percutaneous tracheostomy in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
percutaneous tracheostomy techniques complications
Searching the Web
percutaneous tracheostomy RGUHS ENT 50 marks Scott Brown Cummings Dhingra
Finding Sources
Reading Article
PMID: 35573523
Reading Article
PMID: 39588741
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading Web Page
https://amj.amegroups.org/article/view/9449/html
Finding Sources
PERCUTANEOUS TRACHEOSTOMY
RGUHS ENT Long Essay - 50 Marks
1. INTRODUCTION AND HISTORICAL BACKGROUND
Tracheostomy is the creation of an opening in the anterior wall of the trachea to establish a definitive airway. The percutaneous route refers to a minimally invasive, bedside method of achieving this using needle puncture, guidewire placement, and sequential dilation - bypassing the need for formal surgical incision and dissection.
Historical milestones:
- 1955 - Shelden et al.: first percutaneous tracheostomy concept reported
- 1969 - Toye and Weinstein: first modern percutaneous technique
- 1985 - Pasquale Ciaglia: described elective percutaneous dilatational tracheostomy (PDT) using serial dilators over a J-wire - the landmark paper (Chest 1985;87:715-719)
- 1990 - Griggs: introduced guidewire dilating forceps (GWDF) technique
- 1997 - Fantoni: translaryngeal tracheostomy (TLT)
- 1999 - Ciaglia Blue Rhino: single-step conical dilator (now most widely used worldwide)
- 2002 - PercuTwist: single screw-type dilator technique
(Scott-Brown's Otorhinolaryngology, Vol. 2; Cummings Otolaryngology, 7th ed.)
2. ANATOMY RELEVANT TO PERCUTANEOUS TRACHEOSTOMY
ANTERIOR NECK - SURGICAL ANATOMY
┌────────────────────────────────────────────────────────┐
│ SKIN → Subcutaneous fat → Platysma │
│ → Investing fascia → Strap muscles (sternohyoid/ │
│ sternothyroid) → Pretracheal fascia → TRACHEA │
│ │
│ ← Thyroid gland (isthmus overlies rings 2-4) │
│ ← Cricothyroid arteries (above, avoid) │
│ ← Inferior thyroid arteries (lateral, avoid) │
│ ← Brachiocephalic artery (below, avoid) │
│ ← Cricoid cartilage (landmark - do NOT stab above) │
└────────────────────────────────────────────────────────┘
TARGET ZONE: Between 1st-2nd or 2nd-3rd tracheal rings
(cricotracheal membrane = NEVER - risk of subglottic stenosis)
Key landmarks palpated before puncture:
- Hyoid bone
- Thyroid cartilage (Adam's apple)
- Cricoid cartilage (ring-shaped)
- Cricothyroid membrane (NOT the target - above)
- 1st-4th tracheal rings (target: rings 1-2 or 2-3)
- Sternal notch (inferior limit)
(Cummings Otolaryngology Head and Neck Surgery, 7e; Gray's Anatomy for Students)
3. INDICATIONS
3A. Box: Indications for Tracheotomy (Cummings, Box 7.1)
