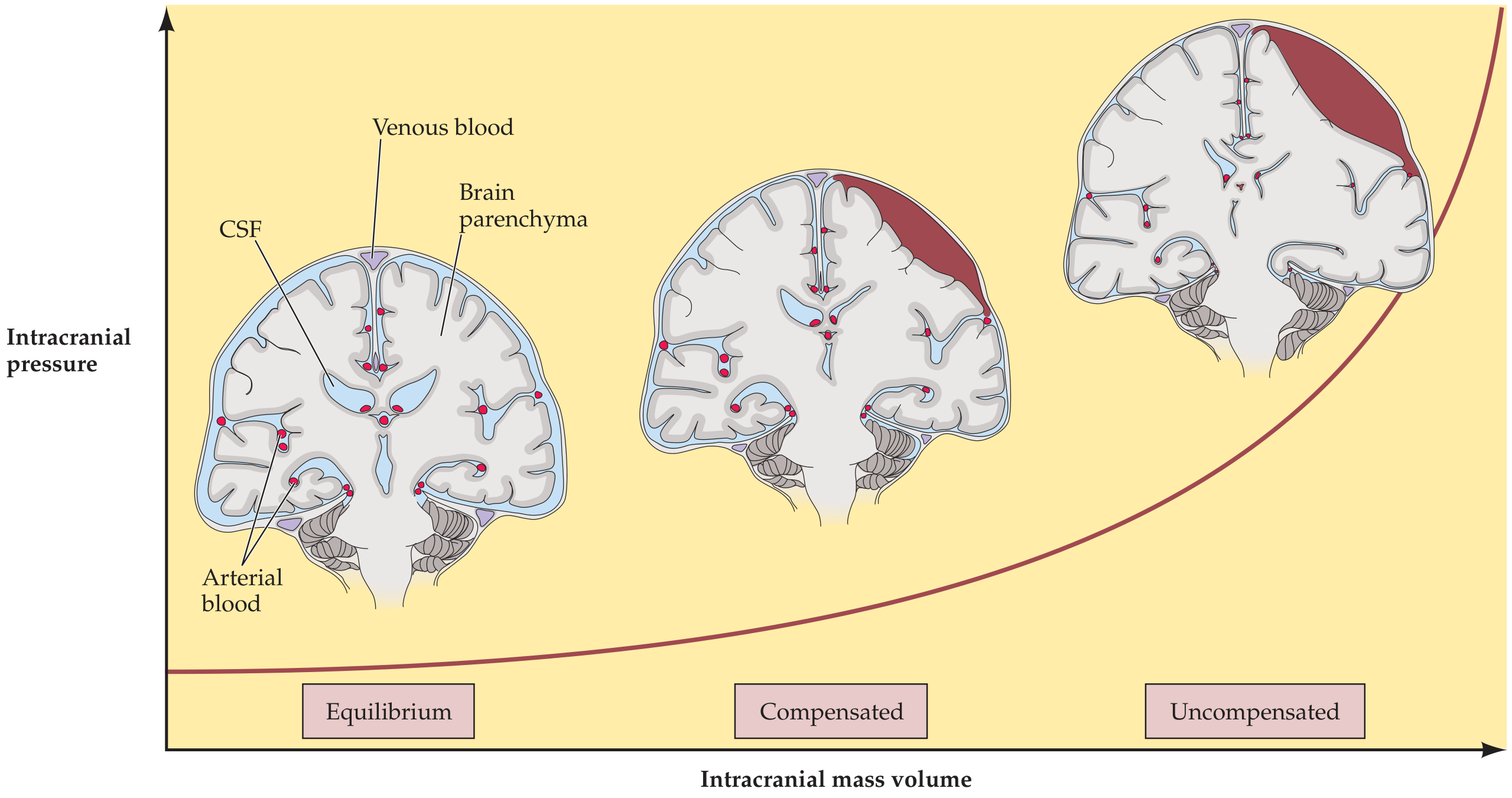
- Equilibrium (compensated): Small increases in volume displace CSF and venous blood. ICP remains near-normal (5-15 mmHg).
- Compensated (early decompensation): Compensatory reserve is exhausted. ICP begins to rise.
- Uncompensated: Any further volume increase causes a steep, exponential rise in ICP, drastically reducing CPP and triggering global cerebral ischemia and herniation.
