Myocarditis
Reading File
Finding Sources
Searching PubMed
myocarditis diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have comprehensive information to deliver a thorough answer. Here is a full clinical overview of myocarditis:
Myocarditis
Definition
Myocarditis is an inflammatory process involving the myocardium, caused by infectious agents, immune-mediated damage, or toxic agents. It must be distinguished from secondary myocardial inflammation resulting from ischemic injury or other structural heart disease.
Epidemiology
Prevalence is estimated at 1 per 100,000 to 1 per 10,000 in population studies, but postmortem studies find myocarditis in up to 12% of young victims of sudden cardiac death. The true incidence is underestimated due to frequent subclinical presentation. It can be the initial clinical manifestation of an arrhythmogenic cardiomyopathy.
- Goldman-Cecil Medicine, p. 511
Etiology
Infectious
| Category | Key Organisms |
|---|---|
| Viral (most common in Western world) | Coxsackievirus A & B (enteroviruses), human herpesvirus 6, parvovirus B19, adenovirus, SARS-CoV-2, HIV, CMV, influenza, hepatitis C |
| Protozoal (most common worldwide) | Trypanosoma cruzi (Chagas disease), Toxoplasma gondii |
| Bacterial | Corynebacterium diphtheriae, Borrelia burgdorferi (Lyme), Mycobacterium, Staphylococcus, Salmonella, meningococcus |
| Spirochetal | Treponema pallidum, Borrelia, Leptospira |
| Fungal | Aspergillus, Candida, Cryptococcus |
| Parasitic | Trichinella spiralis, Echinococcus, Taenia solium |
| Rickettsial | Coxiella burnetii (Q fever), Rickettsia rickettsii |
Immune-Mediated
- Giant cell myocarditis
- Cardiac sarcoidosis
- Systemic lupus erythematosus, systemic sclerosis, dermatomyositis/polymyositis
- Eosinophilic granulomatosis with polyangiitis (EGPA/Churg-Strauss)
- Kawasaki disease
- Drug hypersensitivity (penicillin, sulfonamides, tetracycline, methyldopa)
- Heart transplant rejection
- Immune checkpoint inhibitor therapy
Toxic Causes
- Drugs: anthracyclines, cyclophosphamide, cocaine, amphetamines, trastuzumab, interferon, interleukin-2, clozapine
- Physical agents: electric shock, radiation, hyperpyrexia
- Heavy metals: copper, iron, lead
mRNA COVID-19 Vaccine-Associated
Rare cases occur mainly in male adolescents and young adults, more often after the second dose, typically within a week of vaccination. The excess incidence of myocarditis from SARS-CoV-2 infection itself is approximately 40 extra events per million persons. Most vaccine-associated cases recover uneventfully.
- Goldman-Cecil Medicine, p. 512; Robbins & Kumar Basic Pathology, p. 375
Pathogenesis
Three-phase model (from murine viral myocarditis studies):
- Direct viral invasion - cardiotropic viruses enter cardiomyocytes via receptor-mediated endocytosis; viral genome may cleave dystrophin, impairing sarcolemmal integrity
- Innate immune activation - recruitment of natural killer cells and macrophages; upregulation of pro-inflammatory cytokines (IL-1, TNF); some viruses cause direct cell death
- Adaptive/autoimmune phase - CD4+ T-cell activation promotes B-cell clonal expansion; circulating anti-heart antibodies develop against contractile proteins (myosin), structural proteins, and mitochondrial proteins; cross-reactive T cells attack viral antigens that mimic myocardial proteins; this autoimmune response drives long-term ventricular remodeling and extracellular matrix changes
In Chagas disease, ~10% of patients die during acute myocarditis; survivors may develop progressive CHF and arrhythmia 10-20 years later via chronic immune-mediated cardiomyopathy.