| Category | Specific Indication |
|---|---|
| Prolonged mechanical ventilation | Respiratory disease, neuromuscular disease, depressed mental status |
| Pulmonary toilet | Inability to clear secretions independently |
| Surgical access | Head and neck cancer reconstruction, maxillofacial fractures |
| Airway obstruction | Epiglottitis, tumour, bilateral VCP, angioedema, foreign body, trauma |
Specific indications for PERCUTANEOUS route:
- ICU patient requiring mechanical ventilation > 7-10 days
- Bedside procedure preferred (avoids OR transfer risk)
- Elective setting with palpable, accessible anterior neck
- Patient intubated and ventilated with continuous monitoring
(Scott-Brown's; Cummings Box 7.1; Khaja et al., Cureus 2022)
4. CONTRAINDICATIONS
Absolute Contraindications:
- Emergency airway situation (prefer surgical tracheostomy or cricothyrotomy)
- Uncontrolled coagulopathy
- Non-palpable trachea (markedly obese neck, massive goitre)
- Age < 12-15 years (relative to absolute in children - anatomy too small)
Relative Contraindications:
- Morbid obesity (BMI > 40) - limited landmark palpation
- Short, fat neck
- Previous neck surgery/radiation
- Enlarged thyroid gland (goitre)
- High cervical lesion/instability (cannot extend neck)
- Severe coagulopathy (INR > 1.5, platelets < 50,000)
- Severe hypoxia requiring high FiO2 (brief apnea during procedure risky)
- Tracheal pathology (stenosis, malacia)
- Paediatric age group
(Scott-Brown's Otorhinolaryngology; Cummings; AME Medical Journal updated review 2023)
5. EQUIPMENT REQUIRED
Percutaneous Tracheostomy Kit (Ciaglia Blue Rhino - most commonly used):
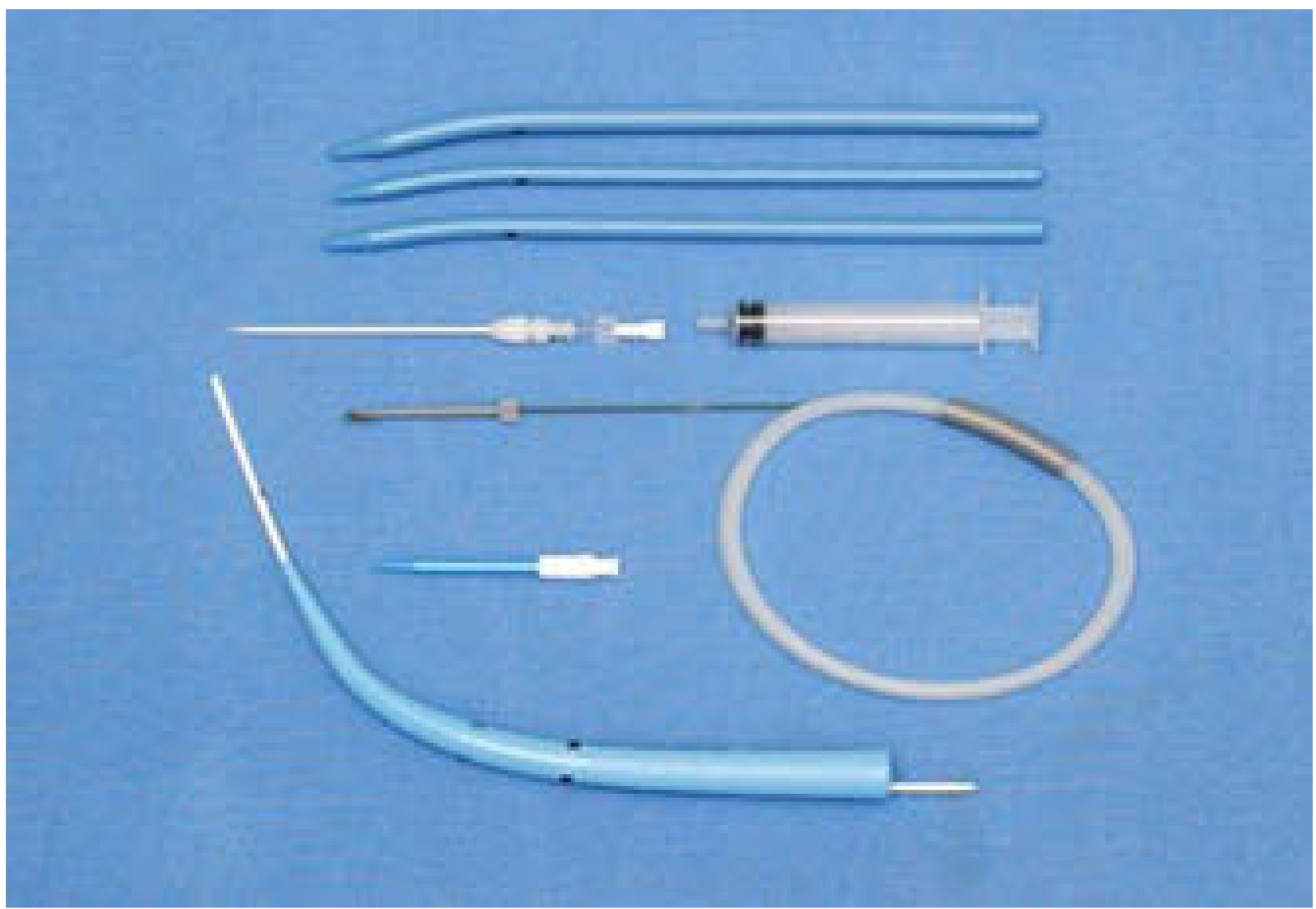
Components:
- Introducer needle (18-gauge, with plastic cannula)
- Saline-filled syringe (10 mL)
- J-tipped guidewire (Seldinger wire)
- 12-Fr guiding catheter (loading dilator)
- Hydrophilic-coated single conical dilator (Blue Rhino)
- Tracheostomy tube (cuffed, size 7 or 8 for adults)
- Sutures (0 prolene or silk for securing)
Additional requirements:
- Flexible fibroscope/bronchoscope (strongly recommended)
- Suction equipment, resuscitation trolley
- Monitoring: SpO2, ECG, BP, capnography
- Local anaesthetic: 1% lignocaine with 1:100,000 adrenaline
6. PRE-OPERATIVE ASSESSMENT AND PREPARATION
Assessment checklist:
- Confirm indication and obtain consent
- Assess neck anatomy: palpate landmarks
- Check coagulation: INR < 1.5, platelets > 50,000
- Review imaging: CT/USS neck if anatomy unclear
- Ensure patient is adequately ventilated (consider increasing FiO2 to 100% pre-procedure)
- Check current endotracheal tube position (ETT must be present for airway security)
- Anaesthetic team and/or intensivist presence mandatory
