Explain me 10 common heart diseases with ECG changes and ECG images of these diseases
Reading File
Finding Sources
Searching Images
ECG changes myocardial infarction ST elevation
Finding Sources
Searching Images
atrial fibrillation ECG rhythm strip
Searching Images
complete heart block third degree AV block ECG
Searching Images
left bundle branch block LBBB ECG 12 lead
Searching Images
hypertrophic cardiomyopathy ECG left ventricular hypertrophy
Searching Images
Wolff-Parkinson-White syndrome delta wave ECG pre-excitation
Searching Images
ventricular tachycardia ECG wide complex tachycardia
Searching Images
pericarditis ECG saddle shaped ST elevation diffuse
Searching Images
long QT syndrome Torsades de Pointes ECG
Searching Images
right bundle branch block RBBB ECG RSR pattern V1
Here is a comprehensive guide to 10 common heart diseases with their ECG changes and images:
10 Common Heart Diseases: ECG Changes & Images
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
Disease Overview: STEMI is caused by complete occlusion of a coronary artery (most commonly the LAD), leading to full-thickness myocardial necrosis if untreated.
Key ECG Changes:
| Feature | Description |
|---|---|
| ST Elevation | Convex ("tombstone") ST elevation ≥1 mm in ≥2 contiguous leads |
| Hyperacute T-waves | Tall, peaked T-waves in early phase |
| Reciprocal ST Depression | In opposite leads (e.g., inferior depression in anterior STEMI) |
| Q-waves | Pathological Q-waves develop after several hours (>40 ms wide or >25% of R-wave height) |
| T-wave Inversion | Evolves in the days following infarction |
Lead Localization:
- Anterior STEMI (LAD): V1–V4 elevation, reciprocal depression in II, III, aVF
- Inferior STEMI (RCA): II, III, aVF elevation, reciprocal depression in I, aVL
- Lateral STEMI (LCx): I, aVL, V5–V6 elevation
ECG Image — Anterior STEMI (LAD Occlusion):

ECG Image — Inferior-Posterior STEMI (RCA/LCx Occlusion):
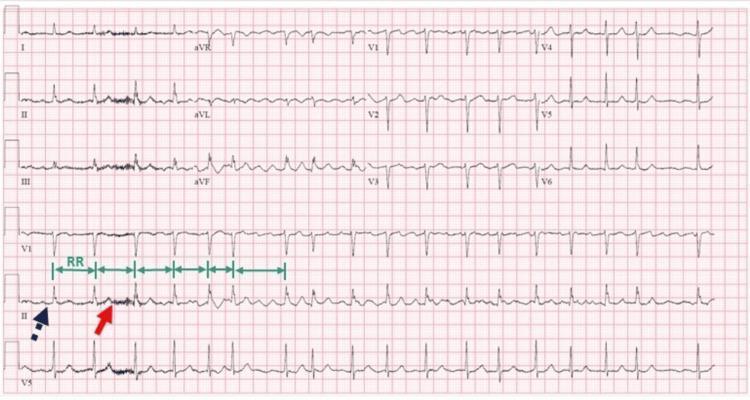
2. 🫀 Atrial Fibrillation (AF)
Disease Overview: AF is the most common sustained cardiac arrhythmia, characterized by chaotic, disorganized atrial electrical activity. It is associated with stroke, heart failure, and systemic thromboembolism.
Key ECG Changes:
| Feature | Description |
|---|---|
| Absent P-waves | No discrete organized P-waves; replaced by fibrillatory (f) waves |
| Irregular Baseline | Low-amplitude fibrillatory waves, best seen in V1 and II |
| Irregularly Irregular R-R | Variable ventricular rate; hallmark finding |
| Narrow QRS | Usually narrow (unless aberrant conduction or BBB present) |
ECG Image — Atrial Fibrillation with Absent P-waves and Irregular RR Intervals:
3. 🫀 Complete (Third-Degree) AV Block
Disease Overview: Complete failure of conduction between the atria and ventricles. Atria and ventricles beat independently. Can be caused by inferior MI, Lyme disease, drug toxicity, or degenerative disease (Lenègre's).
