What is Deep vein thrombosis ?
Reading File
Finding Sources
Searching PubMed
"deep vein thrombosis"[MeSH Terms] AND diagnosis AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of Deep Vein Thrombosis (DVT) based on authoritative medical textbooks.
Deep Vein Thrombosis (DVT)
Definition
Deep Vein Thrombosis is the formation of a blood clot (thrombus) within a deep vein, most commonly in the lower limbs (calf, femoral, popliteal, or iliac veins). When complicated by pulmonary embolism (PE), it can be potentially fatal.
- ROSEN's Emergency Medicine, p. 1196
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 345
Pathophysiology - Virchow's Triad
Three major factors predispose to DVT formation:
- Venous stasis - reduced or stagnant blood flow (immobility, reduced muscular calf pump, obstruction to flow)
- Vascular wall injury - venous trauma damages vessel walls and promotes thrombus formation
- Hypercoagulability - abnormal levels of clotting factors such as antithrombin III, protein C, and protein S
- Gray's Anatomy for Students, p. 785
Anatomy of Relevant Veins
DVT most commonly affects the deep veins of the leg:
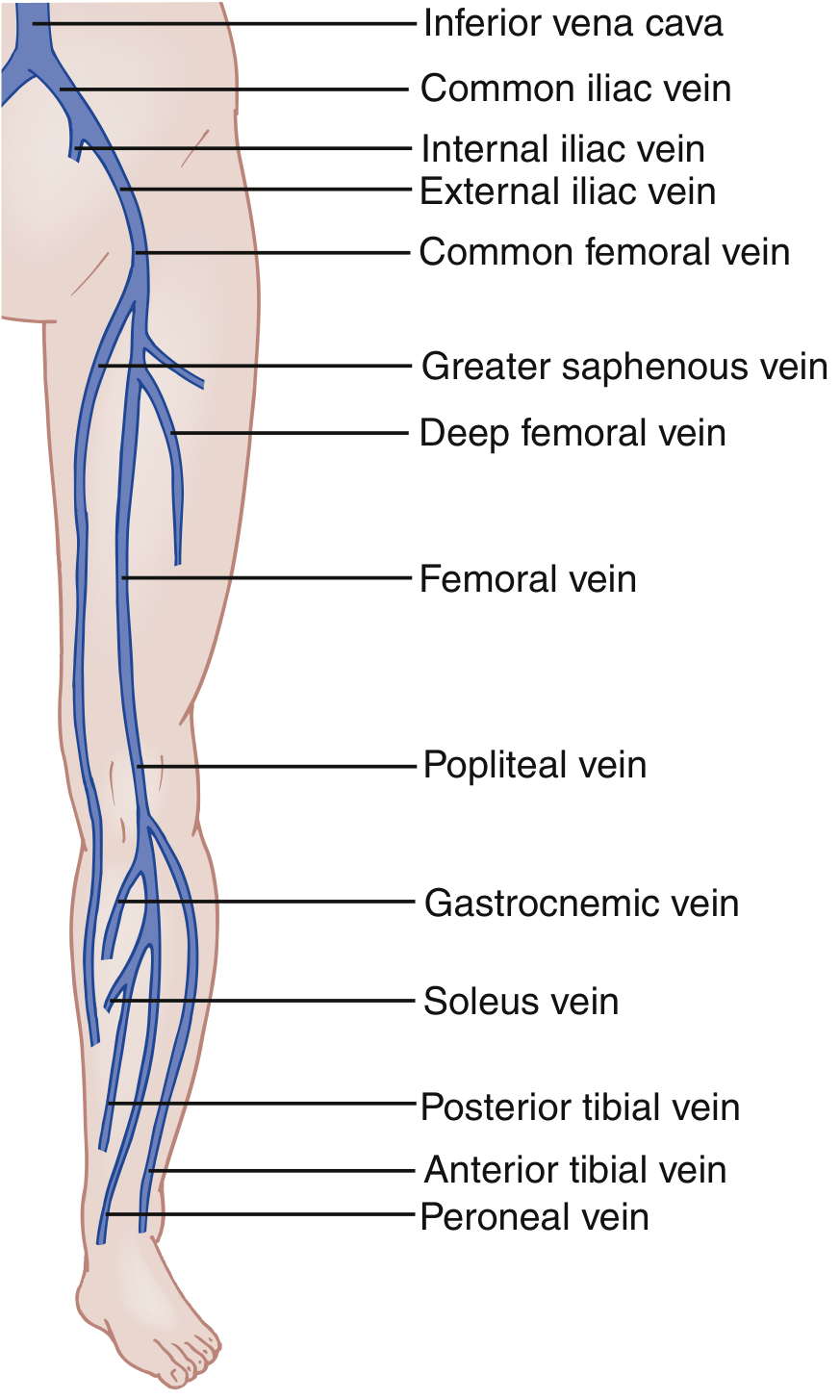
Key veins involved: common femoral, femoral, popliteal, posterior tibial, peroneal, and gastrocnemius veins. Upper extremity DVT occurs most often when an indwelling catheter is present; in young athletes, repetitive arm motion causes Paget-Schroetter syndrome (effort-induced subclavian vein DVT).
