Explain me ecg 10 common heart disease withchanges ecg and ecg images
Reading File
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram changes heart disease
Finding Sources
Searching Images
atrial fibrillation ECG pattern
Searching Images
heart block ECG first second third degree
Reading File
Searching Images
left ventricular hypertrophy ECG voltage criteria
Searching Images
STEMI anterior myocardial infarction ST elevation ECG
Searching Images
ventricular tachycardia ventricular fibrillation ECG
Searching Images
pericarditis diffuse ST elevation saddle shaped ECG
Searching Images
Wolff-Parkinson-White WPW delta wave ECG short PR
Searching Images
pulmonary embolism right heart strain S1Q3T3 ECG pattern
Searching Images
hyperkalemia peaked T wave wide QRS ECG changes
I now have rich ECG images and data for all 10 conditions. Let me compose the comprehensive guide:
10 Common Heart Diseases: ECG Changes with Images
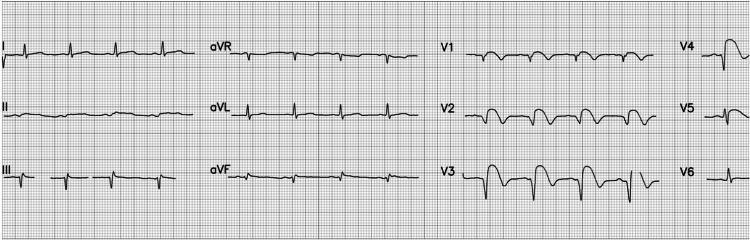
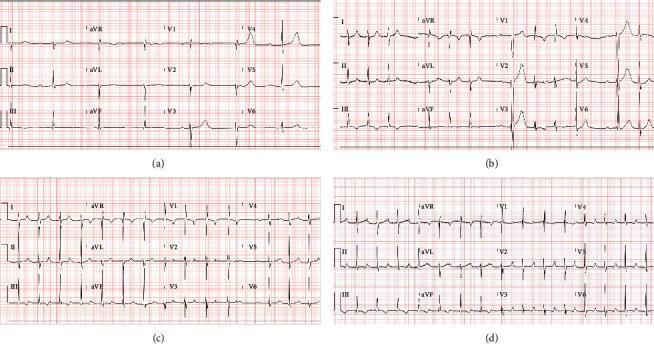
1. 🔴 ST-Elevation Myocardial Infarction (STEMI)
Mechanism: Complete occlusion of a coronary artery → transmural ischemia → injury current
Key ECG Changes:
| Feature | Finding |
|---|---|
| ST segment | Convex ("tombstone") elevation ≥1 mm in ≥2 contiguous leads |
| Reciprocal changes | ST depression in opposite leads |
