teach me the lower limb in detail in organize way
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Excellent! I have all the key images and content. Now let me compile the comprehensive, organized lower limb anatomy guide.
The Lower Limb - A Complete Organized Guide
Source: Gray's Anatomy for Students
Overview: Regions of the Lower Limb
The lower limb is divided into four main regions based on major joints, component bones, and superficial landmarks:
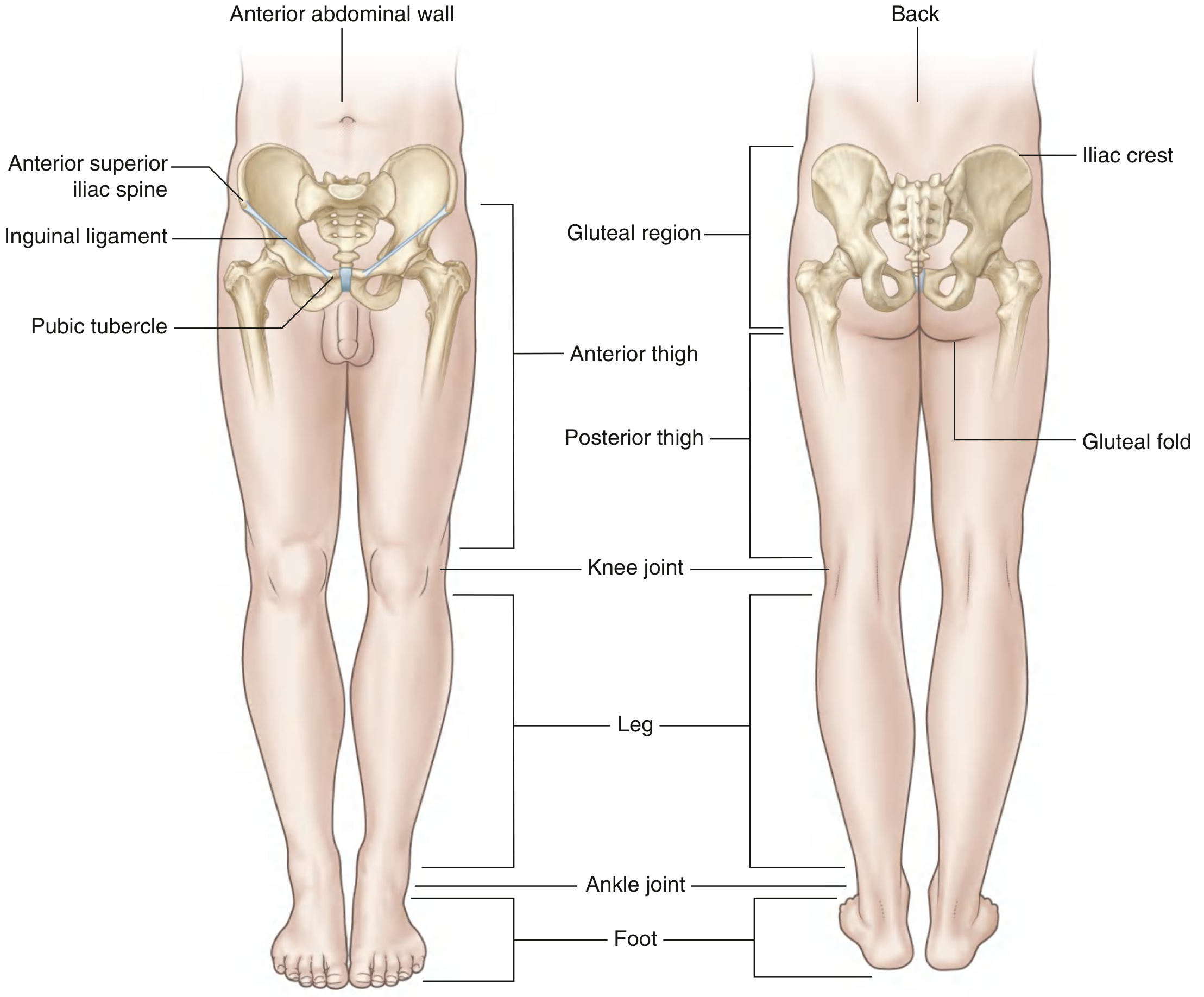
| Region | Boundaries |
|---|---|
| Gluteal region | Posterolateral; between the iliac crest and the gluteal fold |
| Thigh | Anteriorly between the inguinal ligament and the knee; posteriorly between the gluteal fold and the knee |
| Leg | Between the knee joint and the ankle joint |
| Foot | Distal to the ankle joint |
Three key areas of transition connect the regions:
- Femoral triangle - pyramid-shaped depression in the proximal thigh, where major blood supply and the femoral nerve enter from the abdomen under the inguinal ligament
- Popliteal fossa - diamond-shaped region posterior to the knee, where major vessels and nerves pass between thigh and leg
- Tarsal tunnel - posteromedial ankle canals formed by bones and the flexor retinaculum, through which nerves, vessels, and flexor tendons pass between leg and foot
Part 1: Bones of the Lower Limb
1.1 The Pelvis / Hip Bone (Pelvic Girdle)
The pelvic girdle anchors the lower limb to the axial skeleton. The key landmarks include:
- Iliac crest - the superior rim, ending anteriorly as the anterior superior iliac spine (ASIS) and posteriorly as the posterior superior iliac spine (PSIS)
- Anterior inferior iliac spine (AIIS) - attachment for the rectus femoris
- Ischial tuberosity - the bony prominence you sit on; attachment for the hamstring muscles
- Acetabulum - the cup-shaped socket for the femoral head (hip joint)
- The gluteal surface of the ilium is divided by three curved lines (inferior, anterior, and posterior gluteal lines) that define the attachment zones for gluteus minimus, medius, and maximus
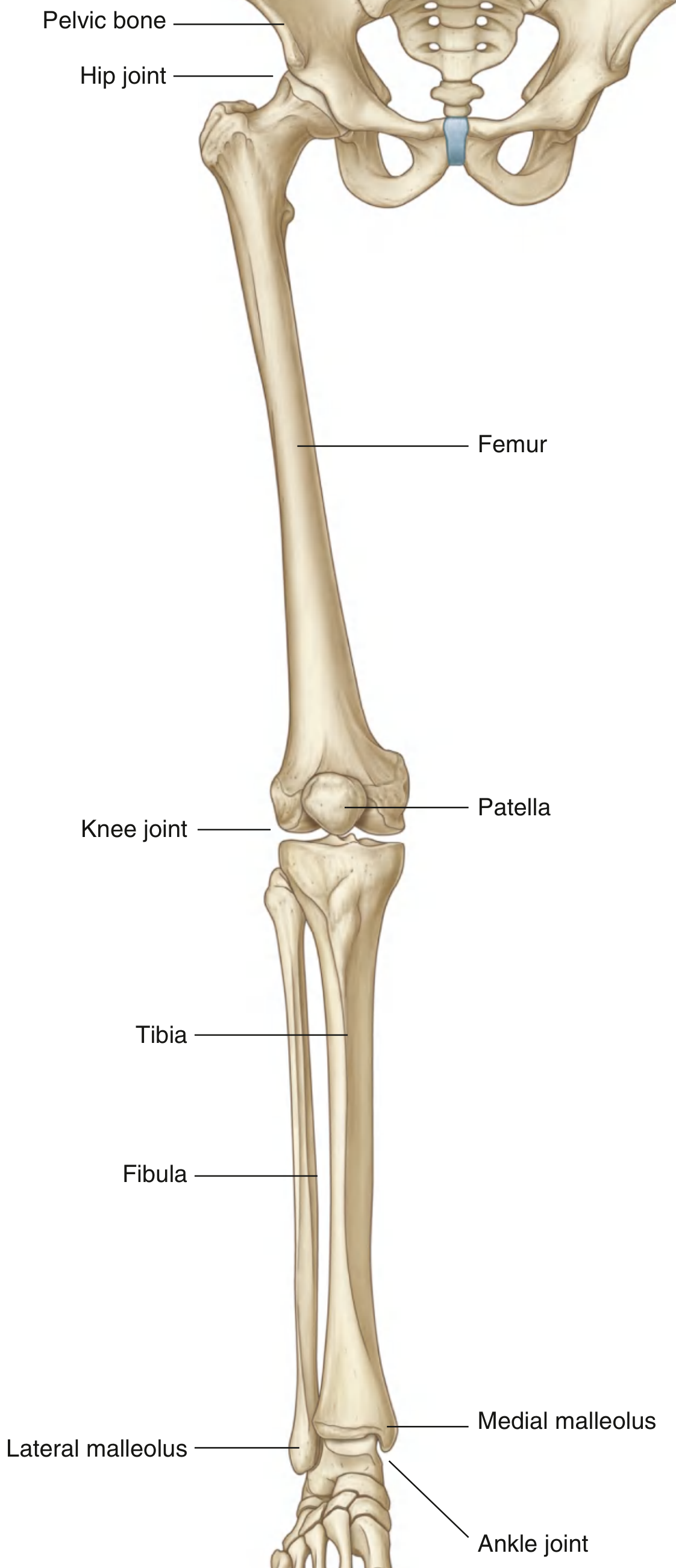
1.2 The Femur
The largest bone in the body. Key features:
- Head - articulates with the acetabulum; blood supply comes primarily from an arterial ring formed by the medial and lateral circumflex femoral arteries around the femoral neck
