Varicose vein
Reading File
Finding Sources
Searching PubMed
"varicose veins"[MeSH Terms] AND treatment
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Here is a complete, well-structured answer on varicose veins:
Varicose Veins
Definition
Varicose veins are tortuous, dilated, elongated subcutaneous veins resulting from sustained venous hypertension and valvular incompetence, predominantly affecting the superficial venous system of the lower limbs. They are distinguished from telangiectasia (thread veins) and reticular veins, which are smaller and more superficial.
Clinical Photograph
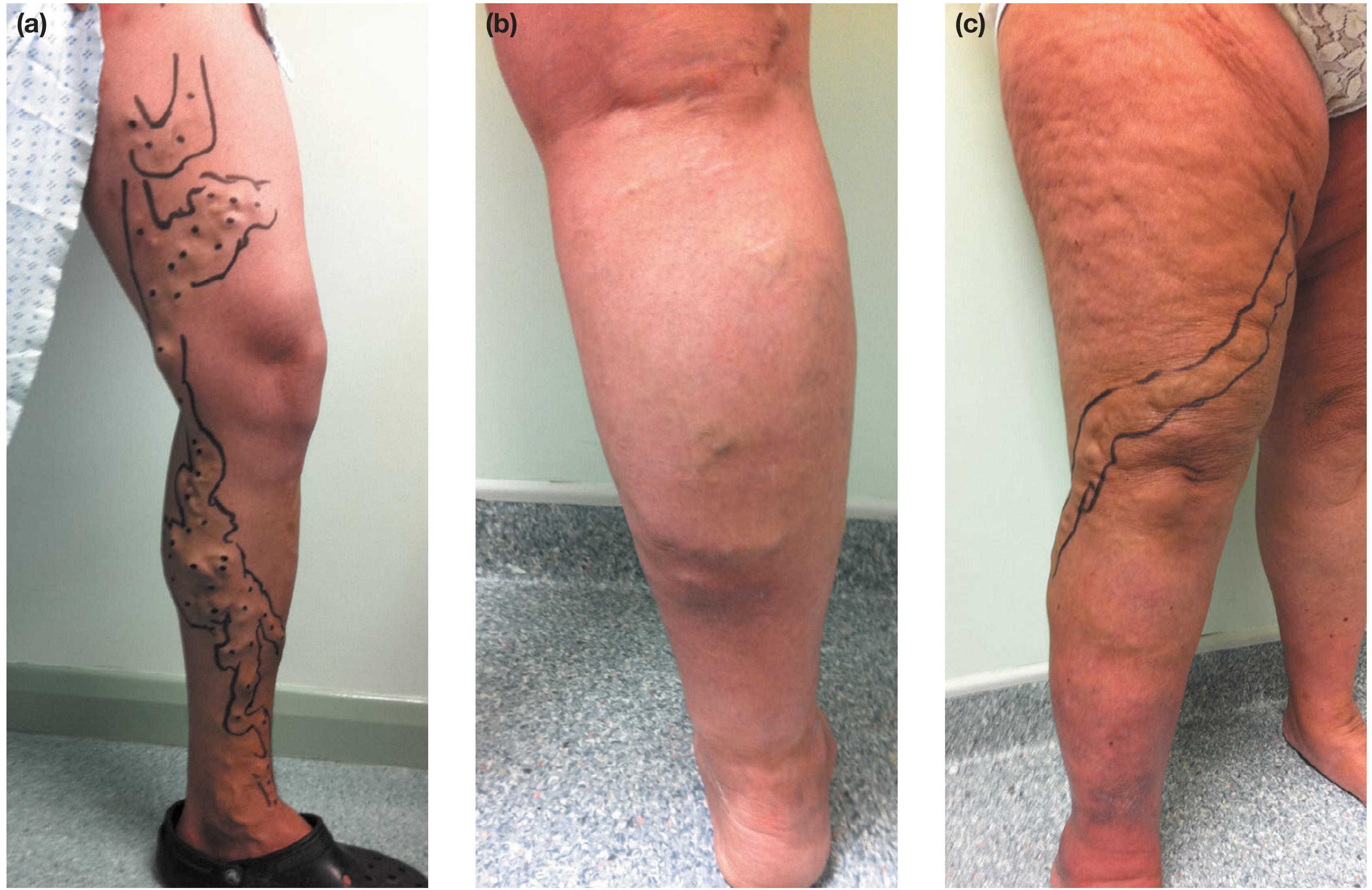
Figure: (a) Left leg GSV varicosities marked for intervention; (b) Right leg SSV distribution with recent phlebitis; (c) Anterolateral AAGSV distribution with gaiter area skin changes - Bailey & Love, p.1049
Epidemiology
- Adult prevalence: 30-50% of the general population
- More common in women than men
- Prevalence increases with age - from 11.5% (age 18-24) to 55.7% (age 55-64) per the Edinburgh Vein Study
- Risk factors: pregnancy, family history, increasing BMI and height, possibly prolonged standing
- Less common in primitive/rural communities (Africa, Far East)
Pathophysiology
The primary problem lies in the vein wall rather than mechanical valve failure alone. Vein wall changes include:
- Inflammatory cell infiltration and activation
- Dysfunctional smooth muscle cell proliferation
- Collagen deposition, decreased elastin content
- Increased matrix metalloproteinases
- Net result: loss of compliance → dilatation → elongation (tortuosity) → secondary valvular dysfunction
This creates retrograde flow with gravity (venous incompetence). Secondary varicosities can follow deep vein thrombosis (post-thrombotic) or occur with congenital arteriovenous fistulae.