| Q waves | Pathological Q waves develop (>40 ms wide, >25% of R height) |
| T waves | Hyperacute (tall, peaked) early; later inversion |
| Location | Anterior (V1–V4 = LAD), Inferior (II, III, aVF = RCA), Lateral (I, aVL, V5–V6 = LCx) |
ECG Image – Anterior STEMI (LAD Occlusion):

2. 🟠 Inferior STEMI
Key ECG Changes:
- ST elevation in II, III, aVF (inferior leads)
- Reciprocal ST depression in I and aVL (high lateral)
- ST depression V1–V3 may suggest posterior involvement
- Watch for right ventricular MI (check V3R, V4R)
3. 🟡 Subendocardial Ischemia / NSTEMI
Key ECG Changes:
| Feature | Finding |
|---|---|
| ST depression | Horizontal or downsloping ≥0.5 mm in ≥2 leads |
| T-wave changes | Inversion, biphasic |
| aVR | ST elevation (reciprocal to widespread subendocardial injury) |
| Q waves | Usually absent |
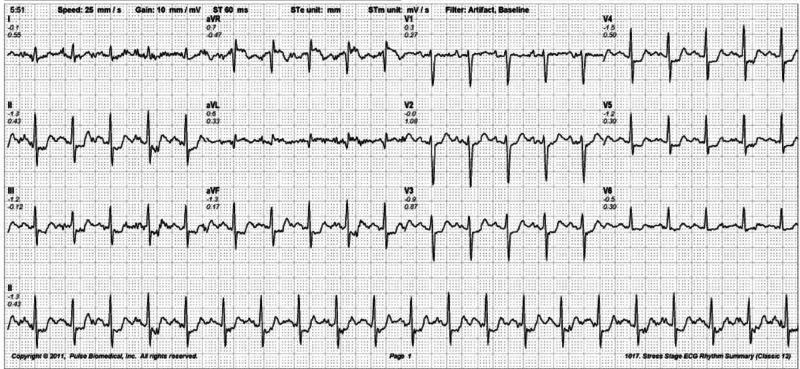
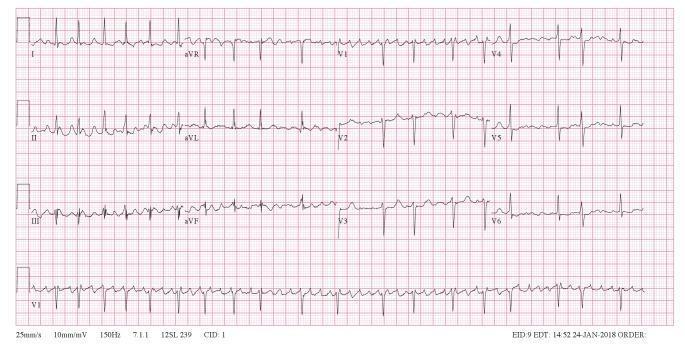
4. 🔵 Atrial Fibrillation (AF)
Key ECG Changes:
| Feature | Finding |
|---|---|
| Rhythm | Irregularly irregular RR intervals |
| P waves | Absent — replaced by fine fibrillatory (f) waves, best seen in V1 |
| Ventricular rate | Variable (controlled <100 bpm; uncontrolled >100 bpm) |
| QRS | Usually narrow unless aberrant conduction |
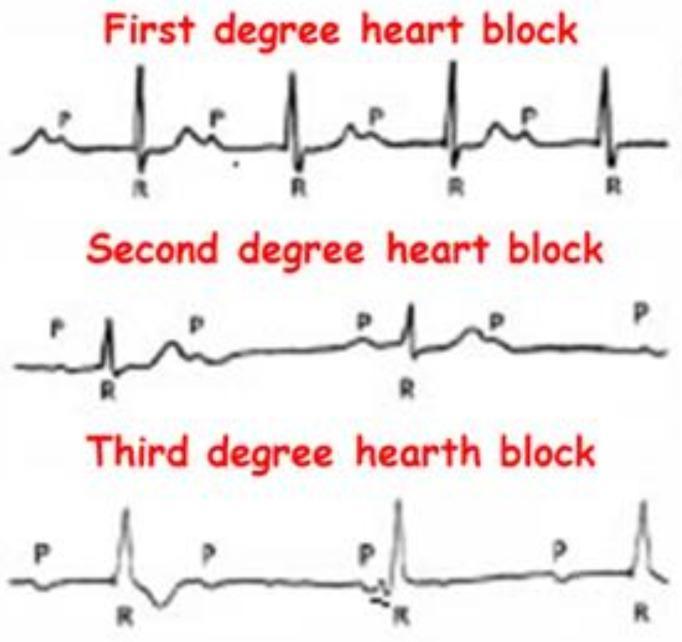
5. 🟣 Heart Block (AV Block)
Three Degrees:
| Degree | ECG Finding |
|---|---|