Positioning:
- Supine with shoulder roll/sandbag beneath shoulders
- Neck extended (unless cervical spine injury contraindicated)
- Head in neutral position on a ring
- Patient placed square on table (shoulders level)
(Cummings, Box 7.3; Scott-Brown's p. 1085-1086)
7. OPERATIVE TECHNIQUE - CIAGLIA BLUE RHINO (Step-by-Step)
FLOWCHART: Percutaneous Tracheostomy - Ciaglia Blue Rhino Method
╔══════════════════════════════════════════════════════════╗
║ PERCUTANEOUS TRACHEOSTOMY - FLOWCHART ║
╠══════════════════════════════════════════════════════════╣
║ STEP 1: PATIENT PREPARATION ║
║ • Supine, shoulder roll, neck extended ║
║ • FiO2 100%, SpO2/ECG/NIBP monitoring ║
║ • IV sedation + analgesia (propofol + fentanyl) ║
║ • Flexible bronchoscope inserted via ETT ║
║ • ETT withdrawn to level of vocal cords (under scope) ║
╠══════════════════════════════════════════════════════════╣
║ STEP 2: SITE PREPARATION ║
║ • Palpate thyroid, cricoid, tracheal rings ║
║ • Mark puncture site: below 1st ring or 2nd-3rd ring ║
║ • Infiltrate 1% lignocaine + adrenaline subcutaneously ║
║ • Prep and drape the surgical field ║
╠══════════════════════════════════════════════════════════╣
║ STEP 3: SKIN INCISION ║
║ • Horizontal 1.5-2 cm incision at planned site ║
║ • Blunt dissection with artery forceps in midline ║
║ • Through subcutaneous tissue to pretracheal fascia ║
╠══════════════════════════════════════════════════════════╣
║ STEP 4: TRACHEAL PUNCTURE (Seldinger Technique) ║
║ • 18G needle + cannula on saline-filled syringe ║
║ • Pass at 90° to tracheal wall (slight caudal angle) ║
║ • CONFIRM by: ║
║ - Aspiration of air through saline (bubbles) AND ║
║ - Bronchoscopic visualisation (see needle tip) ║
║ • Needle should be at 10-2 o'clock on anterior wall ║
║ • Withdraw needle, leave cannula in place ║
╠══════════════════════════════════════════════════════════╣
║ STEP 5: GUIDEWIRE INSERTION ║
║ • Pass J-tipped guidewire through cannula into trachea ║
║ • Wire directed inferiorly (into bronchial tree) ║
║ • Confirm position bronchoscopically ║
║ • Remove cannula, keep wire in situ ║
╠══════════════════════════════════════════════════════════╣
║ STEP 6: INITIAL DILATION ║
║ • Pass 12-Fr guiding catheter (loading dilator) over ║
║ guidewire into trachea ║
║ • This stiffens the wire and prevents kinking ║
╠══════════════════════════════════════════════════════════╣
║ STEP 7: BLUE RHINO DILATION (Single Conical Dilator) ║
║ • Load tracheostomy tube on conical Blue Rhino dilator ║
║ • Hydrate dilator with saline (reduces friction) ║
║ • Advance dilator + tube together over guiding catheter ║
║ • Rotate with GENTLE pressure - do NOT force ║