Causes of predisposition:
- Primary: valvular incompetence, vein wall weakness
- Secondary: obstruction to venous return - pregnancy, pelvic tumours (fibroid, ovarian cyst, carcinoma cervix/rectum), ascites, abdominal lymphadenopathy, retroperitoneal fibrosis
- Congenital: arteriovenous fistula (in younger patients)
CEAP Classification
The CEAP (Clinical-Etiology-Anatomy-Pathophysiology) system is used internationally:
Clinical categories (C):
| Grade | Description |
|---|---|
| C0 | No visible or palpable signs of venous disease |
| C1 | Telangiectasia/reticular veins |
| C2 | Varicose veins |
| C3 | Oedema |
| C4a | Pigmentation/eczema |
| C4b | Lipodermatosclerosis/atrophie blanche |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
Anatomical (A): Superficial (As), Perforator (Ap), Deep (Ad)
Pathophysiological (P): Reflux (Pr), Obstruction (Po), Both (Pr,o)
Symptoms
Patients describe:
- Aching, heaviness, throbbing, burning, or bursting sensation in the legs
- Symptoms worsen throughout the day or with prolonged standing
- Relieved by elevation and compression hosiery
- Ankle swelling (especially by end of day)
- Pruritus (itching), especially with complications
- Night cramps
- Bursting pain on walking (suggests associated deep vein thrombosis)
Note: symptoms are independent of the degree of venous incompetence - asymptomatic varicosities can coexist with severe symptoms from minimal veins on the other side. - S. Das, p.105
Clinical Signs
Inspection:
- Tortuous dilated subcutaneous veins
- Distribution gives clue to axis involved:
- Medial thigh/calf → GSV incompetence
- Posterolateral calf → SSV incompetence
- Anterolateral thigh/calf → AAGSV incompetence
- Saphena varix: dilated vein at the SFJ appearing as a groin lump, disappears when recumbent (can mimic a femoral hernia - impulse on coughing)
- Skin changes: pigmentation, eczema, lipodermatosclerosis, venous ulcer (medial malleolus)
Key clinical tests:
| Test | Method | What it detects |
|---|---|---|
| Trendelenburg test | Tourniquet applied at SFJ after leg elevation; observe vein filling on standing | SFJ incompetence |
| Schwartz test (Percussion) | Tap prominent varicosity; impulse felt at saphenous opening | Continuous column of blood (incompetent valves) |
| Cough impulse (Morrissey) | Leg elevated, then patient coughs; expansile impulse at saphenous opening | SFJ valve incompetence |
| Fegan's method | Mark varicosity bulges; elevate limb; palpate for fascial gaps | Sites of incompetent perforators |
| Auscultation | Continuous machinery murmur | Arteriovenous fistula (secondary varicosities) |
Investigation
Duplex ultrasound is now the gold standard - tourniquet tests and hand-held Doppler have been abandoned. Duplex establishes:
- Presence and distribution of reflux in deep and superficial systems
- Anatomy of the SFJ and SPJ
- Presence of deep vein thrombosis or obstruction
- Location of incompetent perforators
A 7.5-13 MHz linear array transducer is standard. Blue = antegrade flow toward heart; red = reverse (reflux).