| 1st degree | PR interval >200 ms, every P conducts |
| 2nd degree Mobitz I | Progressive PR lengthening until a QRS drops (Wenckebach) |
| 2nd degree Mobitz II | Fixed PR, intermittent non-conducted P waves |
| 3rd degree (Complete) | Complete AV dissociation — P and QRS independent, slow escape rhythm |
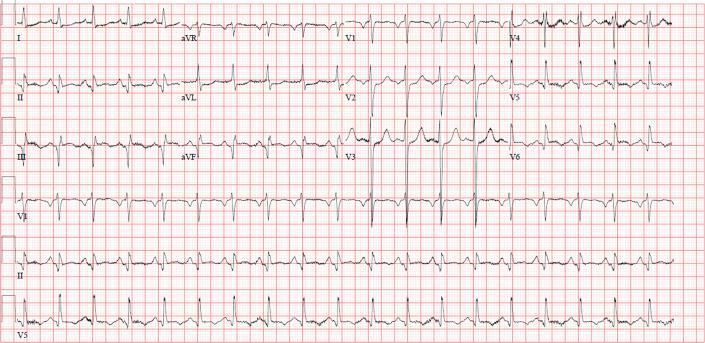
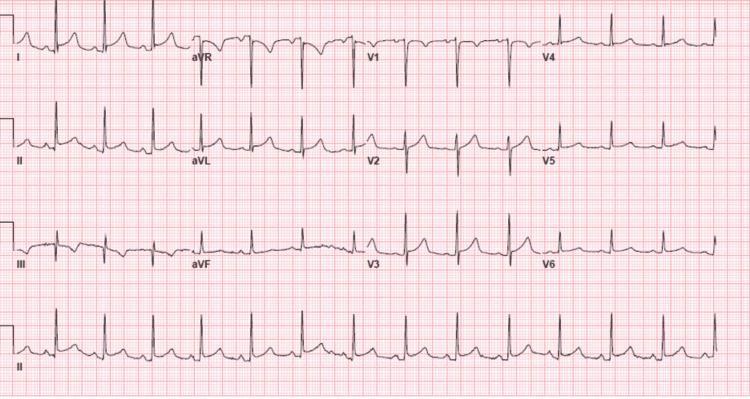
6. 🟤 Left Ventricular Hypertrophy (LVH)
Causes: Hypertension, aortic stenosis, hypertrophic cardiomyopathy
Key ECG Changes:
| Criteria | Threshold |
|---|---|
| Sokolow-Lyon | SV1 + RV5 (or V6) ≥35 mm |
| Cornell voltage | RaVL + SV3 ≥28 mm (men), ≥20 mm (women) |
| Strain pattern | ST depression + T inversion in I, aVL, V5–V6 |
| Left axis deviation | Common |
| P-mitrale | Broad, notched P wave |
7. 🟢 Acute Pericarditis
Mechanism: Inflammation of pericardium → diffuse epicardial injury
Key ECG Changes (4 stages):
| Stage | Timing | Finding |
|---|---|---|
| 1 | Hours–days | Diffuse concave ("saddle-shaped") ST elevation + PR depression |
| 2 | Days | ST normalizes, T-wave flattening |
| 3 | Weeks | T-wave inversions (diffuse) |
| 4 | Months | ECG normalizes |
Distinguishing from STEMI:
- ST elevation is diffuse (not territorial)
- PR depression (most specific sign)
- No reciprocal changes except aVR (ST depression in aVR + PR elevation)