Risk Factors
| Risk Level | Surgical Procedures |
|---|---|
| Low | Maxillofacial, neurosurgery, cardiothoracic |
| Medium | Inguinal hernia, abdominal, gynaecological, urological surgery |
| High | Pelvic surgery, total knee/hip replacement |
Other risk factors include: active cancer, immobility/bed rest, recent major surgery, pregnancy (the gravid uterus can compress the left external iliac vein), paralysis, and inherited/acquired thrombophilias.
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 345
Clinical Features
Symptoms and signs include:
- Unilateral leg pain and swelling (calf pain is most common)
- Warmth, redness, and engorged superficial veins of the affected limb
- Tenderness on palpation along the deep venous distribution
- Homans' sign - calf pain on dorsiflexion of the foot (positive, but neither sensitive nor specific)
- Rarely, a palpable venous cord
Most patients will show no physical signs at all, making clinical suspicion essential.
-
Because the left iliac vein is vulnerable to compression by the left iliac artery (May-Thurner syndrome), DVT occurs slightly more frequently on the left.
-
Bilateral leg DVT is found in fewer than 10% of ED patients.
-
ROSEN's Emergency Medicine, p. 1196-1197
-
Bailey and Love's Short Practice of Surgery, p. 345
Differential Diagnosis
- Venous insufficiency
- Cellulitis (concurrent DVT found in only ~3% of cellulitis cases)
- Gastrocnemius muscle injury or Achilles tendon injury
- Ruptured Baker cyst (can mimic DVT in the calf/popliteal region)
- Calf muscle hematoma
- Systemic edema (e.g., heart failure causing asymmetric swelling)
Diagnosis
1. Wells DVT Score (Pre-test Probability)
The two-level Wells DVT Score is the most commonly used clinical decision tool:
| Clinical Feature | Points |
|---|---|
| Active cancer | 1 |
| Paralysis/paresis or recent plaster immobilisation | 1 |
| Bedridden ≥3 days or major surgery within 12 weeks | 1 |
| Localized tenderness along deep vein | 1 |
| Entire leg swollen | 1 |
| Calf swelling >3 cm compared to asymptomatic leg | 1 |
| Pitting oedema confined to symptomatic leg | 1 |
| Collateral (non-varicose) superficial veins | 1 |
| Previously documented DVT | 1 |
| Alternative diagnosis at least as likely | -2 |
- Score ≥2: DVT likely (High PTP)
- Score <2: DVT unlikely (Low PTP)
In pregnant women, the LEFt score is used: 1 point each for Left leg suspicion, Edema, and First trimester.
2. D-Dimer
- Measures breakdown of cross-linked fibrin from any intravascular thrombus
- Normal D-dimer with low PTP excludes proximal DVT with ~92% sensitivity
- Standard cutoff: >500 ng/mL = abnormal
- Age-adjusted cutoff: Age × 10 ng/mL (e.g., 80-year-old: <800 ng/mL considered negative), maintaining ~95% sensitivity
3. Venous Duplex Ultrasound
-
Gold standard for diagnosis
-
Key findings for DVT: no flow, non-compressible vein, no augmentation with calf compression, no respiratory phasicity
-
A 3-point ultrasound covers common femoral, femoral, and popliteal veins
-
Whole-leg ultrasound adds tibial, peroneal, and gastrocnemius veins
-
ROSEN's Emergency Medicine, p. 1196-1197
-
Gray's Anatomy for Students, p. 785
Treatment
Anticoagulation (First-line)
-
Initial therapy: Treatment-dose subcutaneous LMWH (low-molecular-weight heparin)
- Patients with significant renal impairment: IV unfractionated heparin
- HIT (heparin-induced thrombocytopenia): fondaparinux (anti-Xa) or bivalirudin (direct thrombin inhibitor)
-
Long-term oral anticoagulation for at least 3 months (longer if risk factors persist or recurrent DVT):
- NOACs (preferred): rivaroxaban, apixaban (factor Xa inhibitors) or dabigatran (thrombin inhibitor)
- These are equally effective as warfarin but with fewer major bleeding complications
IVC Filter
- For patients who cannot be safely anticoagulated (high bleeding risk)
- Temporary/retrievable filters are used until anticoagulation is safe or embolisation risk subsides
Endovascular Intervention
-
Thrombus removal, thrombolysis, and stenting are increasingly used for acute DVT, particularly iliofemoral thrombosis
-
Aim: restore patency and reduce risk of post-thrombotic syndrome (chronic leg swelling, pain, skin changes)
-
Bailey and Love's Short Practice of Surgery, 28th Ed., p. 345
Complications
| Complication | Description |
|---|---|
| Pulmonary Embolism (PE) | Clot breaks off and lodges in pulmonary arteries - can be fatal |
| Post-thrombotic syndrome | Chronic venous insufficiency, leg swelling, pain, skin ulceration |
| Phlegmasia cerulea dolens | Massive DVT causing venous gangrene (rare) |
Small pulmonary emboli cause pleuritic chest pain; large emboli can cause sudden cardiovascular collapse. The pulmonary embolism appears as a filling defect on CT pulmonary angiography (CTPA).