Key ECG Changes:
| Feature | Description |
|---|---|
| AV Dissociation | P-waves and QRS complexes bear NO consistent relationship |
| Regular P-P intervals | Atrial rate faster than ventricular rate |
| Regular R-R intervals | Ventricular escape rhythm is regular but slow |
| Wide QRS | If escape is ventricular origin (infra-Hisian) — QRS >120 ms |
| Narrow QRS | If junctional escape (supra-Hisian) — QRS <120 ms |
| Bradycardia | Ventricular rate typically 20–45 bpm |
ECG Image — Complete AV Block (Third-Degree Heart Block):
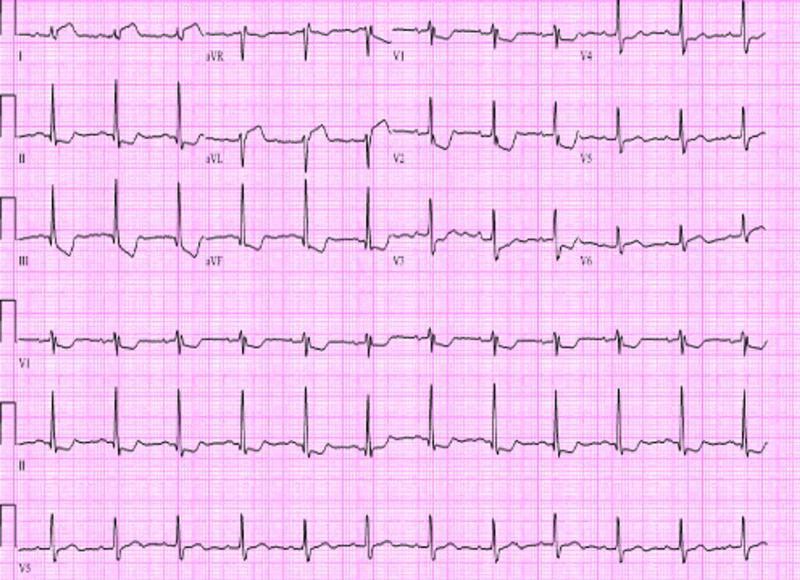
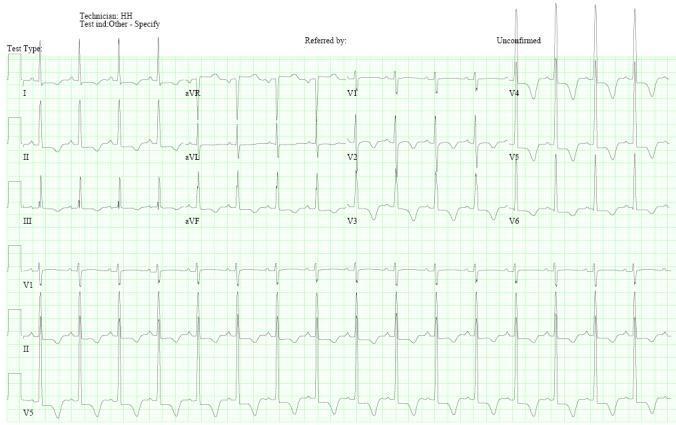
4. 🫀 Left Bundle Branch Block (LBBB)
Disease Overview: LBBB occurs when conduction through the left bundle branch is impaired, causing delayed left ventricular activation. New LBBB can indicate acute MI (Sgarbossa criteria), cardiomyopathy, or hypertension.