║ • Bronchoscope confirms passage through anterior wall ║
╠══════════════════════════════════════════════════════════╣
║ STEP 8: TRACHEOSTOMY TUBE INSERTION ║
║ • Advance tracheostomy tube into trachea ║
║ • Remove dilator, guiding catheter, and guidewire ║
║ • Inflate tracheostomy cuff with 5-10 mL air ║
║ • Attach ventilator circuit ║
╠══════════════════════════════════════════════════════════╣
║ STEP 9: CONFIRMATION AND SECURING ║
║ • Confirm position: CO2 on capnograph, bilateral breath ║
║ sounds, bronchoscope through tracheostomy tube ║
║ • Secure tube with sutures (0-prolene) to skin ║
║ • Apply tracheostomy collar/ties ║
║ • CXR post-procedure ║
║ • Dressing applied (split gauze under flange) ║
╚══════════════════════════════════════════════════════════╝
(Cummings Otolaryngology, Box 7.3; Scott-Brown's p. 1086-1087; Khaja et al., Cureus 2022)
8. TECHNIQUES / TYPES OF PERCUTANEOUS TRACHEOSTOMY
Comparison Table of All Techniques:
| Technique | Year | Method | Key Feature |
|---|---|---|---|
| Ciaglia Sequential Dilatation | 1985 | Serial dilators of increasing size over J-wire | Original, still used |
| Griggs GWDF | 1990 | Howard-Kelly forceps over guidewire dilates tract | Rapid, risk of posterior wall injury |
| Fantoni TLT | 1997 | Retrograde: wire from trachea out mouth, tube pulled in | Complex, rarely used |
| PercuTwist | 2002 | Screw-type dilator - clockwise rotation | Pulls tracheal wall anteriorly |
| Ciaglia Blue Rhino | 1999 | Single conical hydrophilic dilator | Now the gold standard worldwide |
| Balloon Dilation | 2005 | Balloon catheter dilates tract | Gentle, less mucosal trauma |
| Rigid Bronchoscope-guided | Modern | Real-time rigid endoscopic guidance | Best in difficult airways |
Why Blue Rhino is preferred (AME Medical Journal review; Cummings):
- Single step dilation vs. multiple dilators
- Hydrophilic coating reduces friction and mucosal trauma
- Lower complication rate in meta-analyses
- Faster procedure time
- Can be combined with bronchoscopic guidance
(Cummings - Alternative Percutaneous Techniques section; AME Medical Journal, Moore et al.)
9. TRACHEOSTOMY TUBES
Types:
| Feature | Option 1 | Option 2 |
|---|---|---|
| Cuff | Cuffed (ventilated patients) | Uncuffed (breathing independently) |
| Inner cannula | Single lumen | Double lumen (inner removable - easier cleaning) |
| Fenestration | Unfenestrated | Fenestrated (allows phonation with speaking valve) |
| Material | PVC/Portex | Silver metal (Negus - for long-term) |
| Size | Size 7-8 (adult male) | Size 6-7 (adult female) |
Tube components: Outer cannula, inner cannula (if double lumen), cuff, pilot balloon, 15mm connector, flange with eyelets for tapes.
