A patient of 37 years of age, with approximately 24 weeks size mass arising from pelvis, solid, firm, mobile mass. USG s/o posterior mayo
Reading File
Finding Sources
Finding Sources
Searching the Web
posterior myoma uterine fibroid 24 weeks size pelvic mass management
Finding Sources
Finding Sources
Searching PubMed
uterine leiomyoma large pelvic mass management myomectomy
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive clinical analysis of this case:
Clinical Case: 37-Year-Old Female — Posterior Uterine Myoma (Leiomyoma), 24-Weeks Size
Diagnosis: Uterine Leiomyoma (Posterior Wall Myoma)
The USG finding of a posterior myoma (posterior wall fibroid) combined with the clinical triad of:
- Solid, firm, mobile pelvic mass
- 24-weeks uterine size
- Age 37 (reproductive age, premenopausal)
...is classic for a large uterine leiomyoma.
FIGO Classification
Posterior wall myomas are most often intramural or subserosal. The FIGO classification system helps guide management:
| Type | Description |
|---|---|
| 4 | Intramural, entirely within myometrium |
| 5 | Subserosal, ≥50% intramural |
| 6 | Subserosal, <50% intramural |
| 7 | Pedunculated subserosal |
A posterior location is significant because it may compress the rectum, cause backache, or complicate surgery due to proximity to the ureter and rectum.
Clinical Features Supporting This Diagnosis
- Enlarged, irregularly shaped, firm, nontender uterus on bimanual examination — pathognomonic for fibroids
- Mobile — suggests no malignant infiltration or pelvic fixation
- Solid on USG — consistent with leiomyoma (vs. cystic ovarian mass)
- At 24-weeks size, this is a giant fibroid — one of the largest categories
Key Differential Diagnoses to Exclude
| Condition | Features that help differentiate |
|---|---|
| Ovarian tumor (solid) | Arises separately from uterus, different mobility axis |
| Leiomyosarcoma | Rapid growth, pain, age >50, postmenopausal; LMS prevalence is only 1/1,960 surgeries for presumed fibroids (0.051%) |
| Adenomyoma | Tenderness, dysmenorrhea, poorly defined borders |
| Retroperitoneal sarcoma | Fixed, no uterine connection |
Important: "Rapid uterine growth" in premenopausal women almost never indicates sarcoma — only 1 sarcoma was found among 371 (0.26%) women operated on for rapid fibroid growth. The risk of leiomyosarcoma at myomectomy is approximately 4–7/10,000.
Investigations Required
- Ultrasound (done) — confirm posterior wall location, assess vascularity with Doppler
- MRI pelvis — gold standard for fibroid mapping; differentiates leiomyoma from LMS (enhancement pattern on Gd-DTPA); also detects adenomyosis
- CBC — assess for anemia (heavy menstrual bleeding is common)
- LFT/RFT, coagulation — preoperative workup
- CA-125 — to help exclude ovarian malignancy (non-specific)
- Endometrial biopsy — if abnormal uterine bleeding present
- LDH and its isoenzymes — elevated in LMS; helps differentiate from degenerating fibroid
Symptoms to Elicit
- Heavy/prolonged menstrual bleeding (most common — from submucosal component or increased endometrial surface)
- Pelvic pressure, bulk symptoms