- Neck - connects the head to the shaft at an angle; fractures here can interrupt blood supply to the femoral head (avascular necrosis risk)
- Greater and lesser trochanters - prominent projections for muscle attachments
- Intertrochanteric line (anterior) and intertrochanteric crest (posterior) - connect the trochanters
- Linea aspera - the major posterior ridge of the shaft; a key site for multiple muscle attachments. In the proximal femur it splits into the pectineal line (medially) and gluteal tuberosity (laterally)
- The shaft descends at 7 degrees from vertical, so the distal end is closer to the midline than the proximal shaft
- Medial and lateral condyles distally - articulate with the tibia
1.3 The Patella
- The largest sesamoid bone in the body, embedded within the quadriceps tendon
- Protects the knee joint anteriorly and improves the mechanical advantage of the quadriceps
1.4 Tibia and Fibula (Leg Bones)
Tibia (medial, weight-bearing):
- Medial and lateral condyles proximally articulate with the femoral condyles
- Tibial plateau - the superior articular surface
- Tibial tuberosity - anterior prominence, attachment for patellar ligament
- Medial malleolus distally forms part of the ankle mortise
Fibula (lateral, non-weight-bearing):
- Mainly for muscle attachment and ankle stability
- Lateral malleolus distally forms the lateral wall of the ankle mortise
1.5 Bones of the Foot
- Tarsal bones (7): Talus, calcaneus (heel bone), navicular, cuboid, and 3 cuneiforms (medial, intermediate, lateral). Organized in two rows with the navicular as an intermediate bone on the medial side
- Metatarsals (5): One per digit; connected distally by deep transverse metatarsal ligaments
- Phalanges: Three per toe except the great toe (digit I) which has only two (proximal and distal)
Arches of the foot:
- Medial longitudinal arch (higher, more flexible) - supported by the calcaneus, talus, navicular, cuneiforms, and metatarsals I-III
- Lateral longitudinal arch (flatter) - supported by calcaneus, cuboid, and metatarsals IV-V
- Transverse arch - formed across the width of the foot at the level of the cuneiforms and cuboid
- These arches act as shock absorbers and reduce the energy cost of walking