- Goldman-Cecil Medicine, p. 512; Robbins & Kumar Basic Pathology, p. 375
Histopathology (Dallas Criteria)
Four histologic patterns are recognized:
| Pattern | Features |
|---|---|
| Active myocarditis | Myocyte degeneration or necrosis + definite cellular infiltrate ± fibrosis |
| Borderline myocarditis | Definite cellular infiltrate WITHOUT myocardial injury |
| Persistent myocarditis | Continued active myocarditis on repeated biopsy |
| Resolving/resolved | Diminished/absent infiltrate with connective tissue healing |
Viral myocarditis - diffuse lymphocytic infiltrate (most common), interstitial edema, myocyte injury; often patchy (may be missed on biopsy)
Hypersensitivity myocarditis - interstitial and perivascular infiltrates with lymphocytes, macrophages, and a high proportion of eosinophils
Giant cell myocarditis - multinucleated giant cells amid diffuse inflammation; typically fatal without transplant
The Dallas criteria have low sensitivity and specificity (diagnostic yield as low as 10-20%). Molecular techniques (PCR for viral RNA/DNA on biopsy specimens) and immunohistochemical staining for lymphocyte subtypes improve accuracy significantly.
- Robbins & Kumar Basic Pathology, p. 375; Goldman-Cecil Medicine, p. 512
Clinical Manifestations
Presentations span a wide spectrum:
-
Asymptomatic - only transient ECG abnormalities (most common)
-
Prodrome - fever, myalgia, coryzal symptoms, gastroenteritis (viral prodrome)
-
Chest pain - myopericarditis presentation mimicking ACS with angiographically normal coronaries
-
Heart failure - exertional dyspnea, signs of reduced EF; recent-onset dyspnea with hypoxia is the most common symptom
-
Arrhythmias - supraventricular or ventricular tachycardias, AV block (especially Lyme disease, which causes self-limited conduction disease often needing temporary pacing)
-
Fulminant cardiogenic shock - acute cardiovascular collapse
-
Sudden cardiac death - may be first presentation
-
Goldman-Cecil Medicine, p. 512; Braunwald's Heart Disease
Diagnosis
Electrocardiogram
Nonspecific but common findings: sinus tachycardia, ST/T-wave changes, pathologic Q waves, low QRS voltages, supraventricular or ventricular tachyarrhythmias, AV block
Laboratory
- Troponin T and I: may be elevated (but myocarditis can be biopsy-proven even with normal troponins)
- ESR and CRP: usually unhelpful as stand-alone tests
- Autoantibodies against myosin or adenine nucleotide translocator protein: markers of autoimmune myocarditis, correlate with progressive LV dysfunction
- A microRNA (has-miR-Chr8:96) is seen in myocarditis but rarely in MI
- Serologic studies or PCR for viral pathogens
Echocardiography
- Impaired LV (or RV) systolic function with or without dilation
- Regional or global wall motion abnormalities
- LV/RV thrombus
- Diastolic dysfunction
- Pericardial effusion (suggestive of concurrent myopericarditis)
- No single pathognomonic finding
Cardiac MRI (CMR) - Key Non-Invasive Tool
The Lake Louise Criteria (T2-weighted edema + early and late gadolinium enhancement) are the cornerstone of CMR diagnosis:
- T2-weighted STIR: myocardial edema (subepicardial or intramyocardial, frequently lateral/inferior wall)
- Late gadolinium enhancement (LGE): subepicardial pattern - distinguishes myocarditis from MI (which is subendocardial/transmural) and takotsubo (typically absent)
- Early enhancement: demonstrates inflammatory hyperemia even when macroscopic necrosis is absent
- Native T1 mapping: elevated in inflamed regions, superior to T2-STIR for edema detection
- Extracellular volume (ECV): increased in both edema and myocyte necrosis/fibrosis; improves diagnostic accuracy beyond classic Lake Louise criteria
A negative LGE does NOT exclude myocarditis - early enhancement imaging is then critical.
