Tell me everything regarding cataract in reference of ophthalmology
Reading File
Finding Sources
Searching PubMed
"cataract"[MeSH Terms] AND "phacoemulsification"[MeSH Terms]
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed. Let me compile the comprehensive, well-structured answer.
Cataract - A Complete Ophthalmological Review
Based primarily on Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
1. Definition and Epidemiology
A cataract is any opacity of the crystalline lens of the eye. It is the commonest cause of reversible visual disability in the world. There is no medical treatment to prevent the development or progression of cataract. Phacoemulsification with intraocular lens (IOL) implantation is the gold standard surgical treatment and is the most commonly performed surgical procedure worldwide.
2. Anatomy of the Lens
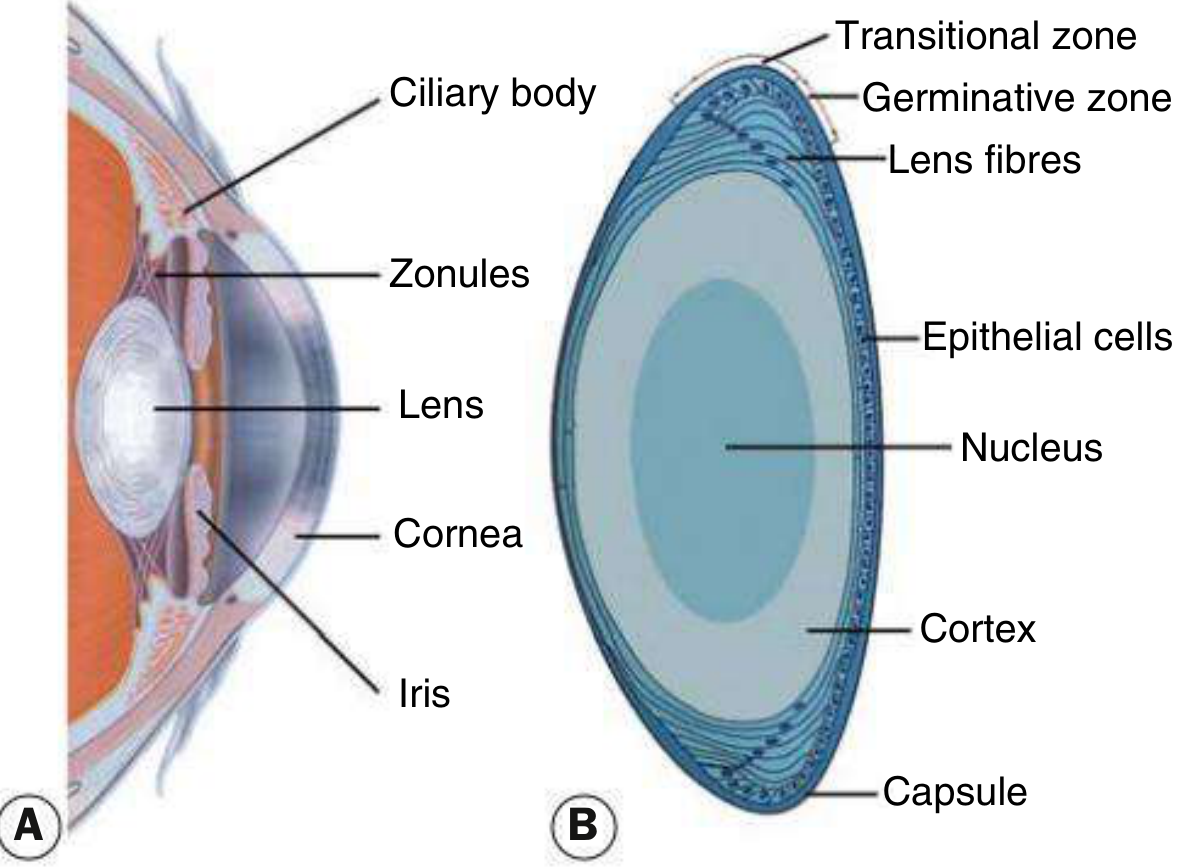
Fig. 10.1 - Kanski's Clinical Ophthalmology, 10th Ed.
- Zonules hold the lens in position, suspending it from the ciliary body.
- Capsule - an acellular membrane enclosing the lens material.
- Lens epithelium - cuboid cells beneath the anterior capsule extending to the equator; cells in the germinative zone divide continuously and differentiate into lens fibers.
- Lens substance - central nucleus surrounded by cortical material.