3b. Transtentorial (Uncal) Herniation
As supratentorial pressure builds, the medial temporal lobe (uncus) herniates downward through the tentorial notch, compressing the midbrain. This produces a sequential, rostral-to-caudal "descending" pattern of brainstem failure (the Plum & Posner central herniation syndrome):
| Stage | Structure Affected | Clinical Signs |
|---|---|---|
| Diencephalic | Hypothalamus, thalamus | Drowsiness, small reactive pupils, Cheyne-Stokes respiration |
| Midbrain | Midbrain tegmentum, CN III | Fixed mid-position pupils (4-5 mm), loss of oculocephalic reflex, central neurogenic hyperventilation |
| Pontine | Pontine tegmentum | Pinpoint pupils (preserved - pontine sympatholytics), absent caloric responses, abnormal respirations |
| Medullary | Medulla oblongata | Fixed dilated pupils, ataxic/gasping respirations → apnea, cardiovascular collapse |
Once the medulla is destroyed, there is no respiratory drive regardless of any CO₂ or pH stimulus - this is the physiological basis of the apnea test.
3c. The "No-Flow" State - When ICP Equals MAP
In the terminal phase of catastrophic brain injury, ICP rises to match or exceed MAP:
CPP = MAP - ICP → CPP approaches ZERO
At this point, cerebral blood flow ceases entirely - a state demonstrable by radionuclide scanning (absent brain perfusion = "hollow skull") or by transcranial Doppler (to-and-fro "Pendelfluss" pattern reflecting oscillating blood at the skull base with no net forward flow). This is the haemodynamic basis of brain death.
3d. Cellular Mechanisms of Irreversible Neuronal Death
When CBF ceases:
- ATP depletion (within seconds): Na⁺/K⁺-ATPase fails → massive Na⁺ influx → cytotoxic edema
- Glutamate excitotoxicity: Depolarization triggers massive glutamate release from presynaptic terminals → NMDA receptor overactivation → Ca²⁺ flooding into neurons
- Calcium-mediated destruction: Activated proteases (calpains), lipases (phospholipase A₂), endonucleases destroy cell membranes, mitochondria, and DNA
- Mitochondrial failure: Loss of oxidative phosphorylation → irreversible energy failure
- Neuronal necrosis and apoptosis: Within minutes of complete ischemia, irreversible neuronal death begins
Once neurons in the ARAS, the medullary respiratory centers, and the brainstem reflex nuclei have undergone this irreversible necrosis, no recovery of function is possible - regardless of any subsequent restoration of circulation.
4. Physiological Basis of Each Diagnostic Sign
| Clinical Sign | Physiological Explanation |
|---|---|
| Deep unresponsive coma | Complete destruction of ARAS in the midbrain/upper pons; no arousal signal reaches the cortex |
| Fixed dilated pupils | Destruction of Edinger-Westphal nucleus (CN III parasympathetics) removes tonic pupilloconstriction; sympathetic dilator tone from the cervical cord persists unopposed → mydriasis |
| Absent corneal reflex | Pontine CN V (afferent) → CN VII (efferent) arc is broken by pontine destruction |
| Absent oculovestibular reflex | Medullary-pontine vestibular nuclei (CN VIII → CN III/VI loop) are destroyed; no eye movement to ice-water caloric stimulation |
| Absent gag/cough | Medullary nucleus ambiguus (CN IX, X) is destroyed |
| Positive apnea test | Pre-Bötzinger complex and medullary respiratory rhythmicity centers are destroyed; PaCO₂ rising far above the normal threshold of ~40 mmHg (even to 60+ mmHg) produces no inspiratory effort |
| Diabetes insipidus (in many cases) | Destruction of hypothalamic supraoptic/paraventricular nuclei → loss of ADH → massive dilute urine output (present in many, not all, brain-dead patients) |
| Spinal reflexes preserved | Spinal cord is NOT the brain; segmental spinal reflex arcs (DTRs, plantar responses, Lazarus sign) are mediated entirely at the spinal cord level and do not require supraspinal input |
5. The Apnea Test - Physiological Mechanism in Detail
The medullary respiratory center (dorsal and ventral respiratory groups, pre-Bötzinger complex) responds primarily to:
- Rising PaCO₂ → H⁺ ions sensed by central chemoreceptors on the ventral surface of the medulla
- Falling PaO₂ sensed by peripheral chemoreceptors (carotid and aortic bodies)
In a living brainstem, a PaCO₂ of even 45-50 mmHg is a strong stimulus to breathe. The apnea test uses a suprathreshold PaCO₂ of ≥ 60 mmHg (an unmistakably maximal stimulus) as proof that the medullary centers cannot respond. The absence of any respiratory effort at this level confirms medullary destruction - the definitive physiological evidence of brain death.
CO₂ rises at approximately 2.5 mmHg per minute at normothermia after ventilator disconnection. This rate is used to calculate the minimum observation time needed.