Part 2: Muscles of the Lower Limb
2.1 Gluteal Region Muscles
| Muscle | Action | Nerve |
|---|---|---|
| Gluteus maximus | Hip extension, lateral rotation | Inferior gluteal (L5-S2) |
| Gluteus medius | Hip abduction, medial rotation | Superior gluteal (L4-S1) |
| Gluteus minimus | Hip abduction, medial rotation | Superior gluteal (L4-S1) |
| Tensor fasciae latae | Abduction, medial rotation; tenses iliotibial tract | Superior gluteal (L4-S1) |
| Piriformis | Lateral rotation, abduction | S1-S2 |
| Obturator internus | Lateral rotation | L5-S2 |
| Superior/inferior gemellus | Lateral rotation | L4-S2 |
| Quadratus femoris | Lateral rotation | L4-S1 |
The gluteus medius and minimus are the primary hip abductors - they hold the pelvis level during walking (a positive Trendelenburg sign means they are weak or their nerve is damaged).
2.2 Thigh Muscles
Anterior compartment (innervated by femoral nerve):
| Muscle | Action |
|---|---|
| Iliopsoas (iliacus + psoas major) | Flex hip (exits under inguinal ligament) |
| Rectus femoris | Flex hip + extend knee |
| Vastus lateralis | Extend knee |
| Vastus medialis | Extend knee |
| Vastus intermedius | Extend knee |
| Sartorius | Flex, abduct, laterally rotate hip; flex knee |
| Pectineus | Flex and adduct hip |
Together, the four vasti and rectus femoris form the quadriceps femoris - the most powerful extensor of the knee.
Medial compartment (adductors) (mainly obturator nerve, L2-L4):
| Muscle | Action |
|---|---|
| Adductor longus | Adduct and flex hip |
| Adductor brevis | Adduct and flex hip |
| Adductor magnus | Adduct and extend hip (dual innervation: obturator + tibial) |
| Gracilis | Adduct hip; flex and medially rotate knee |
| Obturator externus | Laterally rotate hip |
Posterior compartment (hamstrings) (innervated by sciatic nerve - tibial division, except short head of biceps femoris which is innervated by the common fibular division):
| Muscle | Action |
|---|---|
| Biceps femoris (long + short head) | Flex knee, extend hip, laterally rotate leg |
| Semitendinosus | Flex knee, extend hip, medially rotate leg |
| Semimembranosus | Flex knee, extend hip, medially rotate leg |
All three hamstrings originate from the ischial tuberosity (except short head of biceps).