Treatment
Conservative
- Compression hosiery (first-line for symptom relief)
- Leg elevation, weight loss, exercise
- Useful as trial to confirm symptoms are venous before intervention
Interventional (current evidence)
1. Endovenous Thermal Ablation
- Endovenous Laser Ablation (EVLA): Laser fibre inserted under ultrasound guidance; perivenous tumescent anaesthesia used; energy delivered as fibre is withdrawn. Highest technical efficacy.
- Radiofrequency Ablation (RFA): Uses radiofrequency energy via catheter. Comparable efficacy to EVLA with possibly less post-procedural pain.
- A 2024 meta-analysis (Jiang et al., J Vasc Surg Venous Lymphat Disord, PMID 38316290) found RFA and EVLA have comparable clinical outcomes; RFA may have slight advantage in post-operative comfort.
2. Foam Sclerotherapy
- Sclerosant (e.g., sodium tetradecyl sulphate or polidocanol) mixed with air/gas to create foam
- Ultrasound-guided for truncal veins
- Can be used alongside thermal ablation for tributaries
3. Ambulatory Phlebectomy (Stab Avulsion)
- Micro-incisions (2-3 mm) to remove varicosities
- Often combined with truncal ablation in same sitting
4. Open Surgery (Trendelenburg + Stripping)
- Flush ligation of SFJ + stripping of GSV
- Now less commonly performed; reserved for recurrent disease, complex anatomy, or where endovenous techniques are unavailable
For recurrent varicose veins from the SFJ/GSV, a 2024 systematic review (Bontinis et al., Int Angiol, PMID 39559844) found endovenous techniques are effective for recurrence.
Complications
| Type | Examples |
|---|---|
| Chronic | Pigmentation, eczema, lipodermatosclerosis, atrophie blanche, venous ulcer |
| Acute | Superficial vein thrombosis (thrombophlebitis), haemorrhage (from rupture) |
| Post-operative | DVT, nerve injury (saphenous/sural nerve), wound haematoma, recurrence |
Differential Diagnosis of Varicose Veins (causes of dilated leg veins)
- Primary (idiopathic) varicose veins
- Secondary to DVT (post-thrombotic syndrome)
- Secondary to pelvic obstruction (pregnancy, tumour)
- Congenital AV fistula (Klippel-Trenaunay syndrome - port wine stain + limb hypertrophy + varicosities)
- May-Thurner syndrome (iliac vein compression)
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Edition, pp. 1047-1060
- S. Das: A Manual on Clinical Surgery, 13th Edition, pp. 105-109
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Edition
Venoux system of lower limb