3. Symptoms of Cataract
Cataracts often develop slowly; early changes may be subtle. Symptoms include:
| Symptom | Mechanism |
|---|---|
| Reduced visual acuity | Progressive opacification |
| Loss of contrast sensitivity | Scatter of incoming light |
| Change in colour perception (blue hues) | Urochrome pigment deposition (nuclear) |
| Glare / night driving difficulty | Light scattering |
| Monocular diplopia | Irregular refraction through opacities |
| Difficulty in low-light situations | Reduced light transmission |
| "Second sight" (temporary improvement in near vision) | Myopic shift from increased nuclear refractive index |
4. Classification of Cataract
4A. Age-Related (Acquired) Cataract
The most common type. Classified by morphology and location:
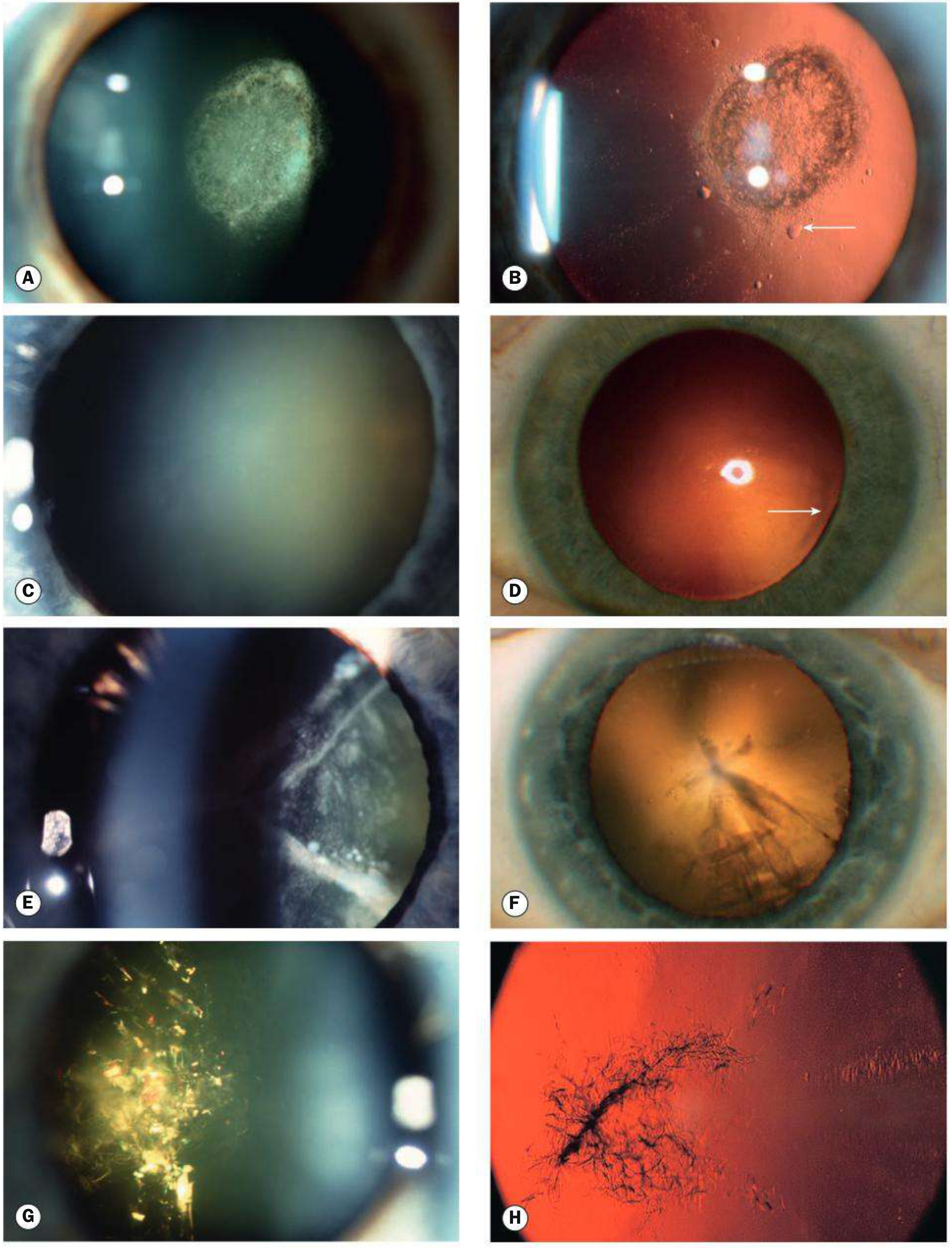
Fig. 10.2 - Kanski's Clinical Ophthalmology, 10th Ed.
i. Posterior Subcapsular (PSC) Cataract
- Located just in front of the posterior capsule
- Granular or plaque-like on oblique slit-lamp biomicroscopy
- Appears black and vacuolated on retroillumination; vacuoles are swollen migratory lens epithelial cells (bladder/Wedl cells)
- Due to location at the nodal point, has a particularly profound impact on vision even when small
- Characteristic symptoms: glare (especially from oncoming car headlights), worse in bright light (miosis) and on near tasks
- Associated with: corticosteroid use, diabetes, irradiation, uveitis
ii. Nuclear Sclerotic Cataract
- Exaggeration of the normal ageing change of the lens nucleus
- Associated with myopia due to increased refractive index - this can cause "second sight of the aged" where presbyopic patients can temporarily read without spectacles
- Characterized by a yellowish hue due to urochrome pigment deposition
- Best assessed with oblique slit-lamp beam
- Retroillumination shows good red reflex but a subtle distinction between nucleus and cortex
- In advanced stages: nucleus appears brown (brunescent) or in rare cases black (nigricans)
iii. Cortical Cataract
- May involve the anterior, posterior or equatorial cortex
- Starts as clefts and vacuoles between lens fibres due to cortical hydration
- Subsequent opacification forms cuneiform (wedge-shaped) or radial spoke-like opacities
- Often found initially in the inferonasal quadrant
- Glare is a prominent symptom
iv. Christmas Tree Cataract
- Uncommon; polychromatic needle-like formations in the deep cortex and nucleus
- Has a distinctive glittering multicolored appearance on slit-lamp examination
4B. Maturity Stages of Cataract
| Stage | Description |
|---|---|
| Immature | Partially opaque; fundal red reflex present |
| Mature | Totally opaque; no red reflex; white/milky in appearance |
| Hypermature | Liquefied cortex; lens shrinks; wrinkled capsule |
| Morgagnian | Nucleus sinks to bottom of liquefied cortex |
4C. Secondary (Complicated) Cataract
Develops as a result of other primary ocular diseases:
- Chronic anterior uveitis - the most common cause of secondary cataract. Incidence related to duration/intensity of inflammation. Earliest sign: polychromatic lustre at posterior pole. Progresses to posterior and anterior opacities. Topical/systemic steroids used in treatment are also causative.