Prevention
All surgical patients should be risk-stratified within 24 hours of admission. Prevention methods include:
-
Compression stockings (avoid in peripheral arterial disease, neuropathy)
-
Pneumatic calf compression pumps
-
Pharmacological prophylaxis (LMWH)
-
Bailey and Love's Short Practice of Surgery, 28th Ed., p. 344-345
Sources: ROSEN's Emergency Medicine 9th Ed. | Bailey and Love's Short Practice of Surgery 28th Ed. | Gray's Anatomy for Students
Whatvis cortical vein thrombosis
Finding Sources
Searching PubMed
"cerebral venous thrombosis"[MeSH Terms] AND management
Finding Sources
Searching PubMed
"cerebral venous thrombosis"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Cortical Vein Thrombosis (also known as Cerebral Venous Thrombosis / CVT).
Cortical Vein Thrombosis (Cerebral Venous Thrombosis)
Definition
Cortical vein thrombosis (CVT) is thrombosis occurring in the superficial cortical draining veins and/or the dural venous sinuses of the brain. It is a form of cerebrovascular disease where clot formation in the cerebral venous system causes venous hypertension, leading to brain edema, venous infarction (often hemorrhagic), and raised intracranial pressure.
It accounts for 0.5-1% of all strokes and is easily overlooked due to its variable, non-specific presentation.
- Bradley and Daroff's Neurology in Clinical Practice, p. 1409
- Grainger & Allison's Diagnostic Radiology, p. 1454
Classification
Intracranial venous thrombosis is broadly divided into:
| Type | Description |
|---|---|
| Dural venous sinus thrombosis | Thrombosis in major sinuses (sagittal, transverse, sigmoid) |
| Cortical/superficial vein thrombosis | Isolated thrombosis of surface draining veins |
| Deep cerebral vein thrombosis | Involves internal cerebral veins, vein of Galen, thalamus |
| Cavernous sinus thrombosis | Usually septic; presents with proptosis and ophthalmoplegia |
The superior sagittal sinus is the most frequently involved structure.
- Bradley and Daroff's Neurology, p. 1409
Causes and Risk Factors
CVT can be septic (infectious) or aseptic (non-infectious). The main causes include:
Infectious/Septic
- Facial, orbital, paranasal sinus, or middle ear infections
- Skull osteomyelitis, mastoiditis (lateral sinus thrombosis)
- Syphilis, varicella-zoster, HIV
Non-infectious/Aseptic
- Pregnancy and puerperium (peripartum period)
- Oral contraceptive pill use
- Smoking, dehydration
- Prothrombotic / hypercoagulable states:
- Factor V Leiden mutation
- Protein C or Protein S deficiency
- Antithrombin III deficiency
- Antiphospholipid antibody syndrome
- Hematologic disorders, disseminated cancer
- Vasculitis (especially Behcet's disease)
- SARS-CoV-2 infection (rare complication)
- Marasmus, dehydration, carcinoma
In approximately 15-20% of cases, no cause is found.
- Bradley and Daroff's Neurology, p. 1409-1410
- Goldman-Cecil Medicine, p. 2727
Epidemiology
- Mean age at presentation: ~39 years
- More common in young women, especially in the peripartum period
- Rare in children; about half of pediatric cases occur in neonates and young infants
- Rare overall (incidence ~0.08% among hospitalized patients)
Pathophysiology
Thrombosis in cortical veins or venous sinuses reduces venous drainage from brain parenchyma. This causes:
- Venous hypertension → cerebral edema (vasogenic, then cytotoxic)
- Reduced CSF absorption → raised intracranial pressure
- Venous infarction - often multifocal and bilateral, affecting gray matter AND subcortical white matter
- Hemorrhagic transformation (approximately 1/3 of cases develop intracerebral hemorrhage)
Unlike arterial infarcts, venous infarcts do NOT respect arterial territories and can be bilateral.
Clinical Features
Presentation ranges from insidious to acute. Key features:
| Feature | Details |
|---|---|
| Headache | Most common symptom; can be gradual (progressive over days-weeks) or "thunderclap" |
| Seizures | ~40% of patients; focal or generalized |
| Focal neurological deficits | Hemiparesis, paraparesis, sensory changes (bilateral leg weakness in sagittal sinus thrombosis) |
| Papilledema | Common - due to raised ICP |
| Altered mental status / coma | ~14% present with coma; severe cases |
| Transient visual obscurations | Due to raised ICP |
| Signs of raised ICP | Vomiting, blurred vision |
Suspect CVT in female patients under age 50 with stroke symptoms but no classic risk factors, unexplained new seizures, or refractory headaches. An elevated LP opening pressure in an appropriate clinical context should prompt venous imaging.