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material with excellent diagrams. Here is the complete answer:
Venous System of the Lower Limb
The venous system of the lower limb is divided into three interconnected compartments: the deep venous system, the superficial venous system, and the perforating (communicating) veins that link them. Blood flows from superficial → deep → central circulation.
1. Overview
The venous system contains approximately 60% of total blood volume at a mean pressure of 5-10 mmHg. Return of blood from the lower limb to the right atrium depends on:
- Venous valves (preventing reflux)
- Calf muscle pump (augmenting flow during exercise)
- Respiratory/thoracic pressure changes
2. Deep Venous System
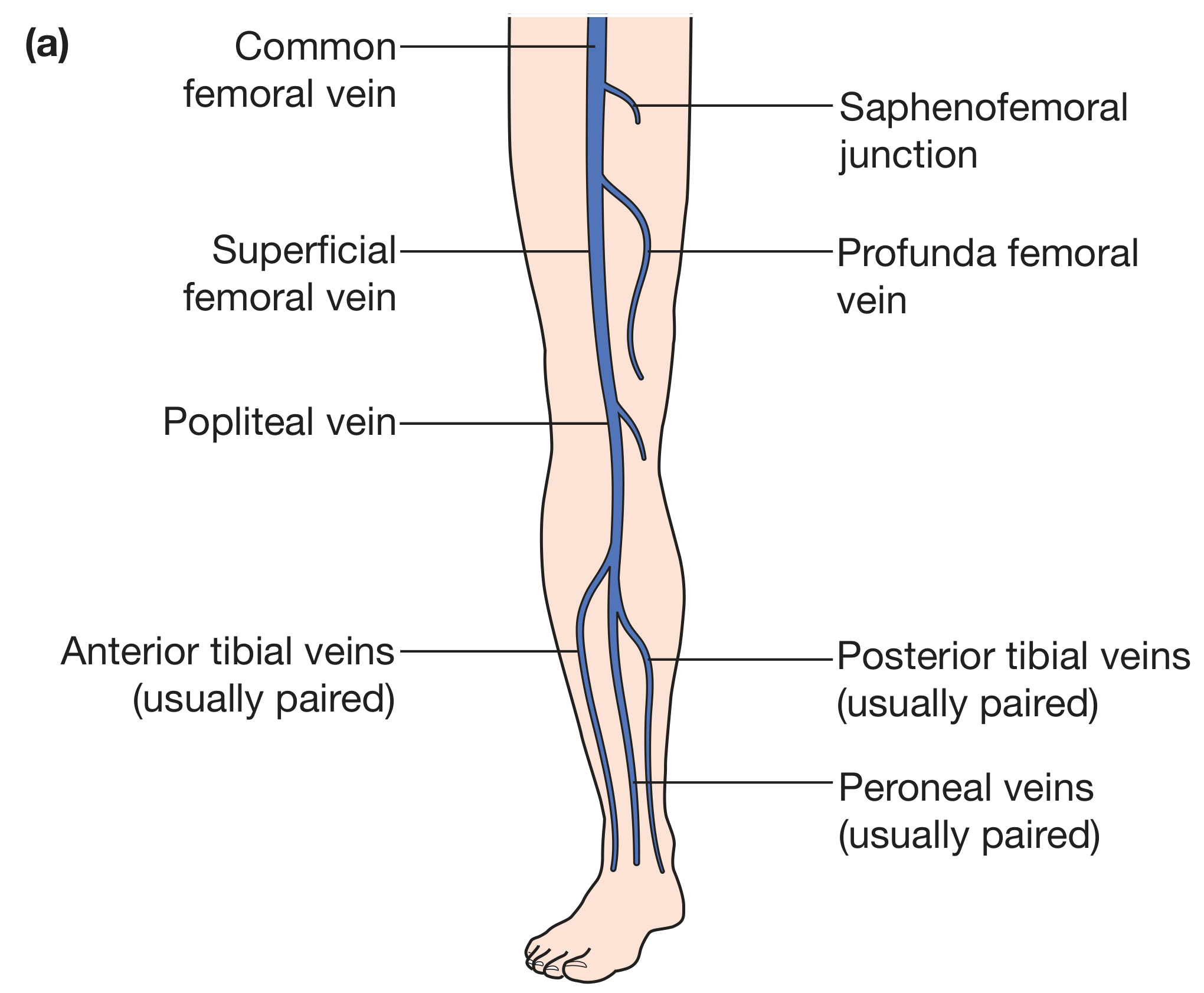
Figure: Anatomy of the deep veins of the lower limb - Bailey & Love, p.1047
The deep veins lie beneath the deep fascia and accompany the arterial tree:
Leg (Crural Veins)
Three pairs of venae comitantes (paired veins running alongside each artery):
- Anterior tibial veins (paired) - accompany anterior tibial artery
- Posterior tibial veins (paired) - accompany posterior tibial artery
- Peroneal (fibular) veins (paired) - accompany peroneal artery
These six veins intercommunicate freely and converge in the popliteal fossa.
They also receive the muscular veins of the calf:
- Soleal veins - drain the soleus muscle (form a sinus/plexus - a common site for DVT initiation)
- Gastrocnemius veins - drain both heads of gastrocnemius
Popliteal Fossa
All six crural veins + soleal + gastrocnemius veins join to form the popliteal vein.
Thigh
The popliteal vein passes through the adductor hiatus → enters the subsartorial canal as the femoral vein (previously called "superficial femoral vein" - a misnomer, it is a deep vein).
In the femoral triangle, it receives the profunda femoris (deep femoral) vein before passing behind the inguinal ligament to become the external iliac vein.
Pelvis and Abdomen
- External iliac vein + Internal iliac vein → Common iliac vein
- Left common iliac vein passes behind the right common iliac artery (clinically important - site of May-Thurner compression syndrome)
- Right and left common iliac veins join on the right side of the aorta → Inferior vena cava → Right atrium
3. Superficial Venous System
The superficial veins lie in the subcutaneous fat, superficial to the deep fascia (fascia lata) but deep to the saphenous fascia - within what is called the saphenous envelope. There are two main axes.