2.3 Leg Muscles
Anterior compartment (deep fibular nerve):
| Muscle | Action |
|---|---|
| Tibialis anterior | Dorsiflexion + inversion |
| Extensor digitorum longus | Extends toes 2-5, dorsiflexion |
| Extensor hallucis longus | Extends great toe, dorsiflexion |
| Fibularis (peroneus) tertius | Dorsiflexion + eversion |
Lateral compartment (superficial fibular nerve):
| Muscle | Action |
|---|---|
| Fibularis (peroneus) longus | Plantarflexion + eversion; supports transverse arch |
| Fibularis (peroneus) brevis | Eversion |
Posterior compartment (tibial nerve):
Superficial group:
- Gastrocnemius - powerful plantarflexion; also flexes knee (two heads from femoral condyles)
- Soleus - plantarflexion (deeper, from tibia/fibula)
- Plantaris - weak plantarflexion (vestigial)
- Together gastrocnemius + soleus form the triceps surae, attaching via the calcaneal (Achilles) tendon to the calcaneus
Deep group:
- Tibialis posterior - plantarflexion + inversion; supports medial arch
- Flexor digitorum longus - flexes toes 2-5
- Flexor hallucis longus - flexes great toe; supports medial arch
2.4 Foot Muscles (Intrinsic)
The foot has intrinsic muscles in both the dorsum and the sole (4 layers). They fine-tune toe movements and support the arches. Mostly innervated by branches of the tibial nerve (medial and lateral plantar nerves). The dorsal intrinsics are innervated by the deep fibular nerve.
Part 3: Joints of the Lower Limb
3.1 Hip Joint
- Type: Ball-and-socket (multiaxial synovial joint)
- Articular surfaces: Head of femur + acetabulum (deepened by the fibrocartilaginous acetabular labrum)
- Movements: Flexion, extension, abduction, adduction, medial/lateral rotation, circumduction
- Key ligaments:
- Iliofemoral ligament (Y-ligament of Bigelow) - strongest in the body; prevents hyperextension
- Pubofemoral ligament - limits abduction and extension
- Ischiofemoral ligament - limits medial rotation and extension
- Ligament of the head of the femur (ligamentum teres) - carries a small artery to the femoral head (minor blood supply in adults)
- Blood supply to femoral head: Primarily from medial and lateral circumflex femoral arteries forming a ring around the femoral neck; these are vulnerable in femoral neck fractures
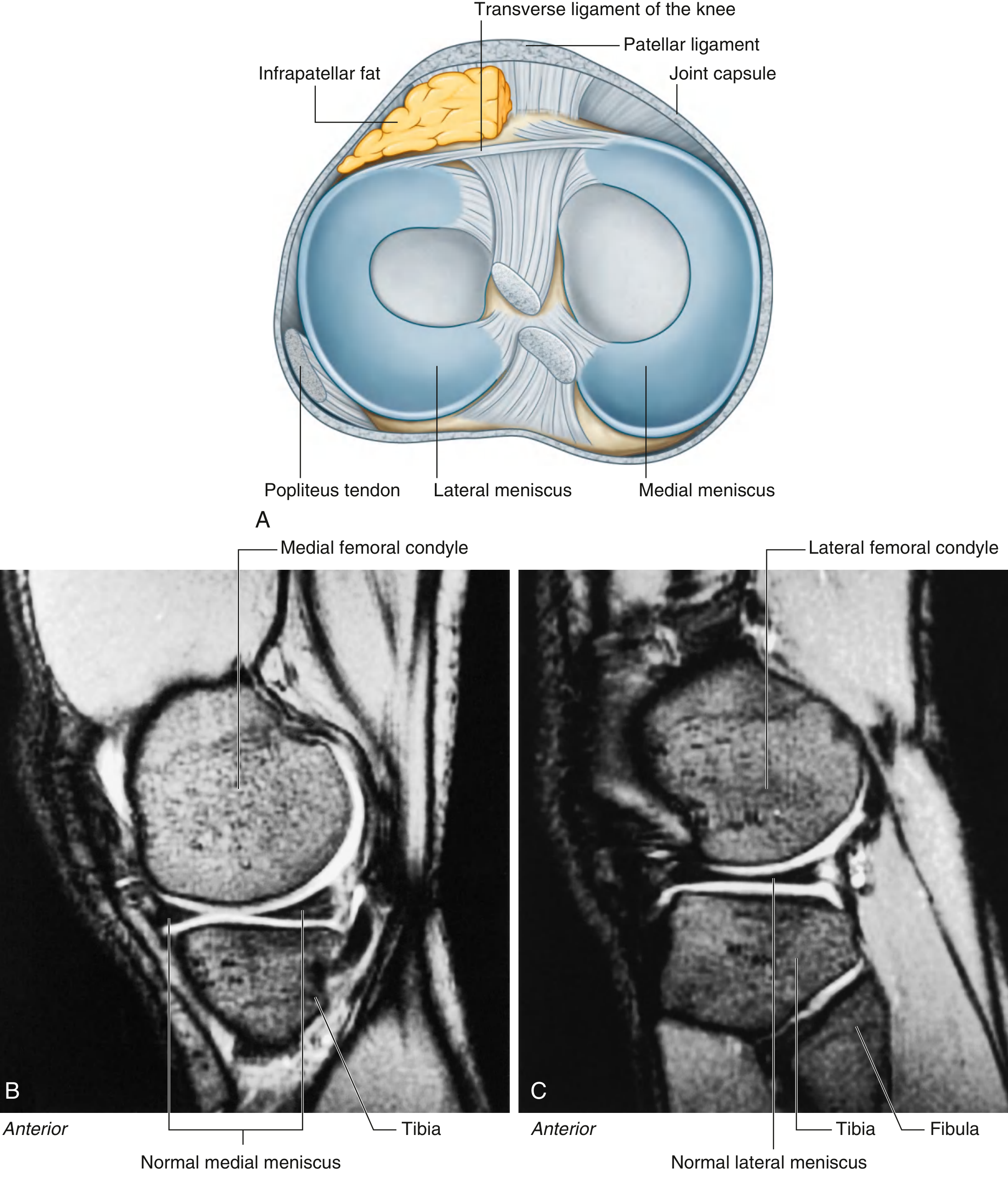
3.2 Knee Joint
- Type: Modified hinge joint (allows flexion/extension + limited rotation when flexed)
- Articular surfaces: Medial and lateral femoral condyles + tibial condyles + patella (patellofemoral component)
- Menisci: Medial and lateral C-shaped fibrocartilage pads that improve congruency and act as shock absorbers. The medial meniscus is attached to the medial collateral ligament, making it more prone to injury. Tears present with joint line pain, locking, clicking, and swelling; diagnosed by MRI.
