AwMI ecg
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer on Anterior MI (AwMI) ECG findings.
Anterior Wall MI (AwMI) - ECG
Anatomy and Culprit Vessel
The anterior wall of the left ventricle is supplied by the left anterior descending (LAD) artery. LAD occlusion is the most common cause of anterior STEMI.
Diagnostic Criteria for STEMI (Fourth Universal Definition)
New ST elevation of >1 mm in at least 2 contiguous leads, except V2-V3 where the thresholds are:
- Women (any age): ≥1.5 mm
- Men <40 years: ≥2.5 mm
- Men >40 years: ≥2 mm
Leads and ECG Changes in Anterior MI
| Territory | Leads with ST Elevation | Reciprocal Changes |
|---|---|---|
| Anterior wall (AwMI) | V1-V4 | ST depression in III, aVF |
| Anterolateral | V1-V6, I, aVL | ST depression in III, aVF |
| Septal | V1-V2 | - |
| High lateral | I, aVL | ST depression in III, aVF, V1 |
Sequential ECG Evolution in Anterior MI
1. Hyperacute T waves (earliest sign, within minutes)
- Tall, broad-based, asymmetrical T waves in V3-V4
- ST segment begins to rise at the J point
- Transient - progresses rapidly to overt STE
2. ST segment elevation - develops as infarction progresses
- Morphology: flat/oblique, convex ("domed"), or "tombstoned"
- Concave morphology is atypical for STEMI; more common in BER or pericarditis
3. Q waves - marker of irreversible necrosis
- Pathologic Q waves appear within 1 hour but most commonly at 8-12 hours
- Persist as permanent markers of prior infarction (may disappear over time)
- Presence of Q waves with STE does NOT preclude reperfusion therapy
4. T wave inversions - evolve as MI matures (post-reperfusion or completed infarct)
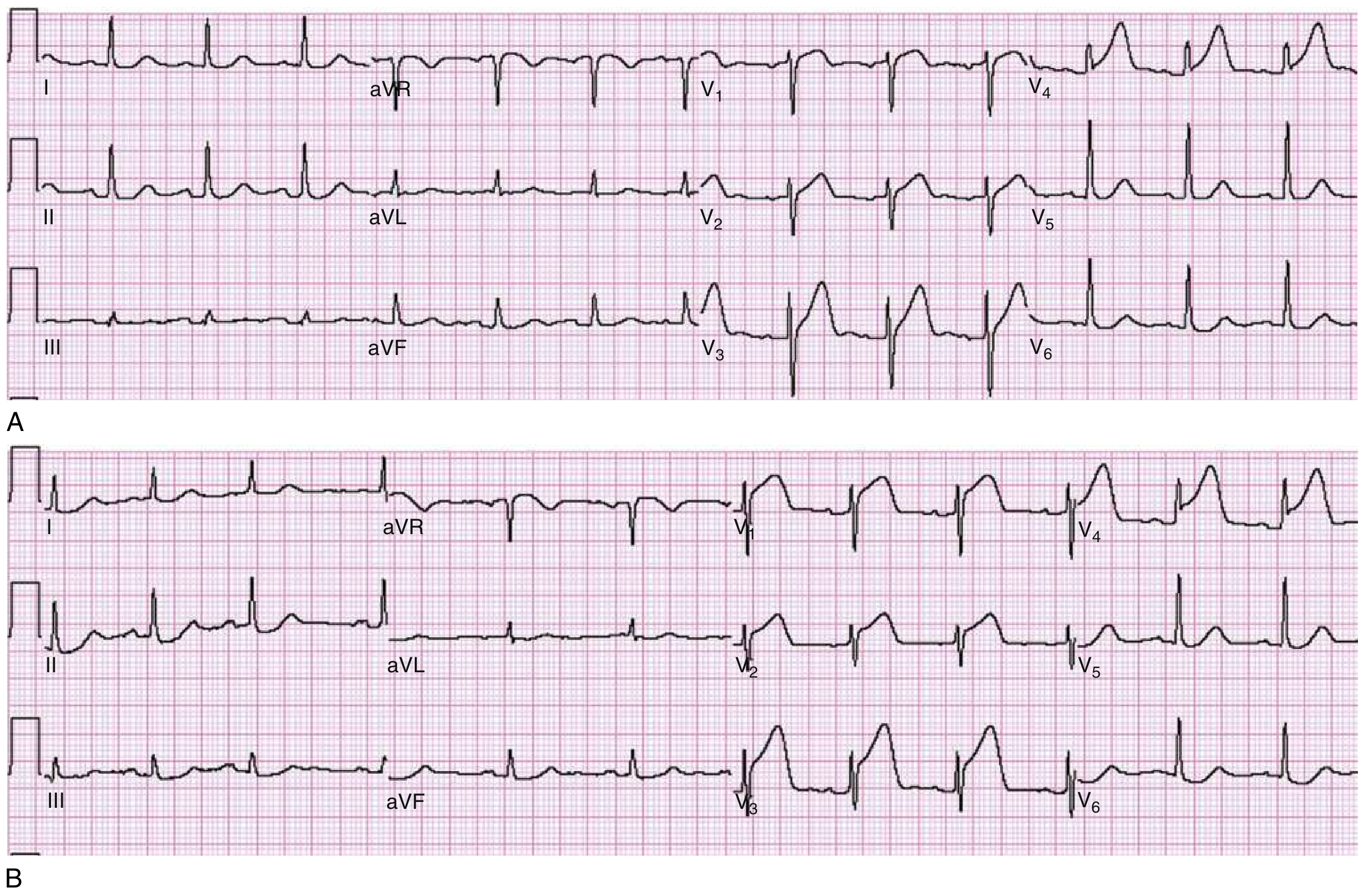
Anterior Wall STEMI - Classic ECG
Anterolateral STEMI - ECG
STEMI-Equivalents / Special Patterns (LAD-related)
Wellens Syndrome