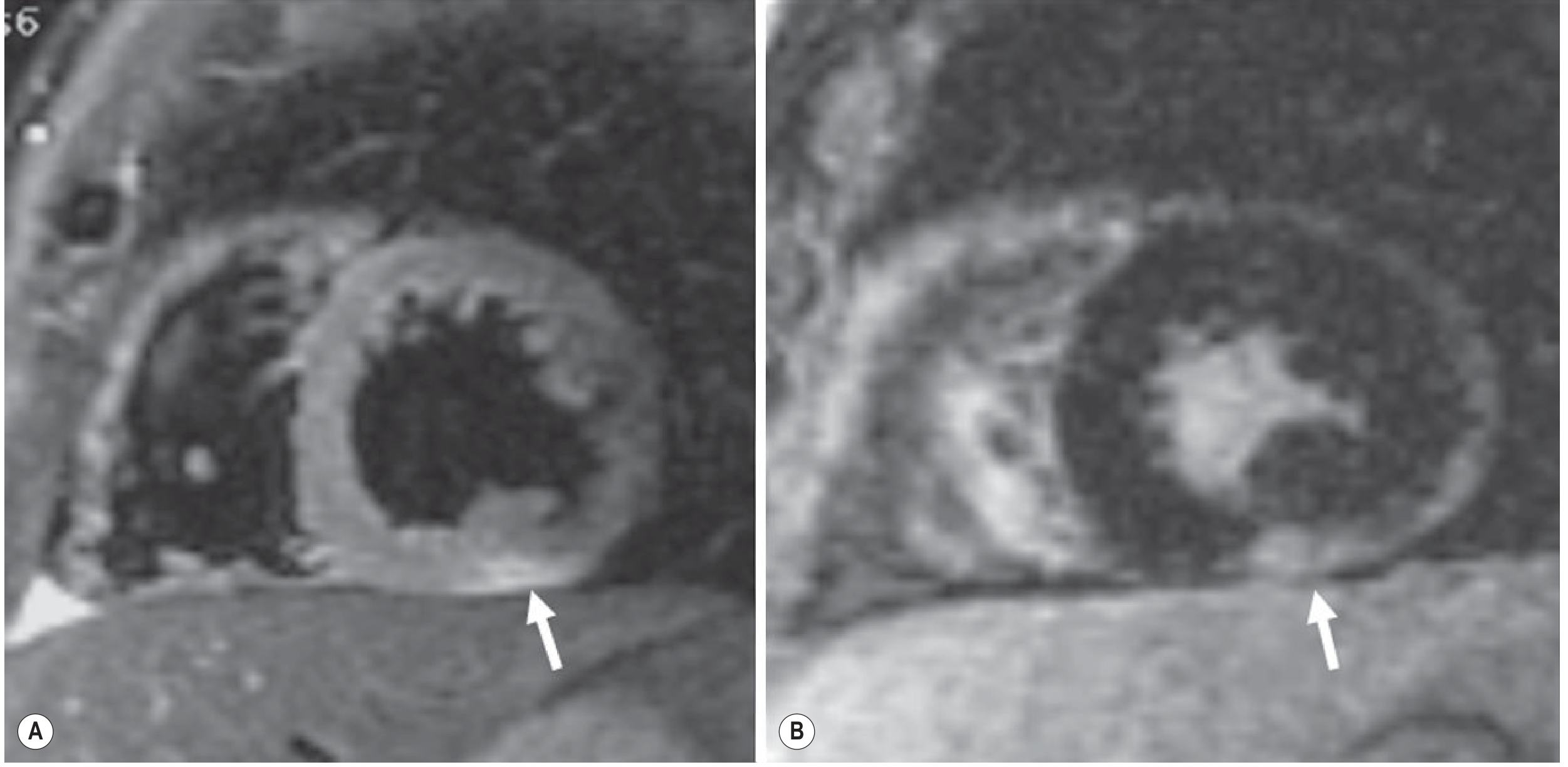
Acute myocarditis on CMR: subepicardial edema and late gadolinium enhancement. - Grainger & Allison's Diagnostic Radiology, p. 331
Endomyocardial Biopsy (EMB) - Gold Standard
- Right ventricular EMB remains the definitive diagnostic test
- US approach: reserved for heart failure refractory to standard therapy, features suggesting systemic disease (sarcoid, amyloid, hemochromatosis, connective tissue disease), or suspected giant cell myocarditis (new HF + tachyarrhythmia/conduction disease)
- European approach: recommended more broadly to achieve etiologic diagnosis and guide treatment in clinically suspected myocarditis
- Histology + PCR + immunohistochemistry together provide the best yield
Management
Supportive (First-Line for All Patients)
- Afterload reduction and diuresis - cornerstone of initial treatment
- Standard HF therapy once stabilized: ACE inhibitors, beta-blockers, diuretics, anticoagulation
- Restrict strenuous exercise during acute phase
Fulminant Myocarditis
- Inotropic support
- Mechanical circulatory support devices
- Extracorporeal membrane oxygenation (ECMO)
- Bridge to cardiac transplantation if refractory
Immunosuppression
- Role remains uncertain for viral lymphocytic myocarditis
- A key RCT (n=111, biopsy-proven myocarditis): prednisolone + cyclosporine or azathioprine showed no difference in mortality or LV function vs. placebo
- Another RCT (MHC expression on biopsy): prednisolone + azathioprine improved LVEF but no difference in mortality or transplant rates at 2 years
- IV immunoglobulin therapy is not helpful
- Immunosuppression IS beneficial for:
- Giant cell myocarditis (often required for survival)
- Eosinophilic myocarditis
- Cardiac sarcoidosis
- Infection-negative immune-mediated forms refractory to conventional HF therapy
Cardiac Transplantation
-
For intractable deteriorating heart failure unresponsive to all measures
-
Goldman-Cecil Medicine, p. 512
Prognosis
| Presentation | Outcome |
|---|---|
| Mild HF / ischemia-like | Typically resolves within weeks, no sequelae |
| Advanced HF (EF < 35%) | May resolve OR progress to dilated cardiomyopathy or death/transplant |
| Fulminant myocarditis | Paradoxically excellent - survival >90% with aggressive support |
| Biopsy-proven viral myocarditis | ~20% long-term mortality at 4.7 years |
| Biventricular dysfunction at presentation | Best predictor of all-cause mortality |
| Giant cell myocarditis | Usually fatal without transplant; stabilized by early immunosuppression |
- Goldman-Cecil Medicine, p. 512
Special Considerations
Chagas Disease (T. cruzi)
The most common infectious myocarditis worldwide. ~300,000 infected individuals in the US. About 10% die in the acute phase; survivors develop chronic dilated cardiomyopathy and arrhythmias 10-20 years later. - Robbins & Kumar Basic Pathology, p. 375