- Cruciate ligaments (inside the joint):
- Anterior cruciate ligament (ACL) - prevents anterior translation of tibia on femur; taut in extension
- Posterior cruciate ligament (PCL) - prevents posterior translation; the stronger of the two
- Collateral ligaments (outside the joint):
- Medial (tibial) collateral ligament (MCL) - resists valgus stress
- Lateral (fibular) collateral ligament (LCL) - resists varus stress
- The "unhappy triad" of knee injury: ACL + MCL + medial meniscus (commonly torn together in contact sports)
- Screw-home mechanism: Terminal extension of the knee involves medial rotation of the femur, "locking" the joint for efficient standing. Unlocking requires the popliteus muscle.
3.3 Ankle Joint (Talocrural Joint)
- Type: Hinge joint (uniaxial synovial)
- Articular surfaces: Distal tibia + medial malleolus + lateral malleolus forming a mortise around the trochlea of the talus
- Movements: Dorsiflexion (tibia and fibula) and plantarflexion (talus)
- Key ligaments:
- Medial (deltoid) ligament - broad, strong; connects medial malleolus to tarsal bones; resists eversion
- Lateral ligaments - three bands (anterior talofibular, calcaneofibular, posterior talofibular); resist inversion; most commonly sprained (anterior talofibular is torn first in inversion sprains)
3.4 Subtalar & Midfoot Joints
- Subtalar (talocalcaneal) joint + transverse tarsal joint = responsible for inversion and eversion of the foot
- Tarsometatarsal joints - allow limited sliding movements only
- Metatarsophalangeal joints - allow flexion, extension, abduction, and adduction
Part 4: Nerves of the Lower Limb
The lower limb is innervated by the lumbar plexus (L1-L4) and sacral plexus (L4-S3).
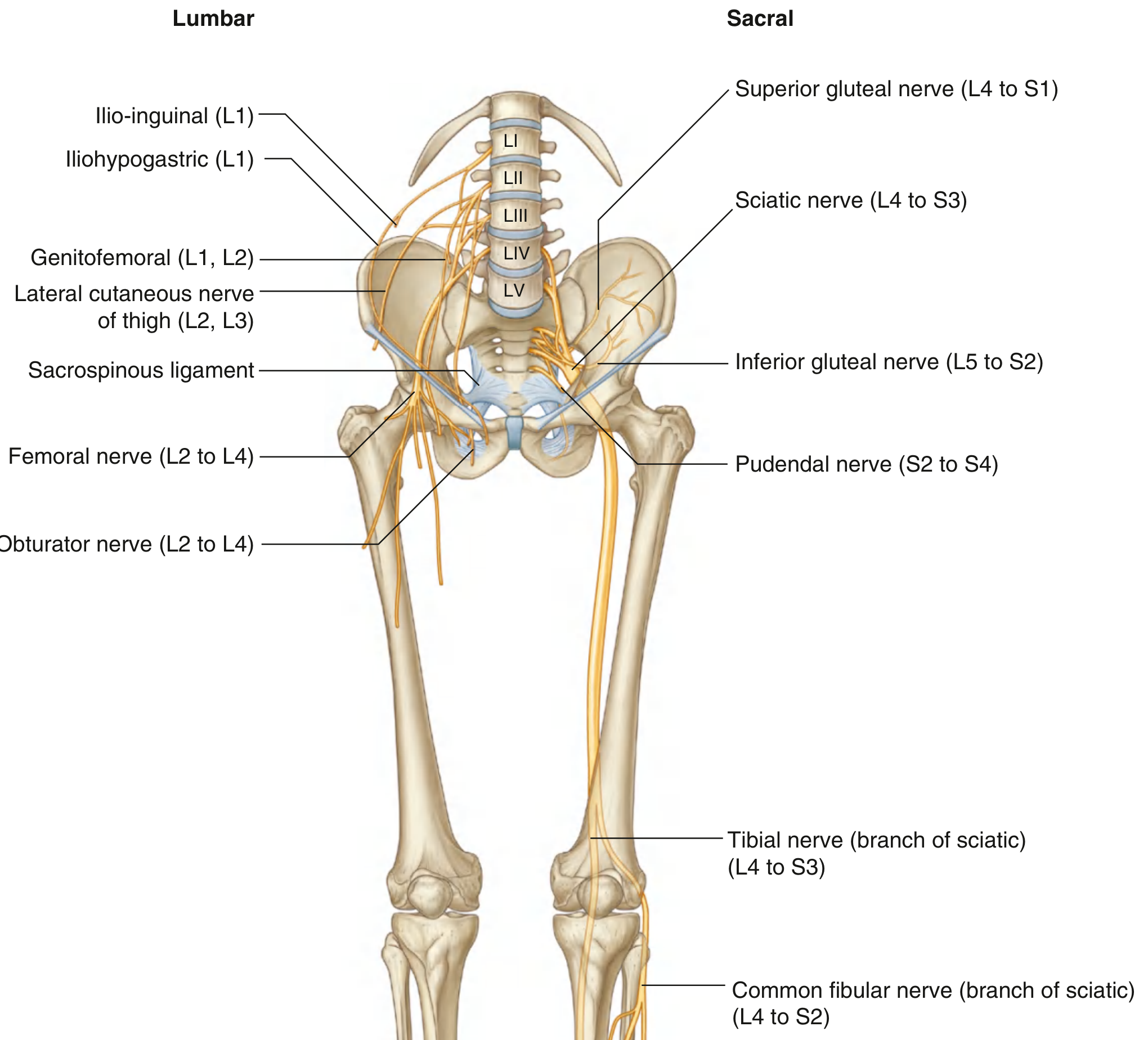
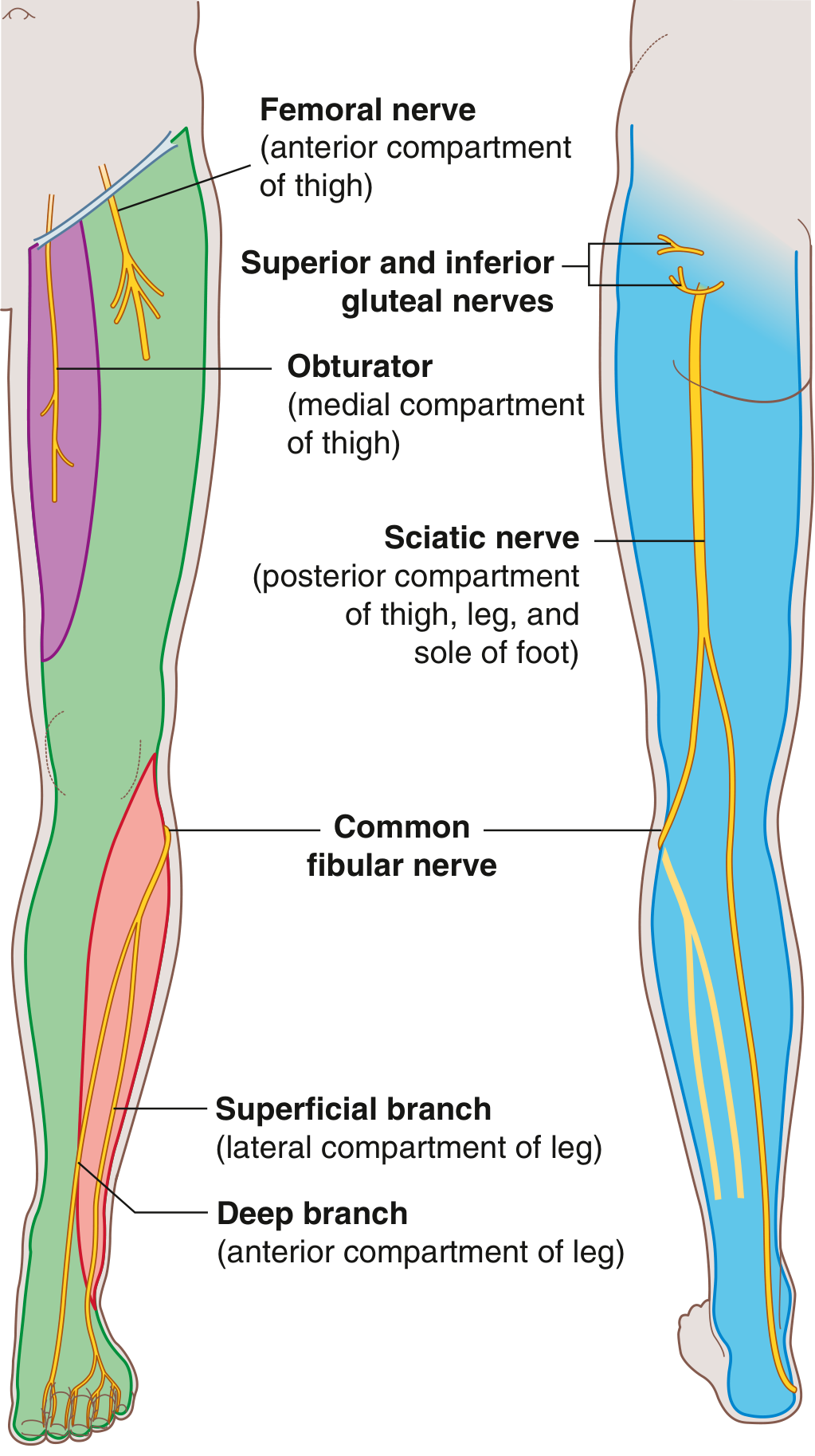