- Tintinalli's Emergency Medicine, p. 1293-1295
- ROSEN's Emergency Medicine, p. 1343
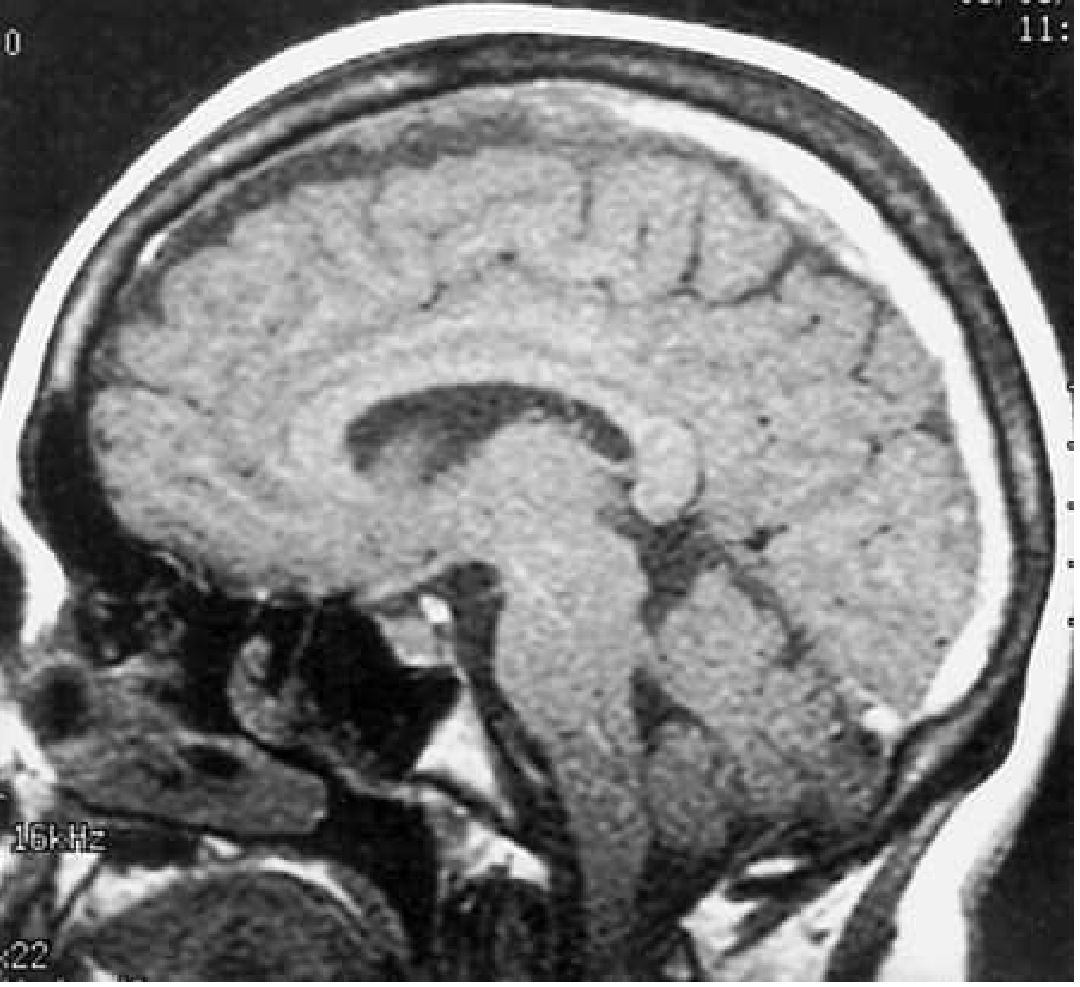
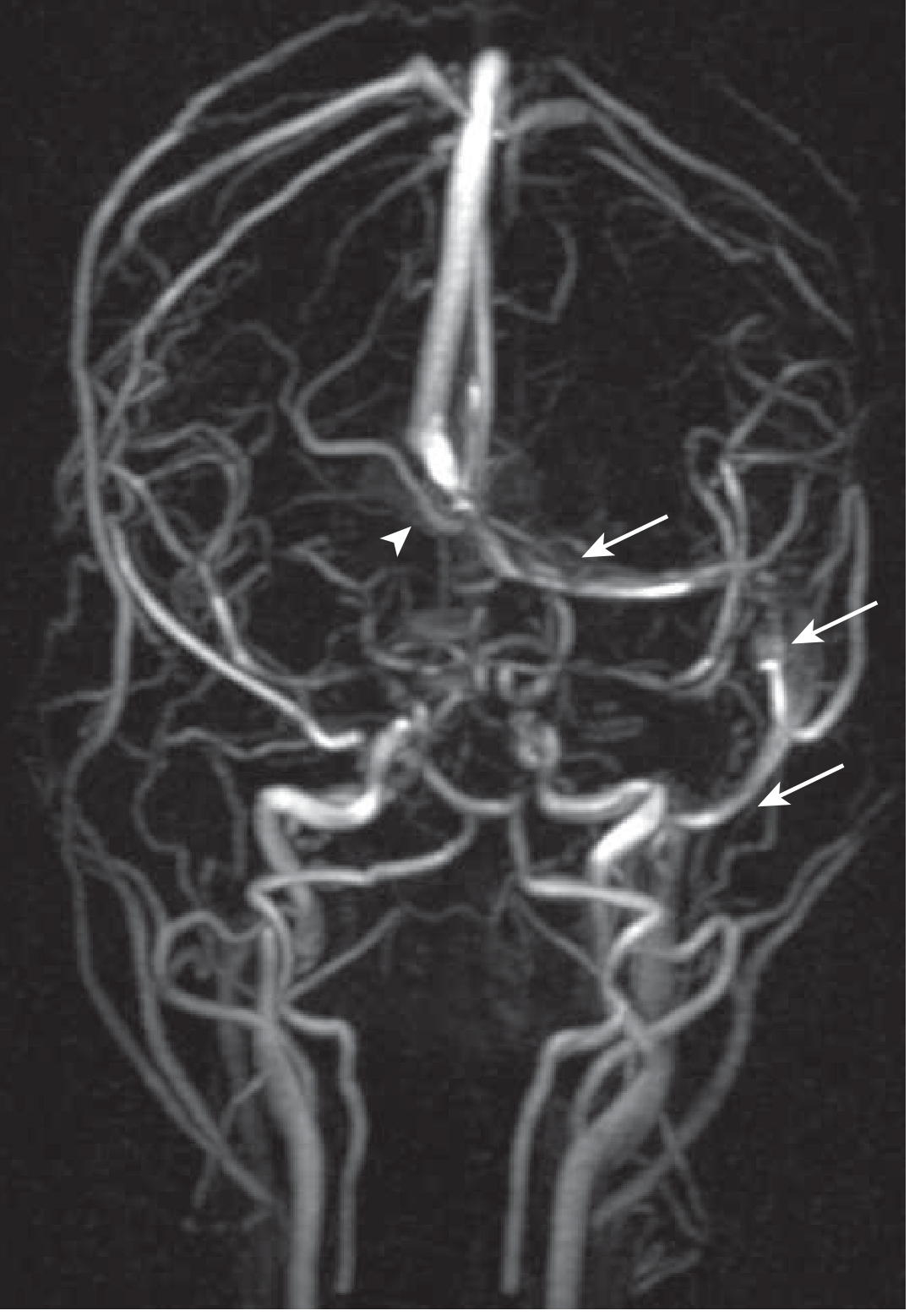
Imaging
MRI with MR Venography (MRV) - Gold Standard
- Loss of normal flow void in the affected sinus or vein
- Thrombosed vessel appears hyperintense on T1 and T2
- Very acute thrombus may be hypointense on T2 (can mimic flow void)
- MRV shows absent or severely reduced flow signal with irregularity and narrowing
CT / CT Venography
- Acutely thrombosed sinus appears hyperdense and expanded on non-contrast CT (NECT)
- Post-contrast CT: "Empty delta sign" - hypodense center within an enhancing periphery (classic for superior sagittal sinus thrombosis)
- Parenchymal changes: low-density edema, hemorrhagic infarction, small ventricles
- SWI (susceptibility-weighted imaging): "blooming" of thrombosed vein; serpiginous dilated collateral veins indicate venous congestion
Lumbar Puncture
-
Elevated opening pressure is a key finding
-
Can be safely performed in CVT (not contraindicated)
-
May show raised protein, red cells if hemorrhagic infarction present
-
Grainger & Allison's Diagnostic Radiology, p. 1454
-
Tintinalli's Emergency Medicine, p. 1295
Treatment
1. Anticoagulation (Primary Treatment)
- Acute phase: IV heparin or subcutaneous LMWH (preferred over unfractionated heparin - associated with lower mortality in one trial)
- Anticoagulation is recommended even if hemorrhagic infarction is already present - the benefit outweighs the risk
- Long-term: Warfarin (INR target 2.0-3.0) or newer anticoagulants for at least 3 months; longer if underlying cause persists
2. Adjunct Measures
- Seizure management: Prophylactic antiepileptics
- Raised ICP management: Head elevation, diuretics, acetazolamide
- Antibiotics: If septic etiology (now rare)
3. Endovascular / Surgical Options (Severe / Refractory Cases)
- Local thrombolysis (tPA) via direct venous infusion - reserved for stupor/coma and severely raised ICP
- Thrombectomy within the occluded sinus
- Decompressive craniectomy - for malignant brain edema with imminent herniation
Note: A small clinical trial found no benefit of adding endovascular therapy to medical therapy compared to medical therapy alone. Local thrombolysis is reserved for extreme cases.