3A. Great Saphenous Vein (GSV)
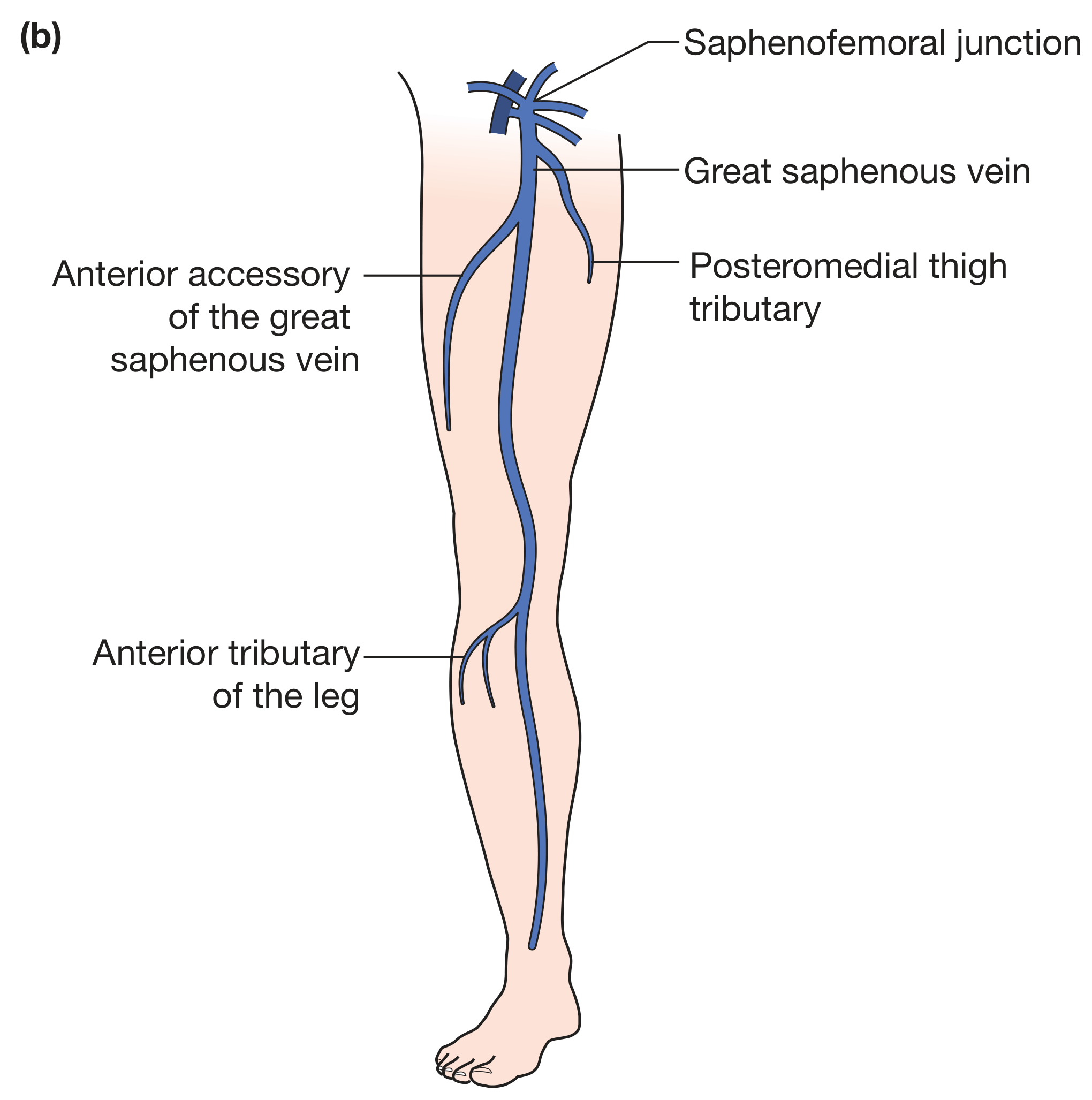
Figure: Great saphenous vein axis with AAGSV and tributaries - Bailey & Love, p.1047
| Feature | Detail |
|---|---|
| Origin | Medial side of the dorsal venous arch of the foot |
| Ankle | Passes anterior to the medial malleolus |
| Leg | Ascends medially with the saphenous nerve; medial to tibia |
| Knee | Loops posteriorly around the medial condyle of femur |
| Thigh | Continues in the medial thigh |
| Termination | Pierces the cribriform fascia at the saphenous opening (~2.5 cm below and lateral to the pubic tubercle) → drains into the common femoral vein at the saphenofemoral junction (SFJ) |
| Clinical significance | Longest vein in the body; most frequently affected by incompetence |
Tributaries at the SFJ (the "bouquet"):
- Superficial external pudendal vein
- Superficial circumflex iliac vein
- Superficial epigastric vein
- Anterior femoral cutaneous vein
- Posteromedial thigh tributary
- Anterolateral thigh tributary
Anterior Accessory of the Great Saphenous Vein (AAGSV):
- One of the most common tributaries
- Originates around the lateral border of the knee (sometimes from the lateral end of the dorsal venous arch)
- Courses anterolateral to the GSV
- Drains into the GSV at or near the SFJ
- Commonly mistaken for the GSV on duplex scan ("duplex GSV" - a true duplicated GSV is rare)