- Acute congestive angle closure - causes small anterior grey-white subcapsular opacities called glaukomflecken - focal infarcts of lens epithelium; pathognomonic of previous acute angle closure
- High (pathological) myopia - posterior subcapsular opacity and early-onset nuclear sclerosis
- Hereditary fundus dystrophies - retinitis pigmentosa, Leber congenital amaurosis, gyrate atrophy, Stickler syndrome - usually posterior subcapsular opacity
- Secondary to medication - systemic and topical steroids cause posterior subcapsular cataracts
- Radiation, vitreoretinal surgery (silicone oil, gas tamponade), trauma
4D. Cataract in Systemic Disease
| Disease | Cataract Characteristics |
|---|---|
| Diabetes mellitus | "Snowflake" cataract (bilateral, acute in young diabetics); accelerated nuclear sclerosis in older patients |
| Myotonic dystrophy | "Christmas tree" cataract with polychromatic crystals; PSC also seen |
| Down syndrome (Trisomy 21) | Sutural/flake/zonular opacities |
| Neurofibromatosis type 2 | PSC or capsular opacities |
| Wilson disease | "Sunflower" cataract - characteristic petal-like deposition of copper in anterior lens capsule |
| Atopic dermatitis | Anterior subcapsular cataracts (bilateral) |
| Hypocalcaemia | Small white iridescent cortical opacities |
| Galactosaemia | Oil-droplet cataract in infants |
4E. Traumatic Cataract
- Blunt trauma - contrecoup forces cause lens fibre disruption; may cause rosette-shaped opacity at the posterior pole; stellate opacity at the anterior pole
- Perforating injury - lens rapidly opacifies (may swell, causing secondary glaucoma)
- Radiation - X-rays, neutrons, and infrared rays can cause posterior subcapsular cataract (glassblowers' cataract from chronic infrared exposure)
- Electrical - anterior subcapsular opacities following electric shock or lightning strike
- Chemical - acids/alkalis affecting the lens secondarily after corneal/anterior segment involvement
4F. Congenital Cataract
Aetiology
Metabolic disorders:
- Galactosaemia - oil-droplet opacity; responds to early dietary galactose restriction
- Galactokinase deficiency - nuclear cataract
- Hypocalcaemia (hypoparathyroidism)
- Lowe (oculocerebrorenal) syndrome - dense cataract; X-linked recessive
Intrauterine infections (TORCH):
- Rubella - bilateral dense nuclear cataracts; often associated with other features (cardiac defects, deafness)
- Toxoplasmosis, CMV, varicella (less common)
Other systemic associations:
- Down syndrome, Turner syndrome, Patau syndrome (Trisomy 13)
- Nance-Horan syndrome (X-linked)
- Norrie disease
Isolated hereditary:
- Autosomal dominant is the most common form of isolated hereditary cataract
Management of Congenital Cataract
- Dense unilateral cataracts require surgery within the first few weeks of life to prevent permanent amblyopia
- Dense bilateral cataracts - surgery within the first 6-10 weeks
- Post-operatively, optical correction (contact lenses or spectacles) and amblyopia treatment (patching the fellow eye) are essential
- Primary posterior capsulotomy and anterior vitrectomy are often performed in young children to prevent posterior capsular opacification
5. Management of Acquired Cataract
5A. Indications for Surgery
- Functional - visual acuity reduced to a level that affects the patient's daily activities (most common indication)
- Medical - lens-induced glaucoma (phacomorphic, phacolytic), lens-induced uveitis, obstruction to view of the posterior segment (e.g., in diabetic retinopathy management)
- Optical - to correct high refractive error (e.g., unilateral aphakia, refractive lens exchange)
5B. Preoperative Assessment
- Visual acuity - best corrected Snellen or LogMAR chart
- Biometry - measurement of axial length (A-scan ultrasound or optical coherence biometry) and corneal curvature (keratometry) to calculate IOL power
- Barrett Universal II, Holladay, SRK/T, Haigis formulas commonly used
- Margin of error: postoperative unaided refraction is within 1.0 D of predicted in ~90% and within 0.5 D in two-thirds of patients
- Corneal assessment - pre-existing endothelial disease warrants caution
- Fundal assessment - particularly if posterior pathology may limit visual recovery
- Pupil dilation - adequacy for surgery
- General health - anticoagulation management, diabetes, fitness for anaesthesia
Refractive Planning
- Emmetropia is typically the desired postoperative refraction
- Many surgeons aim for a small degree of myopia (~-0.25 D) to offset biometry errors
- Monovision - non-dominant eye targeted at ~1-2 D of myopia for near work; dominant eye targeted for emmetropia
- Multifocal IOLs - achieve near, intermediate, and distance vision but can cause glare and loss of contrast sensitivity
- Contralateral eye consideration - target should be within <2.0 D of the fellow eye to avoid anisometropia
5C. Intraocular Lenses (IOLs)
Anatomy of an IOL
- Optic - central refracting element
- Haptics - arms/loops that stabilize the optic by contacting peripheral ocular structures
Positioning
| Location | Indication |
|---|---|
| "In the bag" (capsular bag) | Ideal; standard uncomplicated surgery |
| Ciliary sulcus | After posterior capsule rupture (three-piece IOL only) |
| Anterior chamber (AC) | Insufficient posterior capsule support; specific AC IOL required |
| Iris-fixated / scleral-fixated | No capsular support |
IOL Types
- Monofocal - single focal point; patient needs reading glasses for near
- Toric IOL - corrects pre-existing corneal astigmatism
- Multifocal IOL (diffractive/refractive) - near + distance; risk of glare/haloes
- Extended depth of focus (EDOF) - intermediate and distance; reduced photic phenomena
- Accommodating IOL - attempts to mimic natural accommodation (limited effectiveness)
- Phakic IOL - placed in front of the natural lens (clear lens) for refractive correction
IOL Materials
- Modern IOLs are flexible (foldable) - introduced through a small incision via an injector
- Materials: hydrophobic acrylic (most common), hydrophilic acrylic, silicone, PMMA (rarely used now)
- Hydrophobic acrylic is associated with less posterior capsular opacification (PCO)
5D. Anaesthesia Options
| Type | Details |
|---|---|
| Topical | Proxymetacaine or oxybuprocaine drops; most common for routine phacoemulsification; patient cooperative required |
| Sub-Tenon | Cannula placed in sub-Tenon space; good akinesia + analgesia; minimal risk |
| Peribulbar | Injection outside muscle cone; widespread use; risk of globe perforation (rare) |
| Retrobulbar | Injection inside muscle cone; complete akinesia; higher risk (globe perforation, optic nerve damage) |
| General anaesthesia | Children, uncooperative patients, complex cases |
5E. Phacoemulsification - The Gold Standard Procedure
Phacoemulsification uses ultrasonic energy to emulsify the lens nucleus, which is then aspirated. Performed through a small self-sealing incision (~2.2-2.8 mm).