- Bradley and Daroff's Neurology, p. 1409
- Adams and Victor's Principles of Neurology, 12th Ed., p. 1056
- Goldman-Cecil Medicine, p. 2729-2730
Prognosis
- Most patients who are treated early do well, with good neurological recovery
- Mortality remains significant in severe cases - large hemorrhagic venous infarctions found in 10-20% of cases
- Coma with multiple cerebral hemorrhages is usually fatal
- It may take weeks for headaches to remit even after starting heparin
- Outcomes in neonatal CVT depend on the extent of infarct and hemorrhage
Sources: Bradley and Daroff's Neurology in Clinical Practice | Tintinalli's Emergency Medicine | ROSEN's Emergency Medicine | Goldman-Cecil Medicine | Grainger & Allison's Diagnostic Radiology | Adams and Victor's Principles of Neurology 12th Ed.
What is the corresponding anatomy of vein of galen and other deep cortical vein
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Now I have comprehensive information. Here is a detailed anatomical account of the vein of Galen and the deep cerebral venous system.
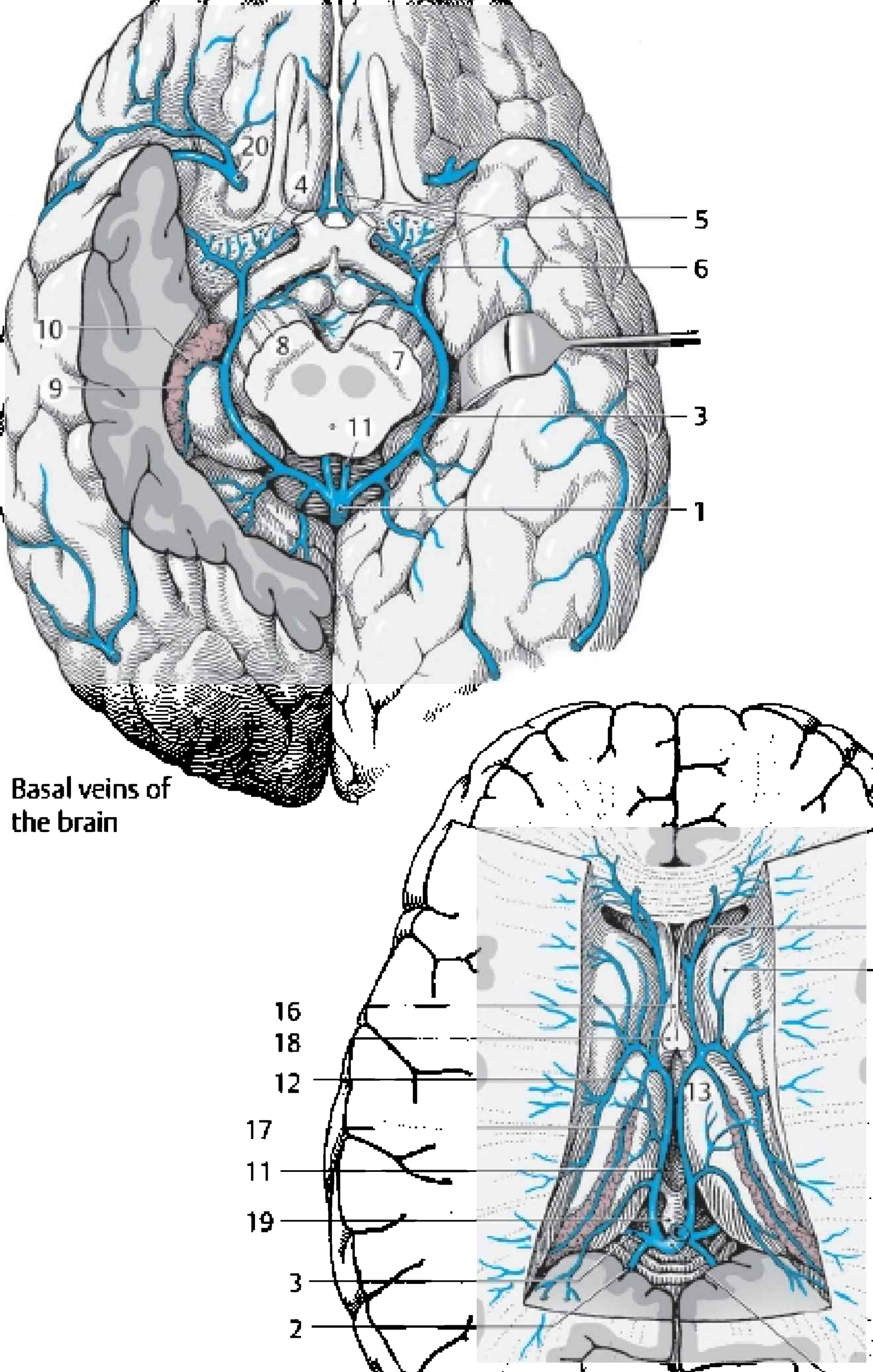
Anatomy of the Vein of Galen and Deep Cerebral Veins
The cerebral venous system is divided into two groups: superficial (cortical) veins and deep (subependymal) veins. The deep veins are remarkably constant in their organization and all ultimately drain into the great cerebral vein of Galen.
Overview: Superficial vs. Deep Venous Systems
| System | Drains | Empties Into |
|---|---|---|
| Superficial cortical veins | Cerebral cortex and subcortical white matter | Superior sagittal sinus, cavernous sinus |
| Deep subependymal veins | Basal ganglia, thalami, deep white matter, choroid plexus | Vein of Galen |
- Neuroanatomy through Clinical Cases, 3rd Ed.