3B. Small Saphenous Vein (SSV)
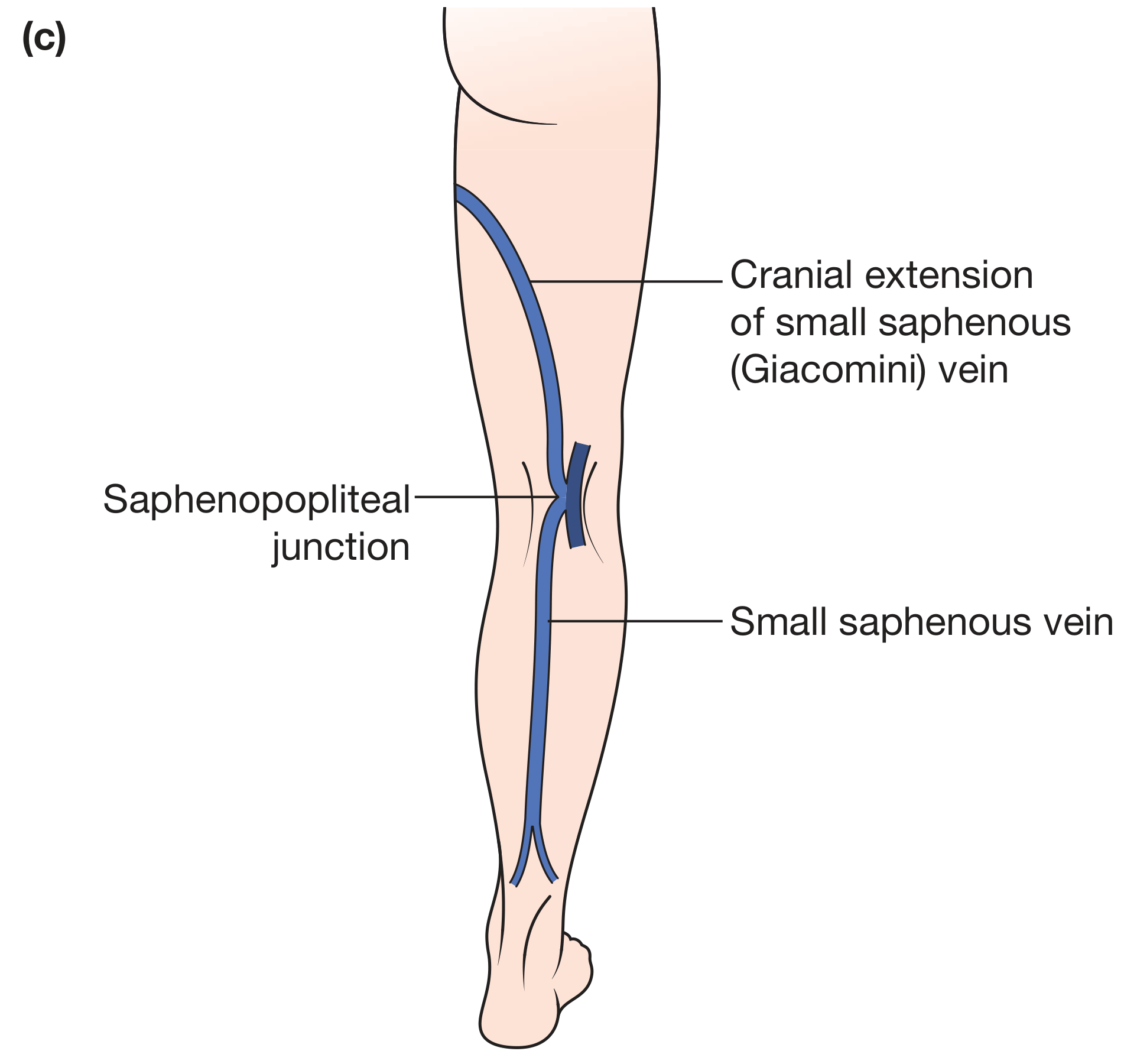
Figure: Small saphenous vein, saphenopopliteal junction, and Giacomini vein - Bailey & Love, p.1047
| Feature | Detail |
|---|---|
| Origin | Lateral side of the dorsal venous arch |
| Ankle | Posterior to the lateral malleolus (with the sural nerve) |
| Leg | Ascends in the posterior midline of the calf; sits in the groove between the two heads of gastrocnemius |
| Termination | Pierces the fascia of the popliteal fossa → drains into the popliteal vein at the saphenopopliteal junction (SPJ) - highly variable, may be as low as mid-calf |
| Extension | May continue cranially as the Giacomini vein - communicates with the GSV system, sometimes joining the GSV at/near the SFJ |
3C. Veins of the Foot
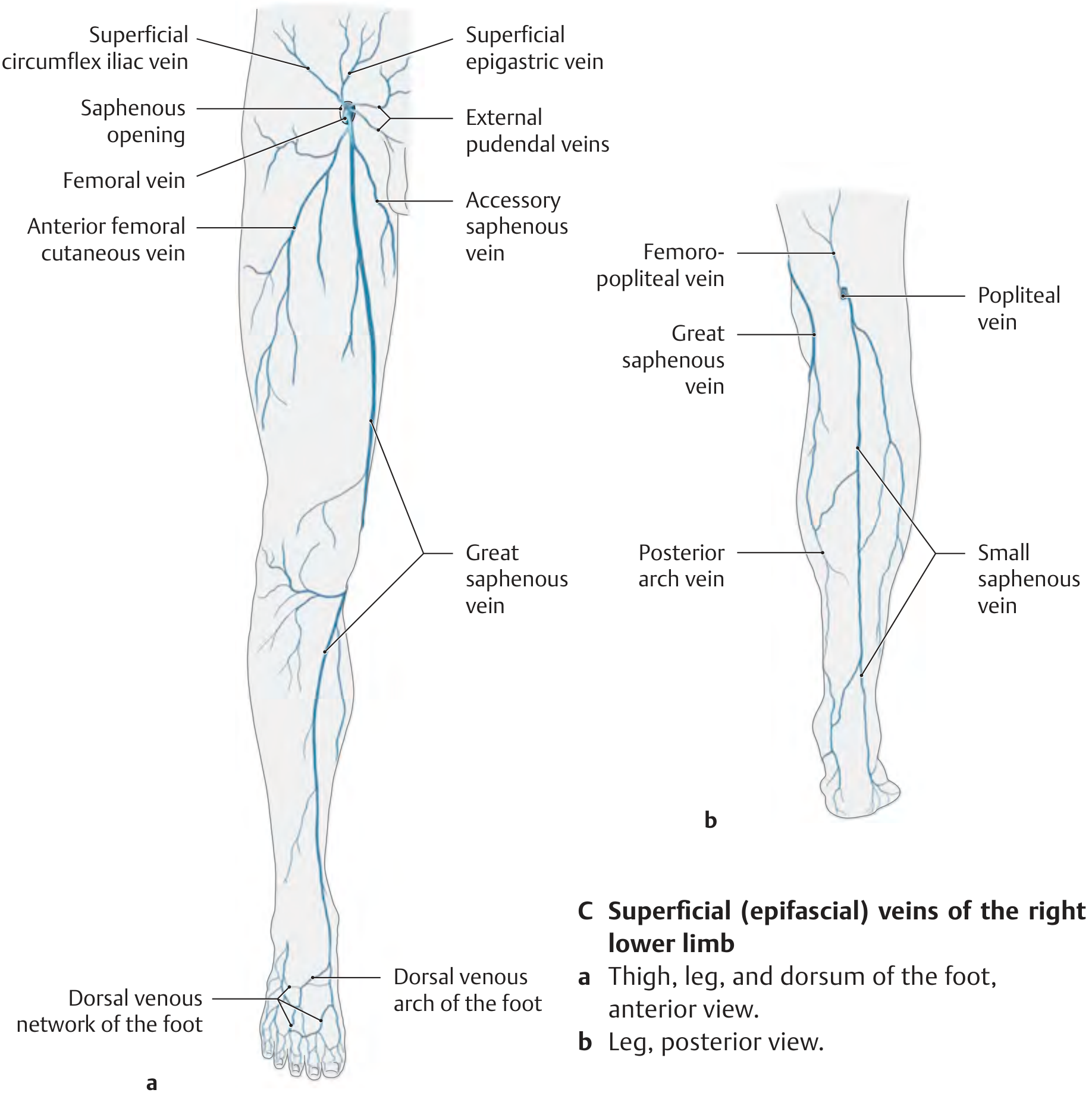
Figure: Superficial (epifascial) veins of the right lower limb - THIEME Atlas
| Structure | Location | Drains into |
|---|---|---|
| Dorsal venous arch | Over metatarsal heads | Medial end → GSV; lateral end → SSV |
| Medial marginal vein | Medial border of foot | GSV |
| Lateral marginal vein | Lateral border of foot | SSV |
| Dorsal venous network | Dorsum of foot | Dorsal arch, then GSV/SSV |
| Plantar venous arch | Plantar surface | Posterior tibial veins (deep) via plantar digital/metatarsal veins |