Key Surgical Steps:
- Corneal incision - usually temporal clear corneal incision; paracentesis for second instrument
- Viscoelastic injection - maintains anterior chamber depth; protects corneal endothelium
- Capsulorhexis - circular continuous tear of the anterior capsule (~5.5 mm diameter)
- Hydrodissection - fluid separates the capsule from the lens cortex
- Phacoemulsification - nucleus is sculpted and chopped using ultrasonic probe; "divide and conquer" or "stop and chop" technique
- Irrigation and aspiration (I&A) - removal of residual cortex
- IOL implantation - folded IOL injected into the capsular bag
- Viscoelastic removal - prevents post-operative IOP spike
Surgical Parameters
- Ultrasound energy - minimized to reduce corneal endothelial damage; phaco time and cumulative dissipated energy (CDE) are key metrics
- Fluidics - balanced salt solution (BSS); appropriate infusion pressure and aspiration flow rate
5F. Manual (Extracapsular) Cataract Surgery (ECCE / MSICS)
- Used when phacoemulsification is not available or nucleus is too hard for phaco
- ECCE: large limbal incision (~10-12 mm); nucleus expressed manually; IOL implanted; sutured
- Manual Small Incision Cataract Surgery (MSICS): Modified technique; nucleus expressed through a small tunnel incision without sutures; popular in developing world settings for high volume surgery
5G. Femtosecond Laser-Assisted Cataract Surgery (FLACS)
- Laser performs capsulorhexis, corneal incisions, and lens fragmentation
- Benefits: potentially more precise capsulorhexis, reduced phaco energy
- A 2025 meta-analysis (PMID: 40731148) found no clinically significant difference in visual outcomes compared to conventional phacoemulsification in RCTs
6. Postoperative Complications
Early Complications
| Complication | Notes |
|---|---|
| Posterior capsule rupture (intraoperative) | ~2-4%; most common intraoperative complication; risk of vitreous loss |
| Vitreous loss | Requires anterior vitrectomy; higher risk of endophthalmitis and RD |
| Zonular dehiscence | Associated with pseudoexfoliation, Marfan syndrome, trauma |
| Suprachoroidal haemorrhage | Extremely rare (0.04%) with phaco; bleed from posterior ciliary artery; potentially catastrophic; requires immediate wound closure |
| Corneal oedema / Descemet's folds | Often transient; persistent if endothelial disease or high phaco energy used |
| IOP spike | Retained viscoelastic; treated with IOP-lowering agents |
Postoperative Endophthalmitis
- Incidence: ~0.1% after cataract surgery
- Most (90%) caused by Gram-positive organisms; Staphylococcus epidermidis most common
- Risk factors: posterior capsule rupture, wound leak, temporal clear corneal incision, adnexal disease, diabetes
- Prophylaxis: intracameral cefuroxime (preferred in Europe) or moxifloxacin at end of surgery; povidone-iodine prep is essential
- Treatment: based on EVSG study results - intravitreal vancomycin + amikacin/ceftazidime; pars plana vitrectomy if light perception only
Posterior Capsule Opacification (PCO)
- Most common long-term complication; occurs in 10-50% within 2-5 years
- Due to proliferation and migration of residual lens epithelial cells (Elschnig pearls)
- Causes visual symptoms similar to the original cataract
- Treatment: Nd:YAG laser posterior capsulotomy - safe, effective outpatient procedure
- Prevention: sharp-edged IOL design (barrier effect), hydrophobic acrylic material, in-the-bag IOL placement
Dysphotopsia
- Positive dysphotopsia - unwanted light perceptions (arcs, streaks, starbursts, haloes) due to internal reflection within the IOL; more common with hydrophobic acrylic
- Negative dysphotopsia - a temporal crescent or shadow; believed to be due to a gap between the IOL and the capsule; resolves spontaneously in most cases
- Management: reassurance; brimonidine for positive; pupil dilation for negative; sulcus IOL repositioning for refractory cases
Other Long-Term Complications
| Complication | Details |
|---|---|
| Refractive surprise | Under/over-correction; risk reduced by preoperative biometry quality check |
| Corneal decompensation | Pseudophakic bullous keratopathy; at-risk: pre-existing low endothelial count |
| Retinal detachment | Rhegmatogenous; uncommon after uncomplicated phaco; risk higher with high myopia, vitreous loss |
| Ptosis | Often mild; topical steroid related; usually resolves; defer lid surgery ≥1 year |
| IOL malposition | Decentration, sunset/sunrise syndrome; may require repositioning or exchange |
| Macular oedema (Irvine-Gass) | Cystoid macular oedema; managed with topical NSAIDs ± steroids |
7. Cataract in Special Situations
High-Risk Eyes
- Pseudoexfoliation syndrome - zonular weakness; risk of zonular dehiscence during surgery; requires iris hooks/Malyugin ring and capsular tension ring (CTR)
- Small pupils - intraoperative floppy iris syndrome (IFIS) associated with tamsulosin; requires iris expansion devices
- High myopia - larger axial length makes biometry less accurate; higher RD risk post-surgery
- Dense mature cataracts - no red reflex; trypan blue used to stain anterior capsule for capsulorhexis visualization
- Corneal pathology - Fuchs endothelial dystrophy; may need combined phaco-DSAEK/DMEK
Paediatric Cataract - Key Points
- Risk of amblyopia is the primary concern
- Dense unilateral cataracts need surgery within 6-8 weeks of birth