Key ECG Changes:
| Feature | Description |
|---|---|
| Wide QRS | ≥120 ms (complete LBBB) |
| Broad Notched R-waves | "M-shaped" broad R in lateral leads (I, aVL, V5, V6) |
| Deep S-waves (QS pattern) | In right precordial leads V1–V3 |
| Discordant ST-T Changes | ST and T-waves opposite in direction to QRS (secondary repolarization) |
| Left Axis Deviation | Common |
| Absent Septal Q-waves | In lateral leads |
ECG Image — LBBB with Broad Notched R-waves Laterally and Deep S-waves V1-V3:
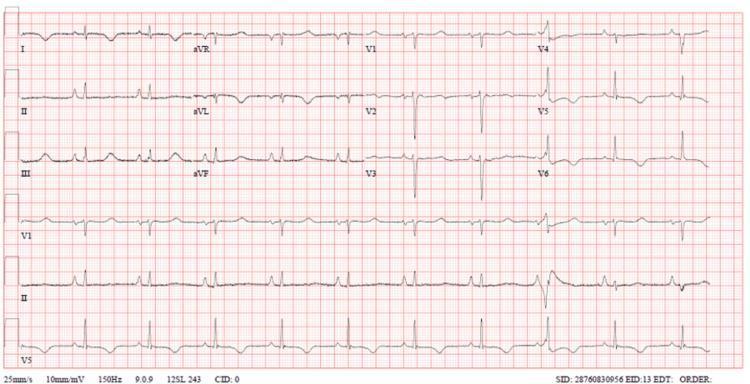
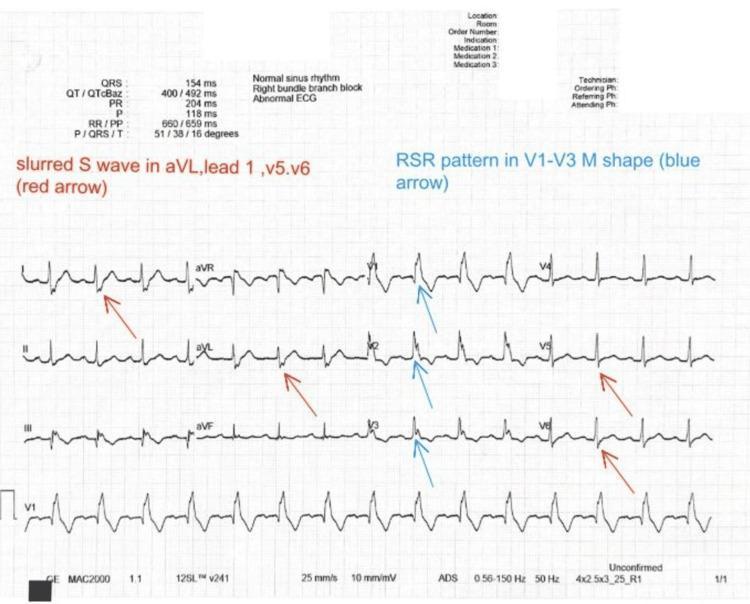
5. 🫀 Right Bundle Branch Block (RBBB)
Disease Overview: RBBB results from conduction delay in the right bundle branch. Can be seen in normal individuals, pulmonary embolism, right ventricular strain, congenital heart disease, or post-cardiac surgery.
Key ECG Changes:
| Feature | Description |
|---|---|
| Wide QRS | ≥120 ms (complete RBBB) |
| RSR' Pattern ("Rabbit Ears") | Classic rSR' or RSR' in V1–V3 — "M-shaped" in right precordials |
| Slurred S-wave | Broad, slurred S-wave in lateral leads (I, aVL, V5, V6) |
| T-wave Inversion | Secondary T-wave inversion in V1–V3 |
| Normal QRS Axis | Usually normal (unless associated hemiblock) |
ECG Image — RBBB with rSR' Pattern in V1 and Slurred S-waves Laterally:
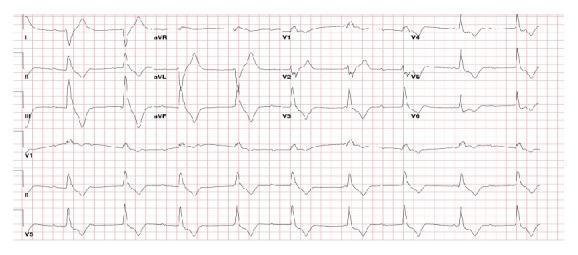
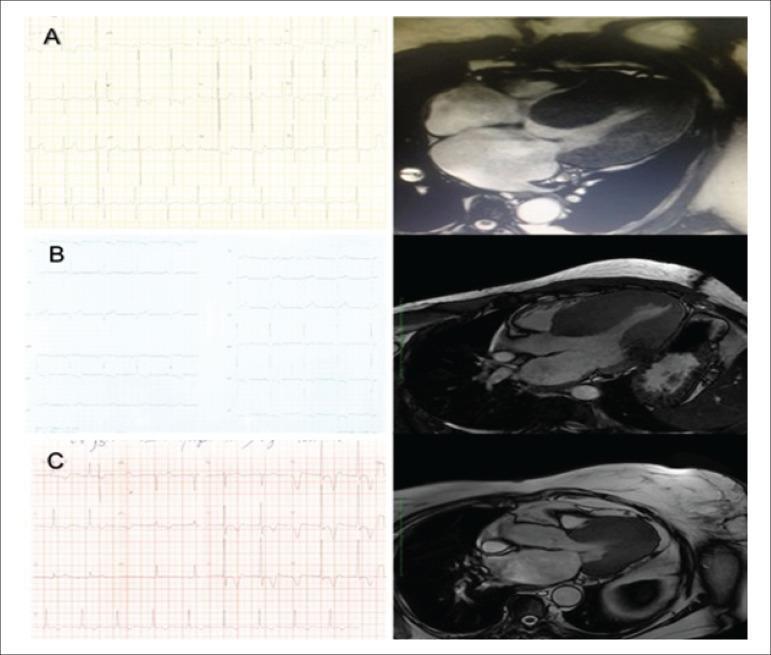
6. 🫀 Hypertrophic Cardiomyopathy (HCM)
Disease Overview: HCM is characterized by asymmetric septal hypertrophy (usually), diastolic dysfunction, and risk of sudden cardiac death. It is the most common cause of sudden cardiac death in young athletes.
Key ECG Changes:
| Feature | Description |
|---|---|
| LVH Voltage Criteria | Sokolow-Lyon: S(V1) + R(V5/V6) ≥35 mm |
| Deep Narrow Q-waves | Septal Q-waves in I, aVL, V5, V6 (pseudo-infarct pattern) |
| Strain Pattern | ST depression + T-wave inversion in lateral leads |
| Giant T-wave Inversions | Hallmark of apical HCM (Yamaguchi syndrome) — deep symmetric T inversions V2–V5 |