Lyme Myocarditis (B. burgdorferi)
Occurs in ~5% of Lyme disease patients. Manifests primarily as self-limited conduction disease, frequently requiring temporary pacemaker insertion. - Robbins & Kumar Basic Pathology, p. 375
Hypersensitivity Myocarditis
Drug reaction (penicillin, sulfonamides, etc.); typically mild; eosinophilic infiltrate on biopsy; rarely leads to CHF or sudden death unless unrecognized.
Clozapine-Associated Myocarditis
Recognized complication of clozapine (antipsychotic); requires close cardiac monitoring, especially in the first 4 weeks of initiation.
Immune Checkpoint Inhibitor Myocarditis
Rare but increasingly recognized; high mortality; requires immediate cessation of the agent and high-dose corticosteroids.
Sources: Goldman-Cecil Medicine (pp. 511-512), Robbins & Kumar Basic Pathology (p. 375), Grainger & Allison's Diagnostic Radiology (pp. 331-333), Braunwald's Heart Disease
Can you give the treatment with dosage
Finding Sources
Searching PubMed
myocarditis treatment immunosuppression dosage
Finding Sources
Finding Sources
Searching the Web
myocarditis treatment protocol dosage 2024 guidelines ACE inhibitor beta blocker immunosuppression
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC11076022
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Now I have all the key dosage information. Let me compile the comprehensive treatment with dosages.
Myocarditis - Treatment with Dosages
1. General Measures (All Patients)
- Physical activity restriction for 3-6 months from symptom onset - reduces mechanical stress on the inflamed myocardium
- Avoid competitive sports until inflammation has resolved (normal troponin, ECG, LVEF, and CMR)
- Treat any underlying precipitant (stop offending drug, treat infection)
2. Supportive Heart Failure Therapy (First-Line)
Initiated when LVEF is reduced, following guideline-directed medical therapy (GDMT):
ACE Inhibitors / ARBs
| Drug | Starting Dose | Target Dose |
|---|---|---|
| Enalapril | 2.5 mg twice daily | 10-20 mg twice daily |
| Lisinopril | 2.5-5 mg once daily | 20-40 mg once daily |
| Ramipril | 1.25-2.5 mg once daily | 5 mg twice daily |
| Sacubitril/Valsartan (ARNI) | 24/26 mg twice daily | 97/103 mg twice daily (preferred over ACEi where tolerated) |
Beta-Blockers (titrate slowly; do NOT initiate in decompensated/wet HF)
| Drug | Starting Dose | Target Dose |
|---|---|---|
| Carvedilol | 3.125 mg twice daily | 25-50 mg twice daily |
| Metoprolol succinate (XL) | 12.5-25 mg once daily | 200 mg once daily |
| Bisoprolol | 1.25 mg once daily | 10 mg once daily |
Titrate every 2 weeks in stable patients. Avoid in acute decompensation.