6. Why Cardiac Function Persists After Brain Death
This is the most counterintuitive aspect of brain death and the source of much public misunderstanding. The heart has its own intrinsic pacemaker (sinoatrial node) that generates action potentials independently of the brain. The cardiac conduction system does not require brainstem input to maintain rhythm. What the brain provides is autonomic modulation (sympathetic acceleration via the cardiac sympathetics; parasympathetic slowing via the vagus from the dorsal vagal nucleus). Loss of this central modulation causes:
- Loss of heart rate variability
- Progressive cardiovascular instability (neurogenic hypotension due to loss of vasomotor tone)
- Eventual cardiac arrest, typically within days to weeks, even with full ventilatory and vasopressor support
This explains why in brain death: the heart beats, the lungs can be ventilated, the skin stays warm - but the brain is irreversibly non-functional.
Summary
Catastrophic Brain Injury
↓
Rising ICP → Falling CPP → Cerebral Ischemia
↓
Excitotoxicity → Ca²⁺ overload → ATP depletion → Neuronal necrosis
↓
Destruction of ARAS → permanent coma (no arousal)
Destruction of brainstem reflexes → absent cranial nerve responses
Destruction of medullary respiratory center → permanent apnea
↓
ICP = MAP → CPP = 0 → No cerebral blood flow ("hollow skull")
↓
BRAIN DEATH = irreversible cessation of all brain function
↓
Without support: hypoxic cardiac arrest within minutes
With support: cardiovascular collapse within days-weeks
Sources:
- Localization in Clinical Neurology, 8e (ARAS anatomy and coma substrate)
- Neuroanatomy through Clinical Cases, 3e (ICP-volume curve, herniation)
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma (herniation syndromes, brain death physiology)
- Adams and Victor's Principles of Neurology, 12e (brainstem centers, apnea test rationale)
- Bradley and Daroff's Neurology in Clinical Practice, 8e (prerequisites, clinical criteria)
What is thalamic reticular formation simpler way for 3 marks
Finding Sources
Reading File
Finding Sources
Reading File
Here is a clean, exam-ready 3-mark answer:
Thalamic Reticular Formation (Thalamic Reticular Nucleus - TRN)
What it is
The thalamic reticular nucleus is a thin shell of inhibitory (GABAergic) neurons that wraps around the outer surface of the thalamus like a net or cage.
- It is NOT part of the thalamus itself - it is a separate layer sitting between the thalamus and the internal capsule.
- It receives inputs from the cerebral cortex, thalamic relay nuclei, and brainstem arousal systems (ARAS).
- It sends inhibitory (GABA) projections back into the thalamus.
What it does (3 key functions)
-
Gating of sensory information - Acts like a "filter" or "gatekeeper." It selectively inhibits certain thalamic relay nuclei, controlling which sensory signals get through to the cortex and which are blocked. This is the physical basis of selective attention.
-
Regulation of consciousness and arousal - The ARAS (in the brainstem) projects upward through the TRN to reach the cortex. The TRN modulates this arousal signal, helping coordinate the sleep-wake cycle, attention, and the level of cortical activity.
-
Sleep spindle generation - During non-REM sleep, the TRN generates characteristic sleep spindles (bursts of 12-14 Hz EEG activity) by producing rhythmic inhibitory bursts that oscillate with thalamic relay neurons.
Simple analogy
Think of the TRN as a volume control knob on a radio - the ARAS is the signal coming in from the transmitter (brainstem), the thalamus is the receiver, and the TRN adjusts how much signal reaches the speaker (cortex).
In the context of brain death: Destruction of the upper brainstem ARAS removes all input to the TRN and thalamus → no thalamocortical activation → permanent loss of consciousness.
(Source: Neuroanatomy through Clinical Cases, 3e)
Glasgow coma scale
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive content from multiple textbooks. Here is the full answer:
Glasgow Coma Scale (GCS)
Introduction
The Glasgow Coma Scale was originally developed by Teasdale and Jennett in 1974 as a standardized, reproducible tool to assess the level of consciousness following traumatic brain injury (TBI). It is now universally applied to all patients with impaired consciousness, regardless of cause.
It assesses three independent behavioral responses - eye opening, verbal response, and motor response - and sums them for a total score.