Major Nerves and Their Distributions
| Nerve | Roots | Motor Supply | Sensory Supply |
|---|---|---|---|
| Femoral nerve | L2-L4 | Anterior thigh (quadriceps, sartorius, iliacus) | Anterior thigh, medial leg and ankle (via saphenous nerve) |
| Obturator nerve | L2-L4 | Medial thigh (adductors) | Medial thigh |
| Superior gluteal nerve | L4-S1 | Gluteus medius, gluteus minimus, TFL | None |
| Inferior gluteal nerve | L5-S2 | Gluteus maximus | None |
| Sciatic nerve | L4-S3 | Posterior thigh, all of leg and foot (via tibial + common fibular) | Via branches below |
| Tibial nerve (branch of sciatic) | L4-S3 | Posterior leg, sole of foot | Lateral ankle and foot, sole |
| Common fibular nerve (branch of sciatic) | L4-S2 | Anterior and lateral leg, dorsum of foot | Lateral leg and dorsum of foot |
| Lateral cutaneous nerve of thigh | L2-L3 | None | Lateral thigh only |
The common fibular nerve is particularly vulnerable as it winds around the neck of the fibula - a fracture there, or pressure from a tight cast, causes foot drop (inability to dorsiflex).
Dermatomes - Key Test Points
| Landmark | Spinal Level |
|---|---|
| Over inguinal ligament | L1 |
| Lateral thigh | L2 |
| Lower medial thigh | L3 |
| Medial great toe (digit I) | L4 |
| Medial side of digit II | L5 |
| Little toe (digit V) | S1 |
| Back of thigh | S2 |
| Skin over gluteal fold | S3 |
Myotomes & Reflexes
| Movement | Level | Reflex Tested |
|---|---|---|
| Hip flexion | L1-L2 | - |
| Knee extension | L3-L4 | Patellar reflex (L3-L4) |
| Knee flexion | L5-S2 | - |
| Ankle dorsiflexion | L4-L5 | - |
| Ankle plantarflexion | S1-S2 | Achilles reflex (S1-S2) |
Part 5: Blood Supply
5.1 Arteries
The main arterial supply enters the thigh as the femoral artery (continuation of the external iliac artery after it passes under the inguinal ligament).