Mineralocorticoid Receptor Antagonists (MRA)
| Drug | Dose |
|---|---|
| Spironolactone | 25-50 mg once daily |
| Eplerenone | 25-50 mg once daily |
SGLT2 Inhibitors (added per 2021+ ESC HF guidelines)
| Drug | Dose |
|---|---|
| Dapagliflozin | 10 mg once daily |
| Empagliflozin | 10 mg once daily |
Diuretics (for congestion relief)
| Drug | Dose |
|---|---|
| Furosemide | 20-40 mg IV/orally; titrate to symptoms and fluid status |
| Torsemide | 10-20 mg once daily orally |
Important: Patients whose LVEF recovers to >40% after myocarditis should continue HF therapy. Premature discontinuation risks relapse of LV dysfunction.
3. Acute/Fulminant Myocarditis - Hemodynamic Support
| Therapy | Details |
|---|---|
| Dobutamine | 2-20 mcg/kg/min IV infusion (use cautiously - highly arrhythmogenic) |
| Milrinone | 0.375-0.75 mcg/kg/min IV infusion (less chronotropic than dobutamine) |
| IABP (intra-aortic balloon pump) | Mechanical hemodynamic support |
| LVAD / ECMO | For refractory cardiogenic shock; bridge to recovery or transplant |
4. Myopericarditis (Chest Pain Dominant Presentation)
When pericardial inflammation coexists (myopericarditis) with preserved LV function:
| Drug | Dose | Duration |
|---|---|---|
| Ibuprofen | 300-600 mg three times daily | Until symptom-free, then taper |
| Colchicine | 0.5 mg twice daily (>70 kg) or 0.5 mg once daily (<70 kg); reduce to once daily after 3-6 months | 3-6 months |
| NSAIDs are avoided if LV dysfunction is present (worsen outcomes in HF) |
- Goldman-Cecil Medicine (pericarditis section, p. 480)
5. Immunosuppressive Therapy
When to Use
Immunosuppression is NOT recommended for routine viral lymphocytic myocarditis. It is recommended for:
- EMB-proven, virus-negative, autoimmune/inflammatory forms
- Giant cell myocarditis
- Eosinophilic myocarditis
- Cardiac sarcoidosis
- Myocarditis from systemic autoimmune disease (SLE, polymyositis, EGPA)
- Lymphocytic myocarditis refractory to conventional HF therapy
- Duration typically at least 6-12 months, tailored to disease activity on serial biopsy/CMR
Corticosteroids
| Indication | Drug | Dose |
|---|---|---|
| Autoimmune/virus-negative myocarditis | Prednisolone | 1 mg/kg/day (induction), taper to 0.2 mg/kg/day maintenance over 3 months total (90-day course) |
| Giant cell myocarditis | Prednisone or Methylprednisolone | High-dose; start 1 mg/kg/day prednisone or IV methylprednisolone pulse initially |
| Fulminant myocarditis with immune etiology suspected | IV Methylprednisolone | 500-1000 mg/day for 3 days, then switch to oral |
| ICI-associated myocarditis (see below) | IV Methylprednisolone | 1000 mg/day initially |
Azathioprine (combined with steroids)
| Drug | Dose |
|---|---|
| Azathioprine | 1-2 mg/kg/day orally (typically 50-150 mg/day depending on weight) |
Used in combination with prednisone in the Myocarditis Treatment Trial and TIMIC trial. Duration at least 6-12 months in autoimmune forms.
Cyclosporine
| Drug | Dose |
|---|---|
| Cyclosporine | 1-2 mg/kg/day orally (adjust to trough levels 100-200 ng/mL) |
Alternative to azathioprine as combination immunosuppression with steroids.