- Primary posterior capsulotomy + anterior vitrectomy done at time of surgery
- Contact lens or spectacle correction immediately post-op
- Patching of the fellow eye for amblyopia therapy
- Secondary IOL implantation typically deferred until ~2 years of age
8. Ectopia Lentis (Lens Dislocation)
Though a distinct entity, closely related to lens pathology:
| Condition | Inheritance | Direction of Dislocation |
|---|---|---|
| Marfan syndrome | AD (FBN1) | Superotemporal |
| Homocystinuria | AR (CBS) | Inferonasal |
| Weill-Marchesani syndrome | AR or AD | Inferonasal/any |
| Isolated familial ectopia lentis | AD | Usually superotemporal |
| Trauma | - | Any direction |
9. Abnormalities of Lens Shape (Associated with Cataract)
- Anterior lenticonus - conical protrusion of anterior lens surface; associated with Alport syndrome (X-linked); progressive - may need surgery
- Posterior lenticonus - more common than anterior; usually unilateral sporadic; progressive opacity often results; "oil droplet" sign on retroillumination
- Lentiglobus - rare unilateral generalized hemispherical deformity
- Microspherophakia - small spherical lens; associated with Marfan, Weill-Marchesani, congenital rubella; complications include lenticular myopia, subluxation
- Lens coloboma - congenital indentation of the peripheral lens from localized zonular deficiency; not a true coloboma
10. Recent Evidence (PubMed, 2024-2026)
- A 2025 meta-analysis of RCTs (PMID: 40731148, Lee SH et al., Sci Rep) comparing femtosecond laser-assisted cataract surgery (FLACS) to conventional phacoemulsification found no clinically significant difference in visual outcomes, suggesting conventional phaco remains the gold standard.
- Combined microinvasive glaucoma surgery (MIGS) with phacoemulsification in open-angle glaucoma shows modest but significant IOP reduction over phaco alone (PMID: 39089358, Yuan PHS et al., Am J Ophthalmol 2025).
Summary
| Feature | Key Point |
|---|---|
| Definition | Lens opacity; #1 cause of reversible blindness worldwide |
| Types | Nuclear sclerotic, posterior subcapsular, cortical, Christmas tree |
| Commonest systemic cause | Diabetes (snowflake/accelerated nuclear) |
| Commonest secondary cause | Chronic anterior uveitis |
| Most visually devastating | Posterior subcapsular (nodal point location) |
| Treatment | Phacoemulsification + IOL implantation |
| Most common complication | Posterior capsule opacification |
| PCO treatment | Nd:YAG laser capsulotomy |
| Commonest endophthalmitis organism | S. epidermidis |
| Congenital - most urgent | Dense unilateral cataract (surgery within 6-8 weeks) |
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition (ISBN 9780443110993)
What is VKC in opthal
Reading File
Finding Sources
Searching PubMed
"vernal keratoconjunctivitis"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I have all the content needed for a thorough answer. Let me now compile the full comprehensive response on VKC.
Vernal Keratoconjunctivitis (VKC)
Based on Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed. and The Wills Eye Manual
1. Definition
Vernal Keratoconjunctivitis (VKC) is a recurrent, bilateral, chronic allergic inflammatory disorder of the conjunctiva in which both IgE-mediated (Type I) and cell-mediated (Type IV) immune mechanisms play important roles. The term "vernal" (Latin for spring) reflects its seasonal predilection, though symptoms may be perennial in some patients.
2. Epidemiology
| Feature | Details |
|---|---|
| Sex | Predominantly boys (M:F ~3:1) |
| Age of onset | Usually from ~5 years onwards |
| Resolution | Spontaneous remission by late teens in 95% of cases; the remainder may transition to atopic keratoconjunctivitis (AKC) |
| Geography | Rare in temperate climates; common in warm, dry climates - Mediterranean, sub-Saharan Africa, Middle East, Indian subcontinent |
| Seasonality | Typically seasonal (peak: late spring/summer); mild perennial symptoms may persist |
| Atopy | In temperate regions, >90% have associated atopic conditions (asthma, eczema); two-thirds have a family history of atopy |
3. Pathogenesis
VKC is driven by a combined Type I (IgE-mediated) and Type IV (cell-mediated/T-cell) immune response:
- IgE pathway: Allergen cross-links IgE on sensitized mast cells in the conjunctiva - degranulation releases histamine, tryptase, prostaglandins, leukotrienes
- Cell-mediated: CD4+ Th2 lymphocytes predominate; they release IL-4, IL-5, IL-13, eotaxin - driving eosinophil recruitment and activation
- Eosinophils: Massively infiltrate the conjunctiva; release major basic protein (MBP) and eosinophil cationic protein (ECP), which cause epithelial toxicity and corneal damage
- Mast cells are increased in the conjunctival epithelium and stroma
- Fibroblast activation leads to collagen deposition forming the fibrovascular core of the giant papillae
4. Classification
VKC is classified based on the primary site of involvement:
| Type | Location | Ethnicity Predilection |
|---|---|---|
| Palpebral VKC | Upper tarsal conjunctiva (under upper eyelid) | All; more in Europeans |
| Limbal VKC | Corneoscleral limbus | Black and Asian patients |
| Mixed VKC | Both tarsal and limbal involvement | Any |
Palpebral disease carries higher risk of corneal complications due to close apposition of the inflamed tarsal conjunctiva against the corneal epithelium.