The Three Components
1. Eye Opening (E) - Maximum 4
| Score | Response |
|---|---|
| 4 | Opens eyes spontaneously |
| 3 | Opens eyes to verbal command (speech) |
| 2 | Opens eyes to pain (noxious stimulus) |
| 1 | No eye opening |
2. Verbal Response (V) - Maximum 5
| Score | Response |
|---|---|
| 5 | Oriented - knows person, place, time |
| 4 | Confused - conversational but disoriented |
| 3 | Inappropriate words - random words, no sentences |
| 2 | Incomprehensible sounds - moaning, groaning, no words |
| 1 | No verbal response |
3. Motor Response (M) - Maximum 6
| Score | Response |
|---|---|
| 6 | Obeys commands - follows two-step instruction |
| 5 | Localizes pain - moves hand toward stimulus to push it away |
| 4 | Withdraws from pain - pulls limb away (normal flexion) |
| 3 | Flexor posturing (Decorticate) - abnormal flexion of arms, wrists |
| 2 | Extensor posturing (Decerebrate) - arms extend and pronate |
| 1 | No motor response |
Memory aid: "EMV" or "3-4-5-6 rule" - Eye (max 4), Verbal (max 5), Motor (max 6). Total = 3 to 15.
Total Score and Interpretation
| Total GCS Score | Severity of Brain Injury |
|---|---|
| 13 - 15 | Mild TBI (minor head injury) |
| 9 - 12 | Moderate TBI |
| 3 - 8 | Severe TBI (deep coma) |
| 3 | Lowest possible score (no response in any component) |
| 15 | Normal |
GCS ≤ 8 = coma - indicates need for airway protection (intubation threshold)
Understanding the Motor Responses (Important for Physiology)
The motor score has the greatest prognostic weight of the three components and reflects the level of brain/brainstem function:
Decorticate posturing (M3 - flexion):
- Arms flex at elbow and wrist; legs extend
- Indicates damage above the brainstem at the level of the internal capsule or cerebral hemispheres
- Cortex cannot inhibit the thalamus/basal ganglia → abnormal flexor pattern
Decerebrate posturing (M2 - extension):
- Arms extend and internally rotate; legs extend and plantarflex
- Indicates damage at the midbrain or upper pons level - the lesion is below the red nucleus
- More ominous than decorticate; indicates impending herniation
- Reflects release of the pontine reticulospinal tract from cortical control
No response (M1):
- Indicates complete loss of motor output from brainstem
- Seen in brain death (though note: spinal reflexes may still cause movement)
Practical Points
Intubated patients: Cannot be assessed for verbal response. Score is written with "T" instead (e.g., GCS 8T). Best possible score = 11T (E4 + V-T + M6).
Timing: Should be measured:
- Before administering sedatives or neuromuscular blocking agents
- Every 30 minutes in the prehospital setting
- Whenever mental status changes
Best eye = use the better eye. Best motor = use the best limb response.
Limitations of GCS
- Does not assess brainstem function (no pupil, caloric, or corneal reflex testing) - the FOUR score was developed to address this
- Unreliable in intubated patients (verbal score lost)
- Cannot detect subtle changes in neurological status
- Confounders: Drugs (opioids, benzodiazepines), alcohol, metabolic encephalopathy, and hypoglycemia can all lower the GCS without structural brain injury - a patient with opioid overdose may have GCS 3 but recover to GCS 15 after naloxone
- Not validated in children <2 years (modified pediatric GCS is used)
- Language barrier and hearing impairment affect the verbal score
- Interrater variability for the motor score (localizing vs. withdrawal can be difficult to distinguish)
GCS in the Context of Brain Death
- Brain death corresponds to GCS = 3 (no eye opening, no verbal response, no motor response)
- However, GCS 3 alone does NOT diagnose brain death - it simply indicates deep unresponsive coma
- Brain death additionally requires absent brainstem reflexes and a positive apnea test
- Spinal reflexes (e.g., Lazarus sign) can persist even at GCS 3 and do not affect the GCS score
GCS vs. FOUR Score (Brief Comparison)
| Feature | GCS | FOUR Score |
|---|---|---|
| Brainstem reflexes | Not included | Included (pupil + corneal) |
| Breathing patterns | Not assessed | Assessed |
| Intubated patients | Limited (verbal lost) | Better suited |
| Eye tracking | Not assessed | Included |
| Range | 3 - 15 | 0 - 16 |
Summary Formula
GCS = Eye (1-4) + Verbal (1-5) + Motor (1-6)
Range: 3 (worst) to 15 (normal)
≤ 8 = Coma / severe injury → secure airway
Motor score carries greatest prognostic value
Sources: Sabiston Textbook of Surgery, 21e - Schwartz's Principles of Surgery, 11e - Plum and Posner's Diagnosis and Treatment of Stupor and Coma - Rosen's Emergency Medicine
Why is there need to declare brain dead
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.