| Left Axis Deviation | Frequent |
| AF | Common complication in established HCM |
ECG Image — Apical HCM with Giant T-wave Inversions (Yamaguchi Syndrome):
ECG Image — HCM Comparison (Concentric, Septal, Apical) with CMR Correlation:
7. 🫀 Wolff-Parkinson-White (WPW) Syndrome
Disease Overview: WPW is a pre-excitation syndrome due to an accessory pathway (Bundle of Kent) between atria and ventricles, bypassing the AV node. Associated with SVT and potentially fatal rapid conduction during AF.
Key ECG Changes:
| Feature | Description |
|---|---|
| Short PR Interval | <120 ms — AV node bypassed |
| Delta Wave | Slurred upstroke at the start of QRS (slow accessory pathway conduction) |
| Wide QRS | >120 ms due to delta wave + normal conduction fusion |
| Discordant ST-T Changes | Secondary repolarization abnormalities opposite to QRS |
| Pseudo-infarct Q-waves | Negative delta waves in inferior/lateral leads can mimic Q-waves |
Accessory Pathway Localization (simplified):
- Delta positive V1 → Left lateral pathway
- Delta negative inferior leads (II, III, aVF) → Posteroseptal pathway
ECG Image — WPW with Short PR, Delta Waves, and Wide QRS:

8. 🫀 Acute Pericarditis
Disease Overview: Inflammation of the pericardium, most commonly viral in origin (Coxsackie, EBV). Presents with sharp positional chest pain, pericardial friction rub, and characteristic ECG evolution.
Key ECG Changes — 4 Stages:
| Stage | Timing | ECG Finding |
|---|---|---|
| Stage 1 | Days 1–2 | Diffuse concave ("saddle-shaped") ST elevation in all leads except aVR and V1 |
| Stage 1 | Days 1–2 | PR-segment depression in most leads; PR elevation in aVR |
| Stage 2 | Days 3–7 | ST returns to baseline; T-waves flatten |
| Stage 3 | 1–3 weeks | Diffuse T-wave inversions |
| Stage 4 | Weeks | Normalization |
Key differentiator from STEMI: Pericarditis ST elevation is diffuse (not in one coronary territory), concave (not convex), and accompanied by PR depression.