- Grainger & Allison's Diagnostic Radiology, p. 1357
The Deep Cerebral Venous System - Step-by-Step Hierarchy
The deep veins form a very consistent and logical chain from the deep brain structures outward:
Medullary veins
↓
Septal vein + Thalamostriate vein
↓ (join at foramen of Monro = "venous angle")
Internal Cerebral Veins (paired, bilateral)
↓
+ Basal Veins of Rosenthal (bilateral)
↓
Great Cerebral Vein of Galen (midline)
↓
+ Inferior Sagittal Sinus
↓
Straight Sinus (Sinus Rectus)
↓
Confluence of Sinuses (Torcular Herophili)
↓
Transverse Sinuses → Sigmoid Sinuses → Internal Jugular Veins
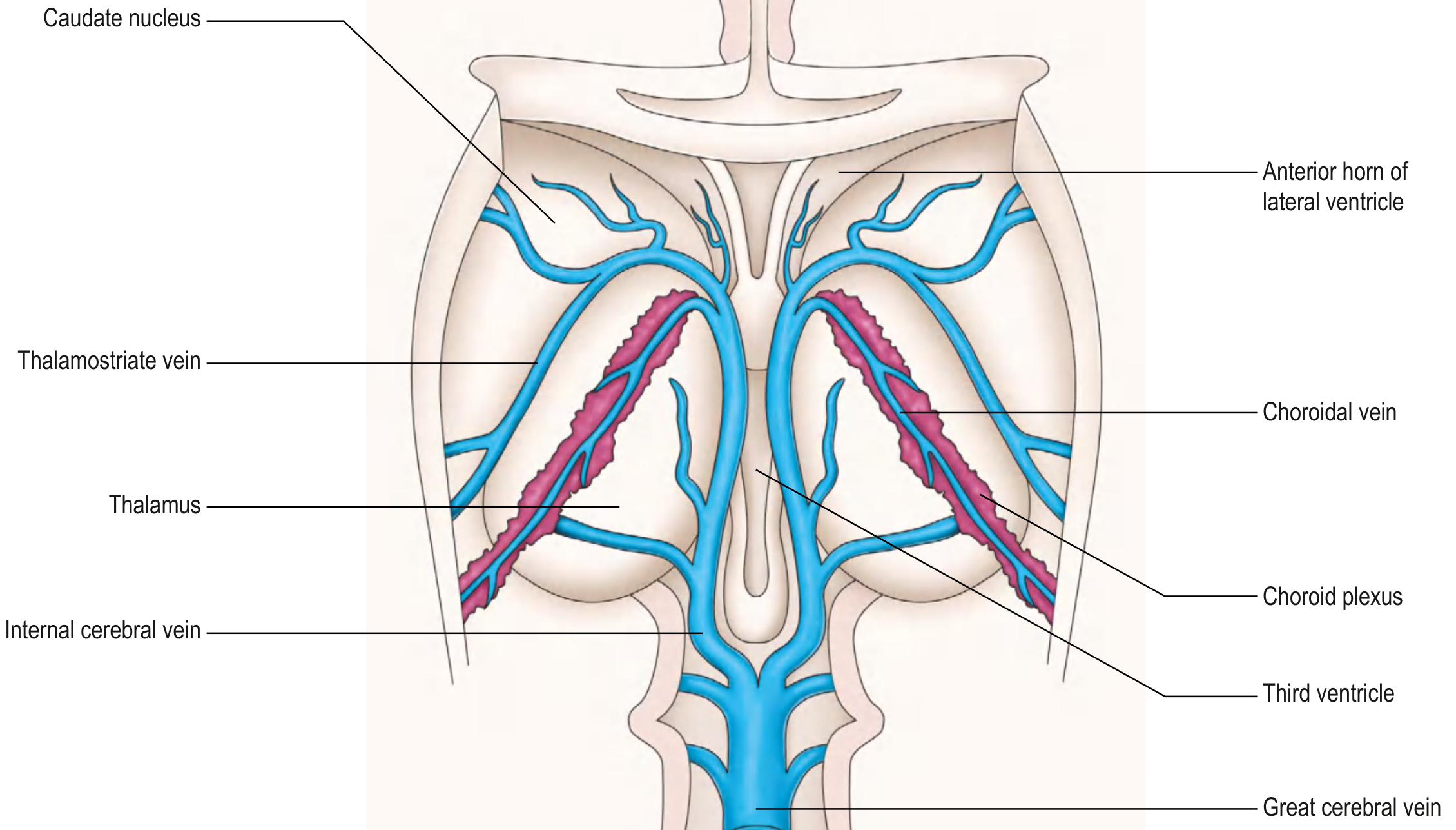
1. Thalamostriate Vein (Superior Thalamic Vein)
- Runs in the groove between the thalamus and the caudate nucleus, in the floor of the lateral ventricle
- Drains the thalamus, caudate nucleus, internal capsule, and adjacent deep white matter
- Travels posteriorly to reach the foramen of Monro (interventricular foramen)
- Joins the septal vein at the foramen of Monro to form the internal cerebral vein
- The point of junction (venous angle) is a key radiological landmark
Clinical note: In birth trauma, rupture of the thalamostriate vein can lead to intraventricular hemorrhage in newborns.