Mycophenolate Mofetil
- 500-1500 mg twice daily (alternative antimetabolite in steroid-refractory cases)
6. Immune Checkpoint Inhibitor (ICI)-Associated Myocarditis
This is a medical emergency with high mortality (~40-50% in severe cases).
| Step | Drug | Dose |
|---|---|---|
| 1. Stop ICI immediately | - | Permanently discontinue ICI |
| 2. High-dose IV corticosteroids | Methylprednisolone IV | 1000 mg/day for 3-5 days |
| 3. Transition to oral | Prednisone oral | 1 mg/kg/day, taper slowly based on troponin/LVEF/ECG normalization |
| 4. Steroid-refractory cases | Anti-thymocyte globulin (ATG) | Specialist dosing |
| Mycophenolate mofetil | 500-1500 mg twice daily | |
| Abatacept | 500-750 mg IV (weight-based) | |
| Infliximab | Avoid in HF (can worsen cardiac function) |
Continue corticosteroids until: resolution of symptoms + troponin normalization + LVEF recovery + conduction abnormalities resolved.
- Braunwald's Heart Disease, p. 2418
7. Giant Cell Myocarditis
Requires aggressive multi-drug immunosuppression immediately upon diagnosis:
| Regimen | Drugs |
|---|---|
| Standard | Prednisone + cyclosporine (most evidence) |
| Alternative | Prednisone + azathioprine |
| Aggressive | Prednisone + cyclosporine + azathioprine |
| Cytolytic | Anti-thymocyte globulin (ATGAM or Thymoglobulin) |
Typical combination: Prednisone 1 mg/kg/day + Cyclosporine targeting trough 150-250 ng/mL + Azathioprine 1-2 mg/kg/day. Most patients require cardiac transplantation if refractory.
- Fuster and Hurst's The Heart, Table 46-5
8. Eosinophilic Myocarditis
- Stop the causative drug/allergen
- Prednisone 1 mg/kg/day - usually responds well to high-dose steroids
- Taper over several months once EF recovers and eosinophil count normalizes
9. Cardiac Sarcoidosis
| Drug | Dose |
|---|---|
| Prednisone (first-line) | 40-60 mg/day initially, taper over 6-12 months to a maintenance dose of 10-20 mg/day (or lowest effective dose) |
| Methotrexate or Azathioprine | Added as steroid-sparing agents when long-term therapy is needed |
10. Arrhythmia Management
- Complete heart block / high-grade AV block: temporary pacing - especially common in Lyme disease and sarcoidosis; often self-resolving in Lyme
- Ventricular tachycardia: amiodarone (150 mg IV bolus, then 1 mg/min x 6 h, then 0.5 mg/min) or lidocaine; cardioversion if hemodynamically unstable
- Implantable cardioverter-defibrillator (ICD): defer until inflammation resolved; consider if persistent LV dysfunction after 3-6 months of optimal therapy
Summary Table
| Situation | Key Drugs | Key Doses |
|---|---|---|
| HF with reduced EF | ACEi/ARNI + BB + MRA + SGLT2i | Standard GDMT doses (above) |
| Congestion | Furosemide | 20-80 mg IV/oral |
| Myopericarditis | Ibuprofen + colchicine | 600 mg TDS + 0.5 mg BD |
| ICI myocarditis | Methylprednisolone IV | 1000 mg/day x 3-5 days |
| Giant cell myocarditis | Pred + cyclosporine ± azathioprine | 1 mg/kg/day + trough 150-250 ng/mL |
| Eosinophilic myocarditis | Prednisone | 1 mg/kg/day, taper |
| Cardiac sarcoidosis | Prednisone | 40-60 mg/day, taper to 10-20 mg |
| Virus-negative autoimmune | Prednisone + azathioprine | 1 mg/kg/day + 1-2 mg/kg/day x 6-12 months |
| Fulminant cardiogenic shock | Dobutamine/milrinone ± ECMO | 2-20 mcg/kg/min |
Key principle: Immunosuppression should only be started after ruling out active viral infection on EMB (PCR negative for cardiotropic viruses), except in life-threatening cases (giant cell, ICI-myocarditis, eosinophilic) where early empirical treatment is justified.
Sources: Braunwald's Heart Disease (p. 2418), Fuster & Hurst's The Heart (Table 46-5, p. 1001), Goldman-Cecil Medicine (p. 512), ESC Heart Failure Guidelines 2021/2023, PMC review of myocarditis management
This is a shared conversation. Sign in to Orris to start your own chat.