ECG Image — Acute Pericarditis with Diffuse Saddle-shaped ST Elevation and PR Depression:

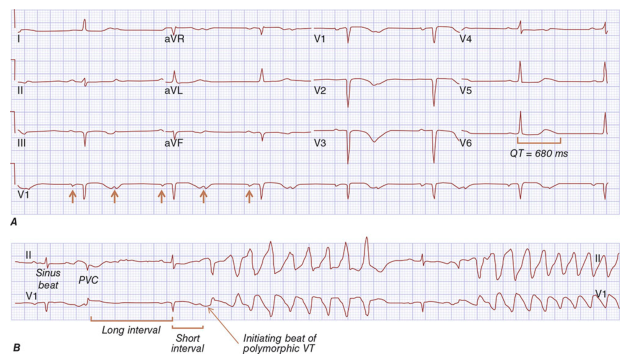
9. 🫀 Long QT Syndrome (LQTS) / Torsades de Pointes
Disease Overview: LQTS is characterized by delayed ventricular repolarization, predisposing to the lethal polymorphic VT called Torsades de Pointes. Can be congenital (channelopathy — LQT1, LQT2, LQT3) or acquired (drugs, hypokalemia, hypomagnesemia).
Key ECG Changes:
| Feature | Description |
|---|---|
| Prolonged QTc | QTc ≥450 ms (men), ≥470 ms (women); dangerous ≥500 ms |
| Abnormal T-wave Morphology | Notched, bifid, or biphasic T-waves (LQT2 especially) |
| U-waves | Prominent U-waves in LQT1 |
| T-wave Alternans | Beat-to-beat T-wave variation — marker of electrical instability |
| Torsades de Pointes | Polymorphic VT "twisting around the isoelectric line," initiated by R-on-T PVC |
ECG Image — Long QT Syndrome with Prolonged QTc and Torsades de Pointes Initiation:
10. 🫀 Ventricular Tachycardia (VT)
Disease Overview: VT is a life-threatening arrhythmia arising from ventricular myocardium or Purkinje fibers (rate ≥100 bpm, ≥3 consecutive beats). Most commonly associated with ischemic heart disease, dilated cardiomyopathy, or channelopathies.
Key ECG Changes:
| Feature | Description |
|---|---|
| Wide QRS Tachycardia | QRS ≥120 ms at rate >100 bpm |
| AV Dissociation | P-waves march independently of QRS — most specific for VT |
| Fusion Beats | Sinus impulse partially activates ventricles alongside VT beat |
| Capture Beats | Narrow QRS amidst wide-complex VT — pathognomonic for VT |
| Concordance | All precordial QRS deflections pointing same direction (positive or negative) — strongly suggests VT |
| Northwest Axis | Negative QRS in I and aVF — extreme axis deviation |
| Brugada Criteria | Help differentiate VT from SVT with aberrancy |
ECG Image — Monomorphic Ventricular Tachycardia with Wide QRS:

Quick Reference Summary Table
| # | Disease | Key ECG Finding |
|---|---|---|
| 1 | STEMI | Convex ST elevation in contiguous leads + reciprocal depression + Q-waves |
| 2 | Atrial Fibrillation | Absent P-waves, irregularly irregular R-R, fibrillatory baseline |
| 3 | Complete AV Block | AV dissociation — P & QRS independent, slow escape rhythm |
| 4 | LBBB | Wide QRS, broad notched R laterally, QS in V1–V3, discordant ST-T |
| 5 | RBBB | Wide QRS, rSR' in V1, slurred S in I/V6 |
| 6 | Hypertrophic CM | LVH voltage, septal Q-waves, strain pattern, giant T-inversions (apical) |
| 7 | WPW Syndrome | Short PR, delta wave, wide QRS |
| 8 | Acute Pericarditis | Diffuse concave ST elevation (all leads), PR depression, no reciprocal changes |
| 9 | Long QT / TdP | Prolonged QTc ≥500 ms, abnormal T-waves, Torsades de Pointes |
| 10 | Ventricular Tachycardia | Wide QRS tachycardia, AV dissociation, fusion/capture beats, concordance |
Clinical Pearl: Always compare any new ECG to a prior tracing when available — dynamic changes (e.g., new LBBB, evolving ST elevation) carry more clinical urgency than chronic findings.
This is a shared conversation. Sign in to Orris to start your own chat.