- Deep symmetrical T wave inversions (Type A/I) or biphasic T wave changes (Type B/II) in anterior precordial leads (V2-V3)
- ST segment isoelectric or minimally elevated (<1 mm); no Q waves
- May occur pain-free or with chest pain; may or may not have elevated troponin
- Indicates critical proximal LAD stenosis - natural history is progression to anterior STEMI
- Stress testing is contraindicated in Wellens syndrome
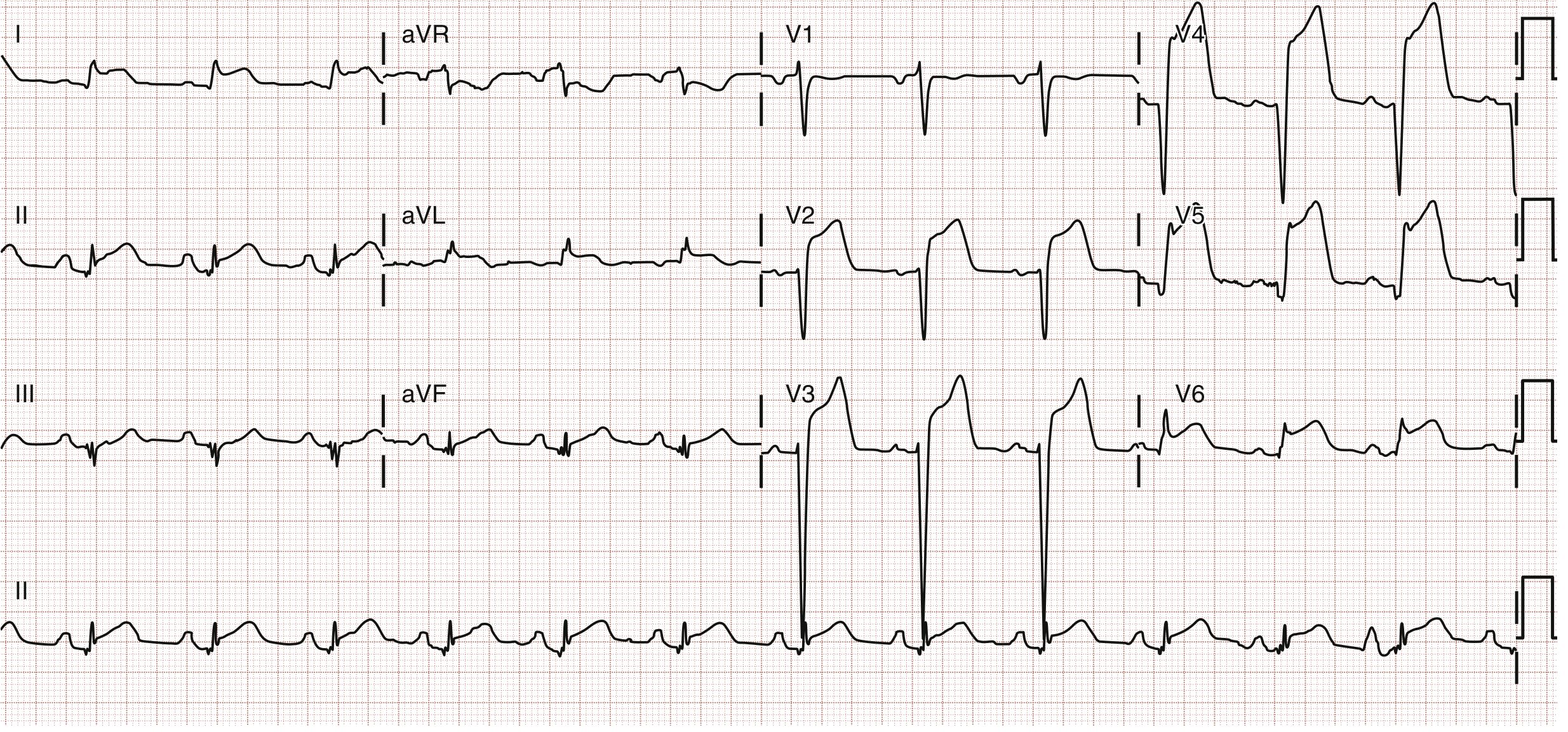
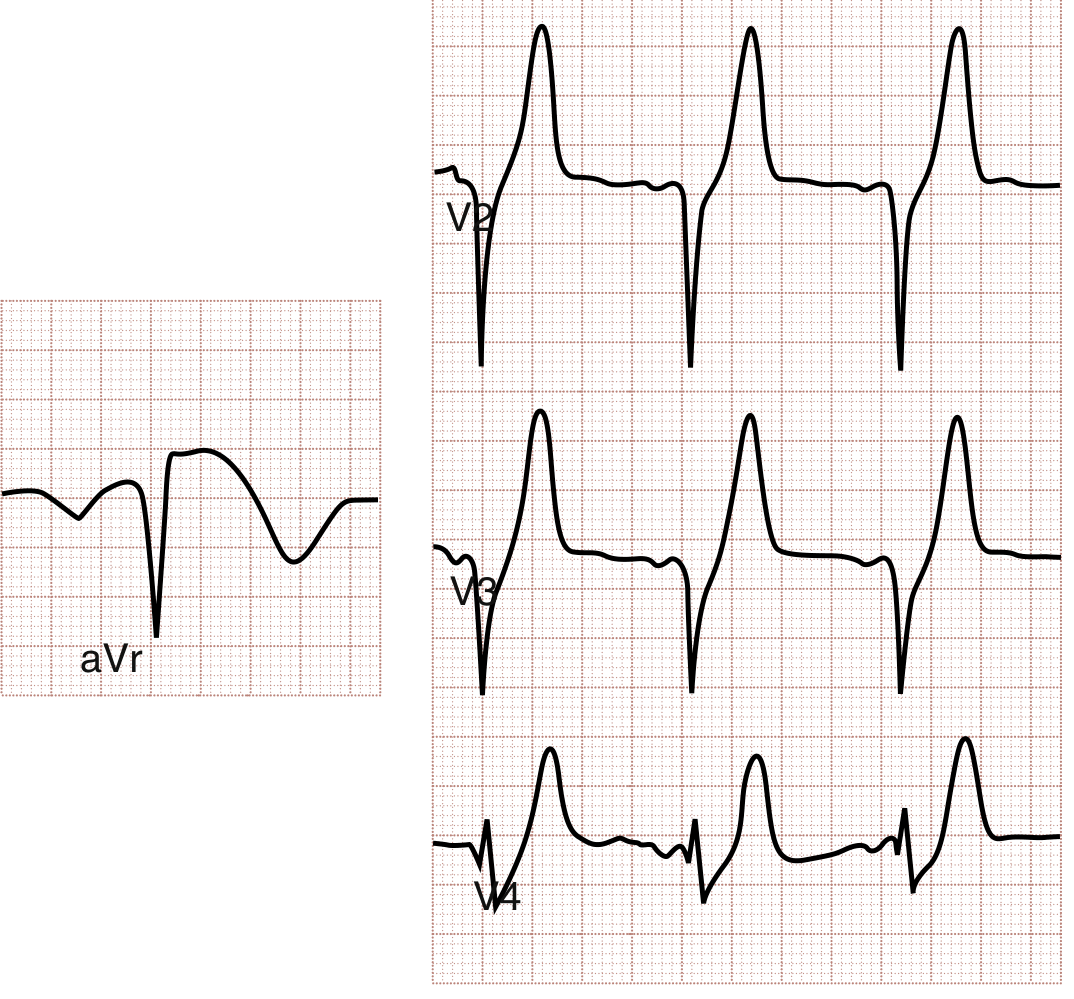
de Winter Pattern
- ST depression (not elevation) at J point with prominent, hyperacute upright T waves in precordial leads
- ST elevation in aVR
- Associated with proximal LAD occlusion - treat as STEMI-equivalent
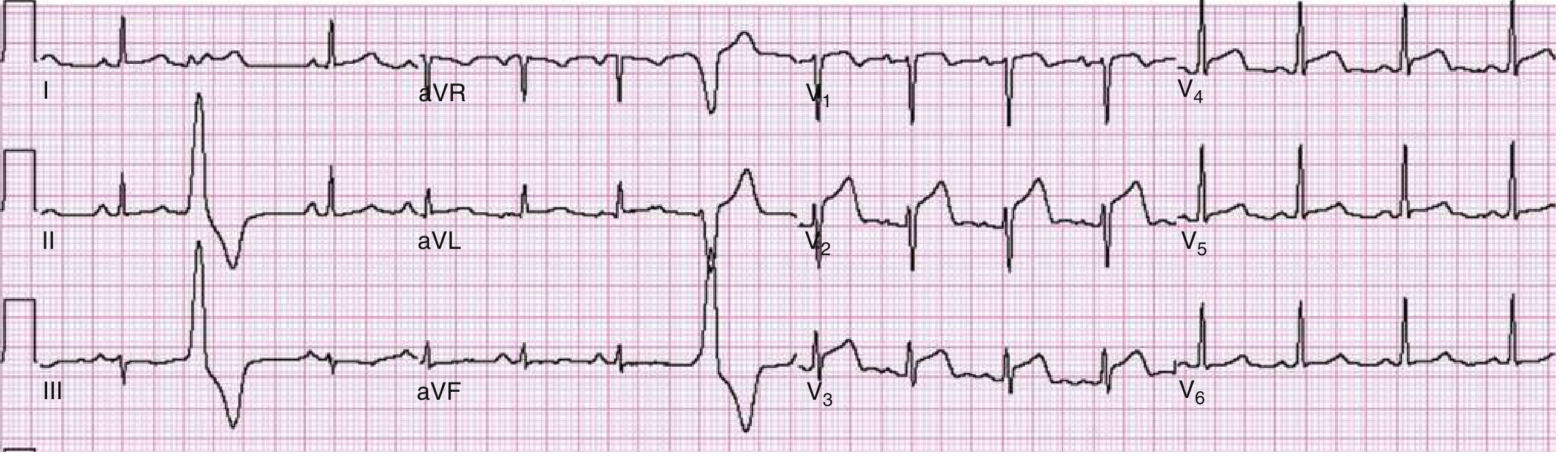
aVR Elevation Pattern (Left Main / Proximal LAD)
- ST elevation in aVR (>0.5 mV) with widespread ST depression in other leads
- ~78% sensitive, ~83% specific for left main coronary artery disease
- If STE is greater in aVR than V1 → left main; greater in V1 than aVR → proximal LAD
Key Points Summary
| Finding | Significance |
|---|---|
| STE V1-V4 | Anterior STEMI (LAD occlusion) |
| STE V1-V6 + I, aVL | Anterolateral STEMI (proximal LAD or diagonal) |
| Reciprocal STD in III, aVF | Increases specificity for anterior STEMI |
| Hyperacute T waves in V3-V4 | Earliest sign - may precede overt STE |
| Deep symmetrical TWI in V2-V3 | Wellens syndrome - critical LAD stenosis |
| J-point STD + tall T waves precordially + STE in aVR | De Winter pattern - proximal LAD STEMI-equivalent |
| STE in aVR > V1 + diffuse STD | Left main or multivessel disease |
| Q waves V1-V4 | Established/completed anterior infarction |
Sources: Rosen's Emergency Medicine, 9th Ed., Ch. 64 (ECG Abnormalities in ACS); Table 64.4 (Regional ST Changes in AMI)
This is a shared conversation. Sign in to Orris to start your own chat.