(Cummings; Khaja et al., Cureus 2022)
10. COMPLICATIONS
FLOWCHART: Complications of Percutaneous Tracheostomy
┌─────────────────────────────────────────────────────────────┐
│ COMPLICATIONS OF PERCUTANEOUS TRACHEOSTOMY │
│ (Classified by Timing) │
├─────────────────────────────────────────────────────────────┤
│ │
│ IMMEDIATE (Intraoperative) │
│ ├── Haemorrhage (minor: venous ooze; major: arterial) │
│ ├── Desaturation / Hypoxaemia │
│ ├── Loss of airway (tube displacement/accidental extubation│
│ ├── Posterior tracheal wall perforation │
│ ├── Oesophageal placement (false passage) │
│ ├── Subcutaneous emphysema / Pneumothorax │
│ ├── Air embolism │
│ ├── Paratracheal insertion │
│ └── Death │
│ │
│ EARLY (Within days to 1 week) │
│ ├── Tube obstruction (secretions, blood clot) │
│ ├── Tube displacement / accidental decannulation │
│ ├── Stomal infection / cellulitis │
│ ├── Surgical emphysema │
│ ├── Aspiration │
│ └── Ventilator-associated pneumonia (VAP) │
│ │
│ LATE (Weeks to months) │
│ ├── Tracheal stenosis (most important long-term) │
│ ├── Tracheoarterial fistula (life-threatening) │
│ ├── Tracheo-oesophageal fistula (TOF) │
│ ├── Persistent stoma / difficult wound closure │
│ ├── Tracheomalacia │
│ └── Dysphagia / dysphonia / impaired cough │
└─────────────────────────────────────────────────────────────┘
Important Complications in Detail:
1. Tracheal Stenosis (Most important late complication)
- Incidence: 1-2% (PDT) vs. 2-3% (surgical)
- Mechanism: mucosal injury at cuff site → fibrous scarring → subglottic/tracheal narrowing
- Prevention: keep cuff pressure < 20-25 cmH2O, proper tube size, avoid high stoma
- Presentation: progressive dyspnoea after decannulation
2. Tracheoarterial Fistula (Catastrophic)
- Occurs within 3 weeks - rare (0.1%)
- Innominate artery eroded by low-lying tube or cuff
- Presents as sentinel bleed or massive haemoptysis
- Emergency treatment: hyperinflate cuff + urgent surgical ligation
3. Haemorrhage
- Immediate: anterior jugular veins, thyroid vessels
- PDT: lower risk than surgical tracheostomy (meta-analyses confirm)
- Table from Cummings: PDT vs. surgical tracheostomy complication comparison
(Cummings; Scott-Brown's; AME Medical Journal updated review)
11. ADVANTAGES OF PDT OVER SURGICAL TRACHEOSTOMY
| Parameter | Percutaneous (PDT) | Surgical (Open) |
|---|---|---|
| Setting | Bedside ICU | Operating theatre |
| Time | 10-20 minutes | 20-40 minutes |
| Incision size | 1.5-2 cm | 3-5 cm |
| Wound infection | Lower | Higher |
| Haemorrhage | Less | More |
| Scarring | Less | More |
| Cost | Lower (no OR use) | Higher |
| Difficult anatomy | Problematic | Preferred |
| Emergency airway | Not suitable | Preferred |
| Children | Avoid | Preferred |
(Cummings; systematic review: Delaney et al., Crit Care 2006; Scott-Brown's)
12. ROLE OF BRONCHOSCOPY IN PDT
Flexible fibreoptic bronchoscopy during PDT provides:
- Real-time confirmation of needle tip position in trachea
- Ensures midline placement (10 o'clock to 2 o'clock position)
- Prevents posterior wall injury
- Confirms correct inter-ring placement (below ring 1)
- Confirms final tracheostomy tube position in trachea
Current recommendation (Lais & Piquilloud, Curr Opin Crit Care 2025): "In the absence of contraindications, the percutaneous single dilator technique under fibroscopic guidance should be the first choice."