5. Clinical Features
Symptoms
- Intense itching - the hallmark symptom
- Lacrimation
- Photophobia
- Foreign body sensation / burning
- Thick ropy/mucoid discharge (stringy mucus - pathognomonic)
- Increased blinking
Signs - Palpebral Form
Early/Mild disease:
- Conjunctival hyperaemia
- Diffuse velvety papillary hypertrophy on the superior tarsal plate
Established disease - "Cobblestone" papillae:
- Macropapillae (<1 mm) - flat-topped, polygonal appearance; "cobblestone" pattern
- Focal or diffuse whitish inflammatory infiltrates between papillae in intense disease
Advanced disease - Giant papillae:
- Giant papillae (>1 mm) form when adjacent macropapillae amalgamate as dividing septa rupture
- Mucus deposition visible between giant papillae
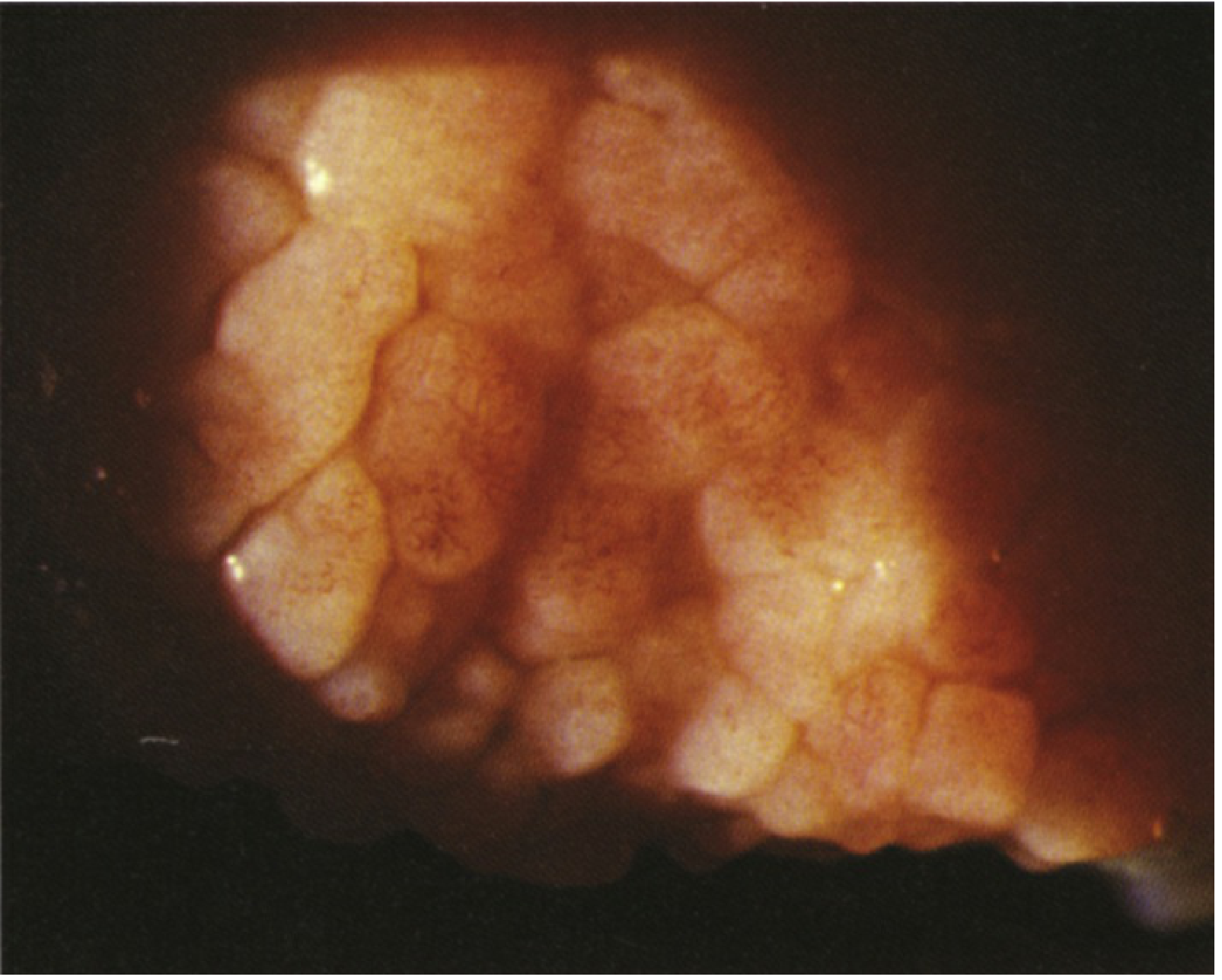
Giant cobblestone papillae of VKC on the superior tarsal conjunctiva - Wills Eye Manual
Signs - Limbal Form
- Gelatinous limbal papillae at the corneoscleral limbus
- Horner-Trantas dots - transient, apically located whitish cellular collections of degenerated eosinophils at the limbal papillae; pathognomonic of limbal VKC
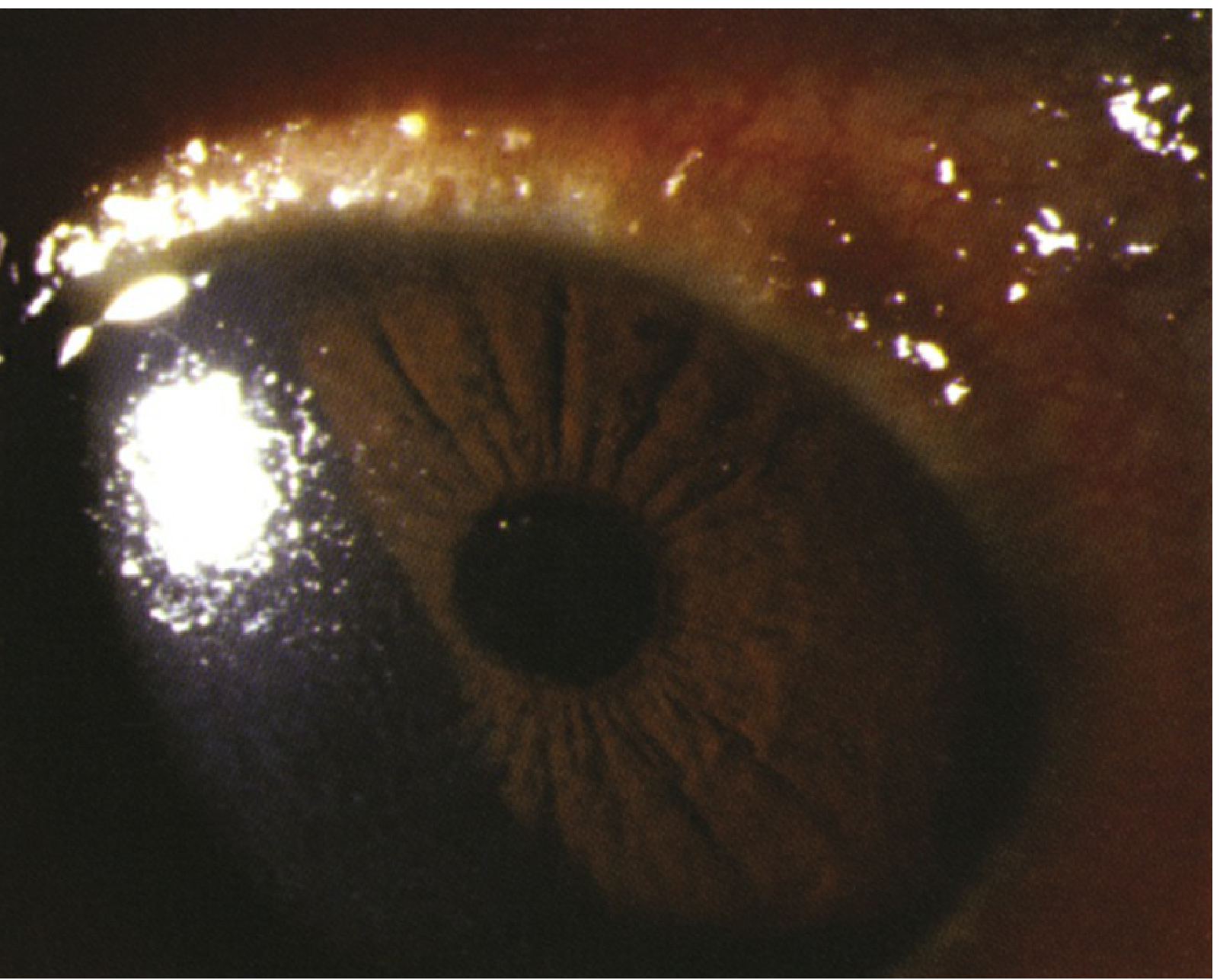
Horner-Trantas dots at the limbus in VKC - Wills Eye Manual
6. Corneal Complications (Vernal Keratopathy)
Corneal involvement is more frequent in palpebral VKC. It is the most sight-threatening aspect of VKC and can progress through stages:
| Stage | Description |
|---|---|
| Superior punctate epithelial erosions (SPE) | Fine epithelial erosions in the superior cornea associated with mucus layers |
| Epithelial macroerosions | From combined epithelial toxicity (mediators) and mechanical trauma from papillae |
| Shield ulcer | Well-delineated, sterile, grey-white infiltrate in the upper third of the cornea with overlying epithelial defect; develops when exposed Bowman's membrane is coated with mucus and calcium phosphate, preventing re-epithelialization |
| Plaque formation | Calcium-mucus plaque in the shield ulcer bed; prevents healing |
| Subepithelial scars | Grey, oval scars; may permanently reduce vision |
| Pseudogerontoxon | Band of superficial scarring resembling arcus senilis, adjacent to the previously inflamed limbus; a sequela of recurrent limbal disease |
Shield ulcer is a sight-threatening emergency - warrants urgent treatment to prevent secondary bacterial infection and permanent scarring.
Vascularization is not prominent in VKC (helps distinguish from other forms of keratitis).