- Urinary frequency/urgency (anterior displacement of bladder)
- Constipation/tenesmus (especially with posterior myoma compressing rectum)
- Infertility or recurrent pregnancy loss
- Backache (posterior myoma compresses lumbar nerves)
Management
Patient is 37 years old → Fertility Preservation is a Priority
Medical (Bridging/Preoperative):
- GnRH agonists (leuprolide) — shrink fibroid size (15–40%), reduce uterine size from ~15 weeks → ~11 weeks; allow vaginal approach; treat preoperative anemia
- IV iron infusion if Hb <9 g/dL (more effective than oral iron — increases Hb by 3.0 vs 0.8 g/dL)
- Tranexamic acid / NSAIDs — for menorrhagia symptom control
Surgical (Definitive):
Since she is 37, premenopausal, and at 24-weeks size, the primary surgical option is:
1. Abdominal Myomectomy (Open) — Preferred for this case
- Uterus-preserving, safe alternative to hysterectomy
- Case-controlled studies show less intraoperative injury with myomectomy vs. hysterectomy at similar uterine sizes (14–15 weeks); blood loss actually less with myomectomy (227 mL vs. 484 mL for hysterectomy)
- At 24-weeks size, laparoscopic approach has technical limitations → open myomectomy preferred
- Posterior myoma requires a posterior uterine incision; retroperitoneal dissection may be needed due to proximity to ureter/rectosigmoid
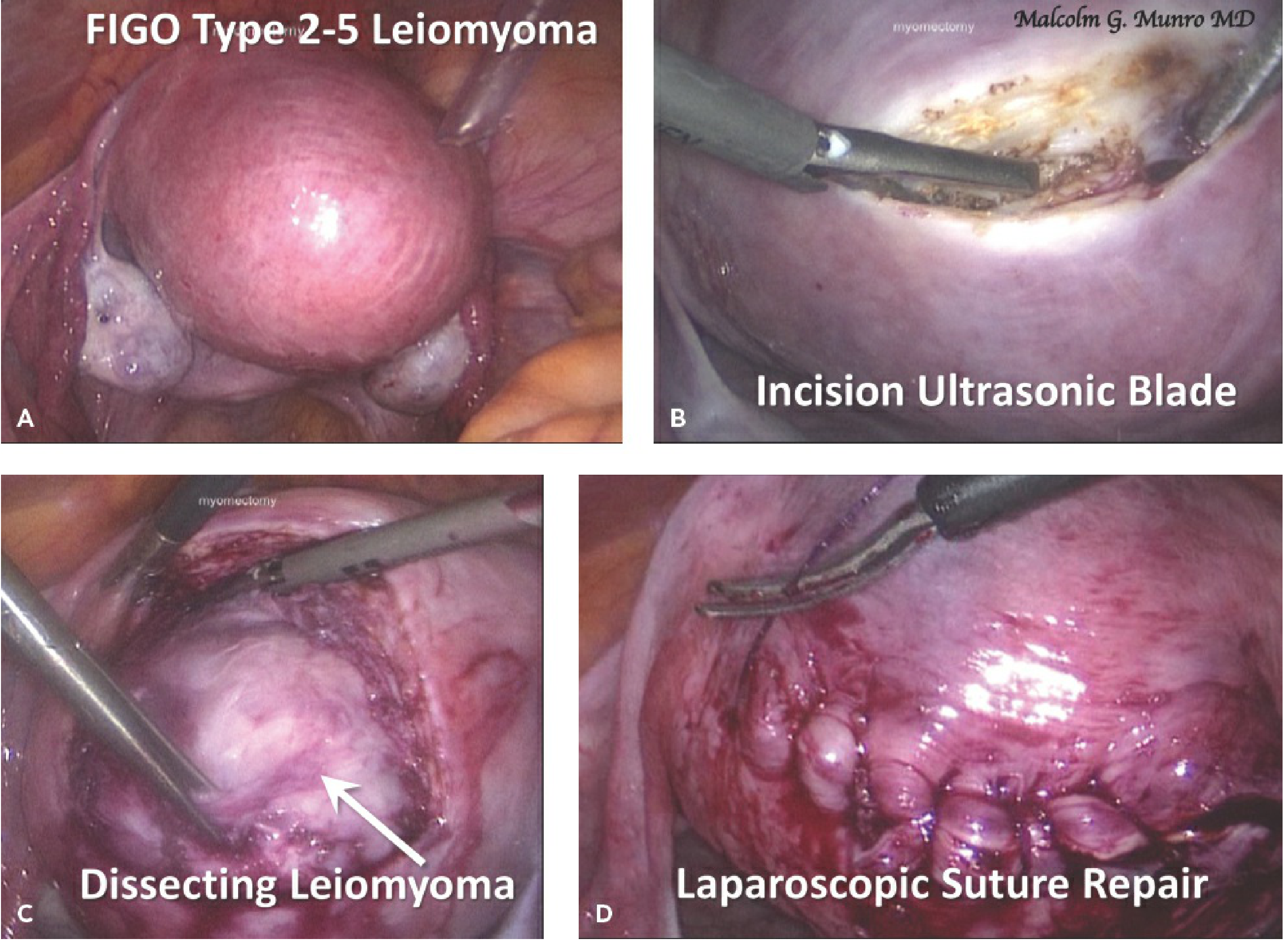
2. Laparoscopic Myomectomy — Limited role at this size
- Better for fibroids <10 cm / fewer than 3–4 fibroids
- Requires multilayer suture closure of myometrium; limited electrosurgery
- Risk of uterine rupture in future pregnancy if closure is inadequate
3. Hysterectomy — Only if:
- Family complete and patient consents
- Severe symptoms unresponsive to conservative measures
4. Uterine Artery Embolization (UAE)
- Non-surgical; reduces fibroid size by ~40%
- Not preferred if future fertility desired (evidence of reduced ovarian reserve and obstetric complications post-UAE)
Specific Considerations for Posterior Myoma
| Issue | Relevance |
|---|---|
| Rectovaginal septum/rectum adhesion | Careful dissection required; bowel prep advisable |
| Ureteral proximity | Risk of ureteral injury; consider ureteral stents intraoperatively |
| Posterior incision → adhesions | Posterior peritoneal closure important; anti-adhesion barriers may be used |
| Access difficulty | May require retroperitoneal approach; longer operative time |
Recurrence After Myomectomy
- Recurrence rate: approximately 27% at 5 years by ultrasound; symptomatic recurrence ~11%
- Higher in younger women and those with multiple fibroids
- GnRH agonists postoperatively may slow recurrence
Post-Myomectomy Pregnancy Counseling
- Uterine rupture risk in subsequent pregnancy: 0.47% with trial of labor after myomectomy
- Cesarean section is typically recommended if deep myometrial entry was made during myomectomy
- Risk increases if only single-layer closure was performed or electrocautery was heavily used
Sources: Berek & Novak's Gynecology (9th ed.), Chapter 11 — Uterine Fibroids; Chapter 26 — Myomectomy Techniques
This is a shared conversation. Sign in to Orris to start your own chat.