Ultrasound guidance (emerging): Pre-procedural neck USS:
- Identifies vascular structures overlying trachea
- Confirms midline and inter-ring position
- Reduces haemorrhagic complications
13. POST-OPERATIVE CARE
Immediate:
- CXR to exclude pneumothorax / confirm tube position
- Continue monitoring: SpO2, capnography
- Ensure secure fixation (sutures + collar ties)
- Avoid early tube change - PDT tubes should NOT be changed before day 10 (tract not yet established; risk of false passage)
Daily care:
- Inner cannula cleaning every 4-8 hours
- Stomal care: clean with NS, apply split gauze
- Suction via inner cannula
- Cuff pressure monitoring: maintain 20-25 cmH2O (use manometer)
- Humidification for all ventilated patients
Communication and swallowing:
- Speech-language pathology (SLP) assessment
- Speaking valve (Passy-Muir) - only with cuff deflated
- Blue dye swallow test to assess aspiration
(Cummings, Table 7.3 - AAO-HNS Consensus Statement on Tracheostomy Care)
14. DECANNULATION
Criteria for Decannulation:
- Underlying indication resolved
- Able to maintain patent airway without tube
- Adequate cough and secretion clearance
- Safe swallowing mechanism confirmed
- No significant residual tracheal pathology
Decannulation Protocol:
ASSESS candidacy
↓
DOWNSIZE tube (sequential)
↓
CAPPING TRIAL (plug the tube for 24-48 hours)
↓
If passes (SpO2 stable, no distress)
↓
DECANNULATE
↓
Apply occlusive dressing
↓
Stoma closes spontaneously (3-10 days)
(Cummings; Scott-Brown's)
15. PERCUTANEOUS TRACHEOSTOMY IN SPECIAL SITUATIONS
1. Obese Patients:
- US guidance for site identification strongly recommended
- Longer-shank tracheostomy tubes needed
- Higher complication rate - some argue surgical preferred
2. COVID-19 Patients (Recent evidence):
- During pandemic: PDT widely used (ICU patients, high demand)
- Delayed tracheostomy (>10 days from intubation) adopted due to aerosol risk
- Arnold et al., J Bronchology Interv Pulmonol 2023 reported outcomes of PDT in SARS-CoV-2 respiratory failure patients
- Modified PPE protocols developed for aerosol-generating procedure
3. Anticoagulated Patients:
- Bridging therapy protocols
- Fresh frozen plasma / vitamin K to correct INR < 1.5 before procedure
4. Paediatric Patients:
- PDT generally AVOIDED in children < 12 years (Namavarian et al., systematic review, Int J Pediatr Otorhinolaryngol 2024)
- Smaller tracheal diameter, softer cartilage, higher complication risk
- Surgical tracheostomy preferred in children
16. COMPARISON: PDT vs. SURGICAL TRACHEOSTOMY (Meta-Analysis Summary)
| Outcome | PDT | Surgical | Significance |
|---|---|---|---|
| Overall complications | Lower | Higher | Favours PDT |
| Wound infection | 1-2% | 5-10% | Favours PDT |
| Perioperative haemorrhage | Lower | Higher | Favours PDT |
| Mortality | Similar | Similar | No difference |
| Tracheal stenosis | Similar | Similar | No difference |
| Post-procedural haemorrhage | Higher | Lower | Favours surgical |
(Delaney, Bagshaw, Nalos: systematic review and meta-analysis, Crit Care 2006 - cited in Cummings)
17. RECENT ADVANCES (2020-2025)
-
Ultrasound-guided PDT: Pre-procedural and real-time ultrasound guidance reduces vascular injury, confirms correct inter-ring placement, and identifies aberrant vessels. Now considered complementary to bronchoscopy.
-
Single-dilator technique dominance: Meta-analysis confirms Ciaglia Blue Rhino (single conical dilator) has fewer failures and complications than multi-dilator or forceps techniques.