7. Diagnosis
- Diagnosis is clinical - investigations are usually not required
- Conjunctival scraping: eosinophils are abundant (eosinophilia on Giemsa stain is supportive)
- Serum total IgE: may be elevated but non-specific
- Skin prick testing / RAST: identifies specific allergens; guides avoidance measures
- Slit-lamp examination is essential for grading severity and detecting corneal complications
8. Differential Diagnosis
| Condition | Key Differentiating Features |
|---|---|
| Atopic keratoconjunctivitis (AKC) | Adults; associated with atopic dermatitis; perennial; lower lid tarsal papillae more prominent; can cause scarring |
| Giant papillary conjunctivitis (GPC) | Contact lens wearers, prosthesis; mechanical cause; no Horner-Trantas dots; milder corneal involvement |
| Allergic conjunctivitis (simple) | Seasonal; watery discharge; no giant papillae; no corneal involvement |
| Trachoma | Follicles + pannus; Arlt's line (subconjunctival scarring); infective (Chlamydia) |
| Bacterial conjunctivitis | Purulent discharge; no giant papillae |
9. Treatment
Step 1 - Environmental Control / Avoidance
- Avoid identified allergens (dust, pollen, animal dander)
- Cold compresses - reduce histamine release and symptom relief
- Dark glasses / UV protection - reduces photophobia
- Air conditioning in rooms (reduces exposure to hot, dry air and allergens)
- Avoid eye rubbing (triggers mast cell degranulation)
Step 2 - Topical First-Line Therapy (Mild-Moderate Disease)
Mast-cell stabilizers / Antihistamine-mast cell stabilizer combinations are the backbone of prophylactic and maintenance therapy:
| Drug | Class | Dosing |
|---|---|---|
| Olopatadine 0.1% | Antihistamine + mast cell stabilizer | Twice daily |
| Olopatadine 0.2% / 0.7% | Same | Once daily |
| Alcaftadine 0.25% | Antihistamine + mast cell stabilizer | Once daily |
| Ketotifen 0.1% | Antihistamine + mast cell stabilizer | Twice daily |
| Lodoxamide 0.1% | Mast cell stabilizer (potent) | Four times daily |
| Sodium cromoglicate (cromolyn) 2-4% | Mast cell stabilizer | 4-6 times daily |
| Nedocromil 2% | Mast cell stabilizer | Twice daily |
| Pemirolast 0.1% | Mast cell stabilizer | Four times daily |
These should be started 2-3 weeks before allergy season begins for prophylactic effect.
Topical antihistamines (levocabastine, azelastine) for symptomatic relief.
Artificial tears (frequent use) - dilute and flush allergens; provide comfort.
Step 3 - Topical Corticosteroids (Moderate-Severe Disease)
Used for acute flares and severe disease; not recommended for long-term use due to steroid-related complications (glaucoma, cataract):
- Prednisolone acetate 1% drops - 4-6 times/day during exacerbations; taper
- Loteprednol etabonate 0.5% - softer steroid; less IOP risk; preferred for maintenance
- Dexamethasone 0.1% ointment - useful for shield ulcers
- Must monitor IOP on any topical steroid
Step 4 - Topical Calcineurin Inhibitors (Steroid-sparing)
- Cyclosporine A 0.05-2% (Restasis, Verkazia 0.1%) - inhibits T-cell activation and cytokine production; excellent for steroid-dependent cases
- Verkazia (0.1%): approved for severe VKC, 4x/day until resolution
- Restasis (0.05%): 4x/day
- Tacrolimus 0.03% ointment - also used topically in refractory cases
Step 5 - Systemic Therapy (Severe/Refractory Cases)
- Oral antihistamines - reduce systemic allergic background
- Oral corticosteroids - short courses for very severe acute exacerbations; avoid long-term
- Systemic cyclosporine - for very severe, sight-threatening refractory VKC
- Supratarsal corticosteroid injection (triamcinolone) - directly into the tarsal plate for palpebral giant papillae; effective for refractory cases; reduces papillae size
Step 6 - Management of Shield Ulcer
Shield ulcers require urgent, aggressive management:
- Topical steroid (prednisolone 1% or loteprednol) 4-6x/day
- Topical antibiotic (trimethoprim/polymyxin B QID, or erythromycin ointment) to prevent secondary infection
- Cycloplegic (cyclopentolate 1% TID) - reduces ciliary spasm and pain
- Mechanical debridement of the plaque (superficial keratectomy) if the plaque prevents re-epithelialization
- Bandage contact lens to protect the epithelium and promote healing
- Mitomycin C (MMC) - topical 0.02% may be used to prevent recurrence of plaques
Step 7 - Surgical Management
- Surgical debridement / superficial keratectomy of shield ulcer plaques that resist medical treatment
- Papillectomy - rarely required; for very large giant papillae causing mechanical corneal damage
- Cryotherapy to papillae
10. VKC vs. AKC - Key Comparison
| Feature | VKC | AKC |
|---|---|---|
| Age | Children, teens | Adults (20-50 yrs) |
| Sex | Predominantly male | Male |
| Season | Spring/summer | Perennial |
| Skin disease | No | Atopic dermatitis (eyelids) |
| Papillae | Upper tarsus (large) | Lower + upper tarsus |
| Horner-Trantas | Yes (limbal form) | Occasional |
| Corneal scarring | Yes (shield ulcer) | Yes (more severe) |
| Prognosis | Good (remits ~20 yrs) | Can cause blindness |
| Subconjunctival fibrosis | Rare | Common |
11. Prognosis
- 95% undergo spontaneous remission in the late teens
- The remaining 5% may develop atopic keratoconjunctivitis (AKC), which is a more severe, potentially blinding condition
- With corneal complications (especially shield ulcers), permanent subepithelial scarring and reduced vision are possible if treatment is delayed
- Regular follow-up is essential during active disease; steroid monitoring (IOP checks) is mandatory
Summary Table
| Feature | VKC |
|---|---|
| Pathology | Type I + Type IV hypersensitivity |
| Key cell | Mast cells, eosinophils, Th2 lymphocytes |
| Hallmark symptom | Intense itching + ropy discharge |
| Palpebral sign | Cobblestone giant papillae (upper tarsus) |
| Limbal sign | Horner-Trantas dots |
| Corneal complication | Shield ulcer (sterile) |
| Conjunctival scraping | Eosinophils |
| First-line Rx | Mast cell stabilizers / dual-action antihistamines |
| Steroid-sparing | Topical cyclosporine A (Verkazia) |
| Remission | ~95% by late teens |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed. (ISBN 9780443110993); The Wills Eye Manual (ISBN 9781975160753)
This is a shared conversation. Sign in to Orris to start your own chat.