| Plantar venous network | Plantar surface | Plantar arch → posterior tibial veins |
| Posterior venous arch of foot | Dorsum, connects arches | Empties into SSV/GSV |
The dorsal and plantar arches are connected by intercapitular veins.
Because the sole bears significant weight and pressure, most venous drainage of the foot is via the dorsal venous arch rather than the plantar surface.
4. Perforating (Communicating) Veins
Perforating veins are valved vessels that pierce the deep fascia, connecting superficial to deep veins. Valves normally allow flow only from superficial → deep. When valves become incompetent, reversal of flow causes superficial hypertension and varicosities.

Figure: Deep and superficial veins with perforators, plantar and dorsal venous networks - Color Atlas of Human Anatomy
The three clinically important groups of perforators (THIEME Atlas, p.551):
| Group | Location | Clinical relevance |
|---|---|---|
| Dodd group | Medial thigh, middle third | Incompetence → medial thigh varicosities |
| Boyd group | Medial leg, just below knee | Common site of incompetence |
| Cockett group | Medial distal leg (ankle region) | Most important clinically; incompetence causes gaiter area pigmentation, lipodermatosclerosis, venous ulcers |
The Cockett perforators are located at approximately 7.5, 12.5, and 18.5 cm above the medial malleolus.
5. Venous Physiology - Calf Muscle Pump
At rest (standing), superficial venous pressure in the foot is ~80-90 mmHg (hydrostatic). During walking:
- Calf muscle contraction compresses the deep veins
- Valves direct flow upward (antegrade)
- Superficial pressure falls to ~25 mmHg
- On stopping exercise, pressure rises slowly back to resting level (refilling time)
In venous incompetence (valve failure), pressure does not fall adequately during exercise, producing venous hypertension - the root cause of all complications (oedema, skin changes, ulceration).
6. Summary: Flow Pathway
Foot veins (dorsal venous arch / plantar network)
↓
Great saphenous vein Small saphenous vein
(medial) (posterior)
↓ ↓
Saphenofemoral junction Saphenopopliteal junction
(common femoral vein) (popliteal vein)
↓
Femoral vein
↓
+ Profunda femoris vein
↓
External iliac vein
↓
Common iliac vein
↓
Inferior vena cava
↓
Right atrium
All along this pathway: perforating veins connect superficial → deep systems at the leg and thigh.
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Edition, pp. 1046-1049
- Gray's Anatomy for Students, p. 671
- THIEME Atlas of Anatomy: General Anatomy and Musculoskeletal System, p. 551
- Color Atlas of Human Anatomy, Vol. 2 (Internal Organs), pp. 144-146
This is a shared conversation. Sign in to Orris to start your own chat.