Key arterial pathway:
Aorta → Common iliac → External iliac → Femoral artery (in femoral triangle)
→ Deep femoral artery (profunda femoris) → perforating arteries to thigh
→ Popliteal artery (posterior to knee)
→ Anterior tibial artery → Dorsalis pedis artery (dorsum of foot)
→ Posterior tibial artery → Medial and lateral plantar arteries (sole)
→ Fibular (peroneal) artery
Additional supply:
- Superior and inferior gluteal arteries (from internal iliac) - supply the gluteal region
- Obturator artery (from internal iliac, through obturator canal) - supplies medial thigh
- A rich anastomotic network around the hip (formed by circumflex femoral, gluteal, and obturator arteries) provides collateral circulation when one vessel is blocked
5.2 Veins
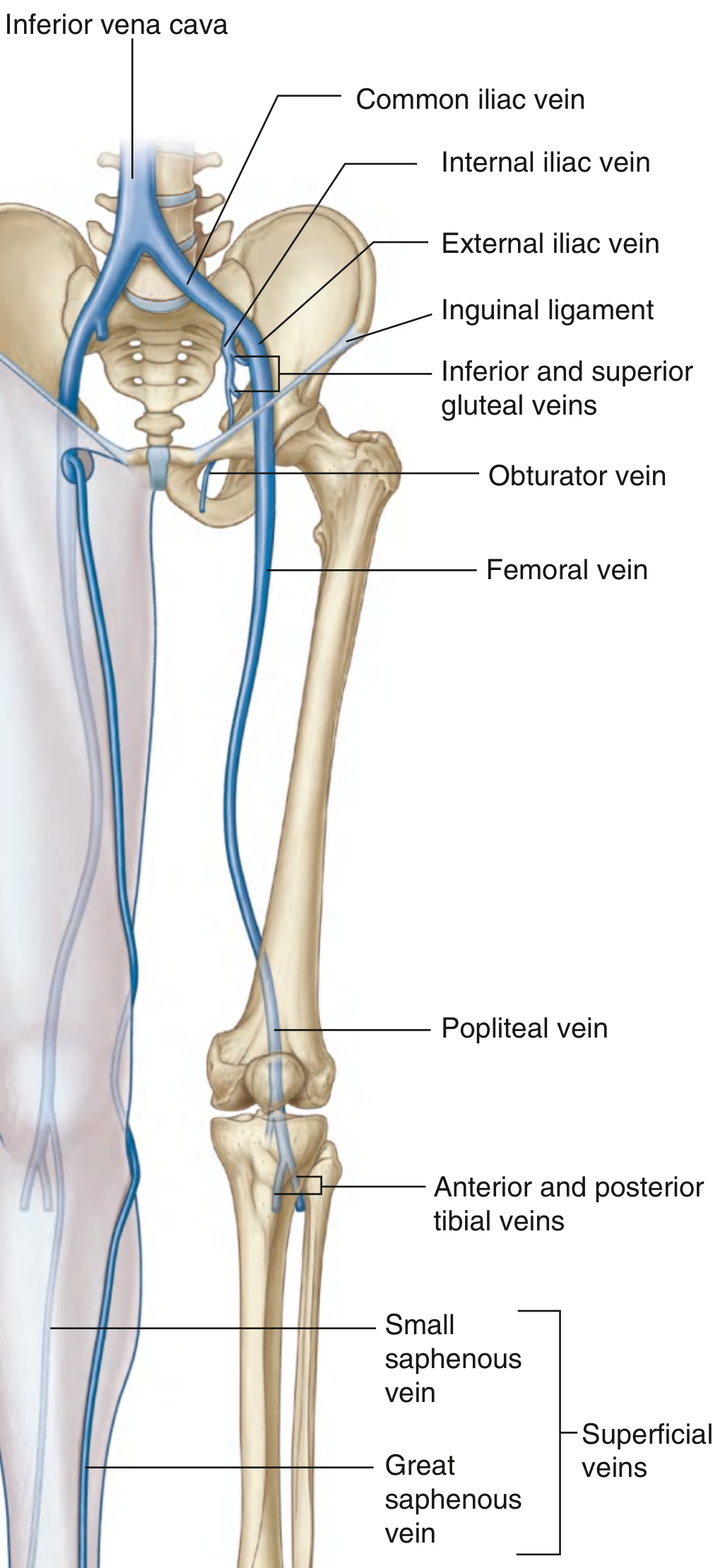
Deep veins follow the arteries (femoral, popliteal, tibial veins). The femoral vein is the main deep drainage vessel; it becomes the external iliac vein above the inguinal ligament.
Superficial veins (in subcutaneous tissue):
- Great (long) saphenous vein - originates from the medial dorsal venous arch, ascends the medial leg, knee, and thigh, drains into the femoral vein just below the inguinal ligament (at the saphenofemoral junction). Longest vein in the body; used for coronary artery bypass grafts
- Small (short) saphenous vein - originates from the lateral dorsal venous arch, ascends the posterior leg, penetrates deep fascia and drains into the popliteal vein behind the knee
Varicose veins occur when venous valves become incompetent, causing reflux and dilation of the superficial veins, typically in the great saphenous system.
Part 6: Function & Gait
Body Weight Support
The center of gravity in standing is anterior to the S2 vertebra. The vertical line through it passes:
- Slightly posterior to the hip joints (so the hip is passively extended - no muscle needed)
- Anterior to the knee and ankle joints (so these are passively stabilized in extension)
- This arrangement allows standing with minimal energy expenditure
Determinants of Gait
To reduce the vertical oscillation of the body's center of gravity during walking, the lower limb uses several strategies:
- Pelvic rotation - reduces stride length drop
- Pelvic tilt - the non-stance hip drops slightly (requires active gluteus medius on stance side)
- Knee flexion in the stance phase
- Foot and ankle mechanics - heel strike, then plantarflexion at toe-off
Part 7: Clinical Correlates Summary
| Condition | Anatomy Involved | Key Point |
|---|---|---|
| Femoral neck fracture | Medial/lateral circumflex femoral arteries | Risk of avascular necrosis of femoral head |
| Trendelenburg sign | Gluteus medius (superior gluteal nerve) | Pelvis drops on unaffected side during single-leg stance |
| Foot drop | Common fibular nerve at neck of fibula | Loss of dorsiflexion |
| ACL tear | Anterior cruciate ligament | Positive anterior drawer / Lachman test |
| Unhappy triad | ACL + MCL + medial meniscus | Valgus force with rotation |
| Varicose veins | Great/small saphenous veins | Incompetent venous valves |
| DVT | Deep leg veins (popliteal, femoral) | Risk: immobility, Virchow's triad |
| Ankle sprain | Lateral ligaments (ATFL most common) | Inversion injury |
| Meralgia paresthetica | Lateral cutaneous nerve of thigh | Compression at ASIS; burning/tingling lateral thigh |
All content sourced from Gray's Anatomy for Students (Gray's Anatomy for Students, 9780323934237)
This is a shared conversation. Sign in to Orris to start your own chat.