- Spodick's sign: downsloping TP segment

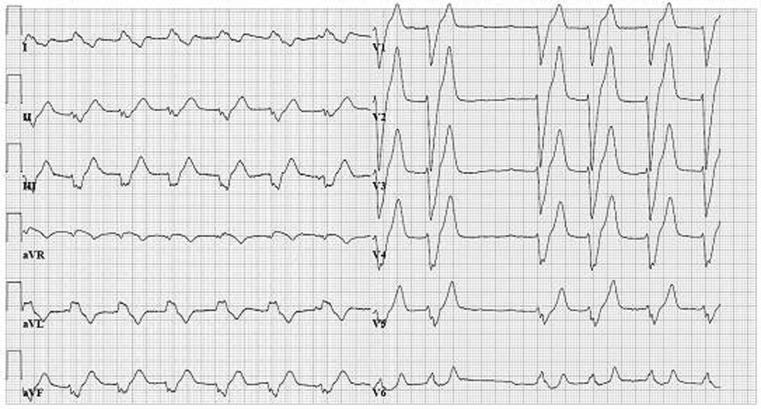
8. ⚡ Wolff-Parkinson-White (WPW) Syndrome
Mechanism: Accessory pathway (Bundle of Kent) bypasses AV node → ventricular pre-excitation
Key ECG Changes (Classic Triad):
| Feature | Finding |
|---|---|
| PR interval | Short (<120 ms) |
| Delta wave | Slurred upstroke at onset of QRS |
| QRS | Widened (>120 ms) due to pre-excitation |
| ST-T changes | Secondary (discordant) repolarization changes |
| Risk | AF with rapid conduction → ventricular fibrillation |


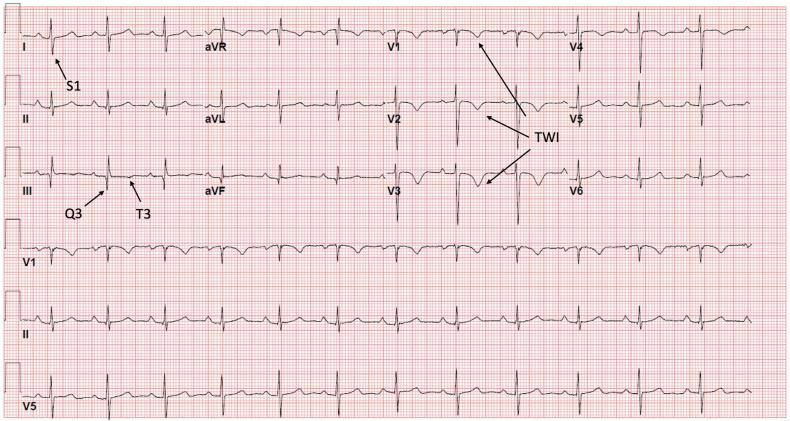
9. 🫁 Pulmonary Embolism (PE)
Mechanism: Acute right heart strain from increased pulmonary vascular resistance
Key ECG Changes:
| Feature | Finding |
|---|---|
| S1Q3T3 | Deep S wave in lead I, Q wave in III, T inversion in III |
| Tachycardia | Sinus tachycardia (most common finding) |
| RBBB | Incomplete or complete right bundle branch block |
| T inversions | V1–V3 or V1–V4 (right ventricular strain) |
| Axis | Right axis deviation |
| P pulmonale | Tall P waves >2.5 mm in II (right atrial enlargement) |

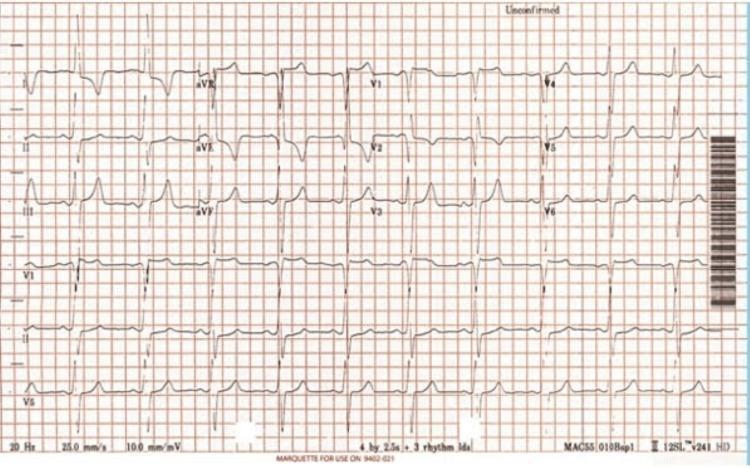
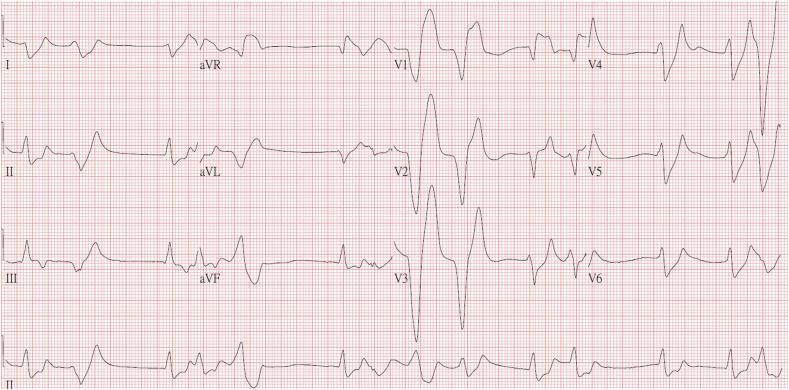
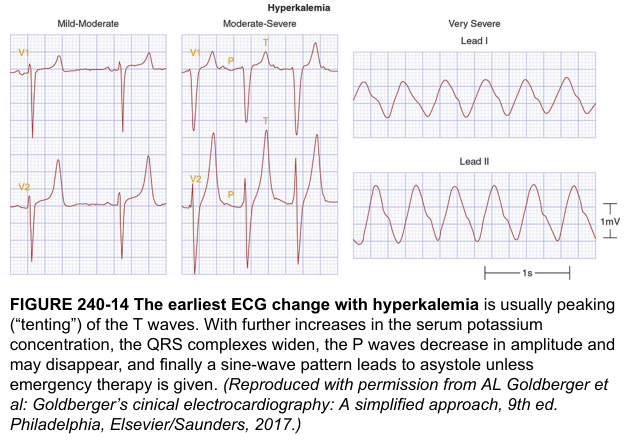
10. 🔋 Hyperkalemia
Mechanism: Elevated K⁺ → altered membrane potential → progressive conduction failure
Progressive ECG Changes by K⁺ Level:
| K⁺ Level | ECG Finding |
|---|---|
| 5.5–6.5 mEq/L | Tall, peaked ("tented") T waves — narrow base, most prominent V2–V4 |
| 6.5–7.5 mEq/L | P wave flattening/disappearance, PR prolongation |
| 7.5–9.0 mEq/L | QRS widening, right axis deviation |
| >9.0 mEq/L | Sine-wave pattern, ventricular fibrillation, asystole |

Quick Reference Summary Table
| Disease | Key ECG Feature | Critical Sign |
|---|---|---|
| Anterior STEMI | ST↑ V1–V4 convex | Tombstone morphology |
| Inferior STEMI | ST↑ II, III, aVF | Reciprocal ↓ I, aVL |
| NSTEMI/Ischemia | ST depression, T inversion | aVR ST↑ = LM/3-vessel |
| Atrial Fibrillation | Irregularly irregular, no P waves | f-waves in V1 |
| Complete Heart Block | AV dissociation | Escape <40 bpm |
| LVH | High voltage (SV1+RV5 ≥35 mm) | Strain pattern I, V5–V6 |
| Pericarditis | Diffuse saddle ST↑ | PR depression |
| WPW | Short PR + delta wave | Pseudo-STEMI risk in AF |
| Pulmonary Embolism | S1Q3T3, sinus tach | T inversion V1–V3 |
| Hyperkalemia | Peaked T waves → sine wave | Wide QRS = emergency |
Sources: Braunwald's Heart Disease (10th ed.) · Harrison's Principles of Internal Medicine (21st ed.) · Rosen's Emergency Medicine — ECG interpretation chapters; clinical ECG image library (PMC/Harrison's).
This is a shared conversation. Sign in to Orris to start your own chat.