2. Septal Vein
- Courses directly posteriorly along the septum pellucidum
- Drains the frontal horn of the lateral ventricle and adjacent white matter
- Joins the thalamostriate vein at the foramen of Monro to form the internal cerebral vein
3. Internal Cerebral Veins (paired)
- Formed bilaterally at the foramina of Monro by union of the septal and thalamostriate veins
- Run posteriorly along the roof of the third ventricle, near the midline, enclosed within the velum interpositum (a fold of pia mater)
- Receive tributaries from the choroidal veins (draining the choroid plexus) along their course
- The two internal cerebral veins travel parallel to one another and unite posteriorly, below the splenium of the corpus callosum, to form the vein of Galen
4. Basal Vein of Rosenthal (paired)
- Formed near the anterior perforated substance by the union of the:
- Anterior cerebral vein (runs adjacent to the anterior cerebral artery / ACA)
- Deep middle cerebral vein (runs adjacent to the MCA in the Sylvian fissure)
- Courses posteriorly and medially, winding around the lateral aspect of the midbrain (through the ambient cistern)
- Drains the insula, basal ganglia (lentiform nucleus), hypothalamus, medial temporal lobe, midbrain, and uncus
- Joins the internal cerebral veins posteriorly to contribute to the vein of Galen
5. Great Cerebral Vein of Galen
- A short (~1 cm), midline, unpaired vein formed by the confluence of:
- The two internal cerebral veins
- The two basal veins of Rosenthal
- Other tributaries (e.g., posterior fossa veins)
- Located in the quadrigeminal cistern (superior to the quadrigeminal plate/tectum), posterior to the splenium of the corpus callosum
- Drains deeply located structures: basal ganglia, thalami, hypothalamus, midbrain, choroid plexus, corpus callosum, deep white matter
- Joins the inferior sagittal sinus (coming from the lower border of the falx cerebri) to form the straight sinus (sinus rectus)
6. Downstream: Straight Sinus to Torcular
- Straight sinus (sinus rectus): Formed by vein of Galen + inferior sagittal sinus; runs obliquely in the midline within the junction of the falx cerebri and tentorium cerebelli, toward the confluence of sinuses
- Confluence of sinuses (torcular Herophili): Where the superior sagittal sinus, straight sinus, and occipital sinus converge
- Most blood from the superior sagittal sinus preferentially enters the right transverse sinus
- Most blood from the straight sinus (and vein of Galen) preferentially enters the left transverse sinus
- Transverse sinuses → Sigmoid sinuses → Internal jugular veins
Superficial Deep Cortical Veins (Anastomotic Veins)
These large named superficial veins bridge the two venous territories:
| Vein | Course | Drains Into |
|---|---|---|
| Superior anastomotic vein (of Trolard) | Courses superiorly across the parietal lobe | Superior sagittal sinus |
| Inferior anastomotic vein (of Labbé) | Courses inferiorly over the temporal lobe | Transverse sinus |
| Superficial middle cerebral vein | Runs parallel to the lateral (Sylvian) fissure | Cavernous sinus |
It is uncommon for both Trolard and Labbé to be well developed simultaneously. Thrombosis of the vein of Labbé causes posterolateral temporal lobe infarction.
Posterior Fossa Venous Drainage
The posterior fossa has three principal drainage pathways:
- Vein of Galen (receives superior cerebellar veins, precentral cerebellar vein)
- Superior petrosal sinus
- Direct tributaries into the transverse and straight sinuses
Clinical Correlations
| Deep Vein Thrombosed | Brain Region at Risk | Clinical Presentation |
|---|---|---|
| Internal cerebral vein / Straight sinus | Bilateral thalami + basal ganglia | Altered consciousness, memory loss, bilateral motor deficits |
| Vein of Galen | Deep central structures | Severe coma, bilateral hemispheric signs |
| Vein of Labbé | Posterolateral temporal lobe | Temporal lobe infarct, aphasia, seizures |
| Superior sagittal sinus | Bilateral parasagittal cortex | Leg weakness (bilateral), seizures, raised ICP |
| Thalamostriate vein (neonates) | Thalamus + caudate | Intraventricular hemorrhage |
- Grainger & Allison's Diagnostic Radiology, p. 1454-1455
- Neuroanatomy through Clinical Cases 3rd Ed., p. 10.11
- Gray's Anatomy for Students, p. 1311-1312
Sources: Neuroanatomy through Clinical Cases 3rd Ed. | Gray's Anatomy for Students | Grainger & Allison's Diagnostic Radiology | Color Atlas of Human Anatomy 3
This is a shared conversation. Sign in to Orris to start your own chat.