-
COVID-19 experience: Pandemic validated PDT as a safe bedside procedure even in high-risk ventilated patients; timing protocols and PPE adaptations now standardised.
-
Tracheostomy weaning protocols: Personalised, multidisciplinary weaning teams shown to reduce ICU stay and improve decannulation rates.
-
Videolaryngoscope guidance: Some centres now use video-laryngoscopic or transnasal flexible scope to guide PDT instead of bronchoscopy, with comparable safety.
-
Robotic/AI-assisted tracheostomy: Experimental - robotic platforms for surgical tracheostomy being evaluated; not yet clinical standard.
-
Early vs. late timing: Lais & Piquilloud (2025) confirm personalised approach - no universal timing rule; early tracheostomy (< 7 days) beneficial in select populations (neuro-ICU, prolonged weaning expected).
-
PDT in paediatrics: Systematic review (2024) confirms PDT feasible in select adolescents but surgical tracheostomy remains gold standard in children.
(Lais & Piquilloud, Curr Opin Crit Care 2025 - PMID 39588741; Namavarian et al., Int J Pediatr Otorhinolaryngol 2024 - PMID 38185003; AME Medical Journal updated review, Moore et al.)
18. SUMMARY DIAGRAM: PDT AT A GLANCE
┌──────────────────────────────────────────────────────────┐
│ PERCUTANEOUS TRACHEOSTOMY - SUMMARY │
├──────────────┬───────────────────────────────────────────┤
│ INDICATIONS │ Prolonged MV > 7-10 days, airway │
│ │ obstruction, pulmonary toilet │
├──────────────┼───────────────────────────────────────────┤
│CONTRAINDICS │ Emergency, paediatrics, uncorrected │
│ │ coagulopathy, non-palpable trachea │
├──────────────┼───────────────────────────────────────────┤
│ GOLD │ Ciaglia Blue Rhino (single conical │
│ STANDARD │ dilator) + Bronchoscopic guidance │
├──────────────┼───────────────────────────────────────────┤
│ KEY STEPS │ Position → Puncture (ring 1-2/2-3) │
│ │ → Guidewire → Catheter → Dilate → Tube │
├──────────────┼───────────────────────────────────────────┤
│ COMPLICATNS │ Haemorrhage, tracheal stenosis, │
│ │ tracheoarterial fistula, displacement │
├──────────────┼───────────────────────────────────────────┤
│ ADVANTAGE │ Bedside, lower infection, smaller scar, │
│ │ faster, less costly │
├──────────────┼───────────────────────────────────────────┤
│ TUBE CHANGE │ NOT before Day 10 (PDT) │
├──────────────┼───────────────────────────────────────────┤
│ RECENT ADV │ US guidance, COVID protocols, personalised │
│ │ timing, single-dilator meta-analysis data │
└──────────────┴───────────────────────────────────────────┘
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (8th ed.) - Chapter 72, Vol. 2, pp. 1085-1087
- Cummings Otolaryngology Head and Neck Surgery (7th ed.) - Chapter 7, Box 7.1, Box 7.3, pp. 134-145
- Bailey and Love's Short Practice of Surgery (28th ed.) - Percutaneous Tracheostomy section
- Ciaglia P et al. - Elective percutaneous dilatational tracheostomy. Chest 1985;87:715-719
- Delaney A, Bagshaw SM, Nalos M - PDT vs surgical tracheostomy, systematic review and meta-analysis. Crit Care 2006;10:R55
- Khaja M, Haider A, et al. - Percutaneous Tracheostomy: A Bedside Procedure. Cureus 2022. PMID: 35573523
- Lais G, Piquilloud L - Tracheostomy: update on why, when and how. Curr Opin Crit Care 2025. PMID: 39588741
- Namavarian A et al. - Percutaneous tracheostomy in the pediatric population: systematic review. Int J Pediatr Otorhinolaryngol 2024. PMID: 38185003
- Moore et al. - An updated review in percutaneous tracheostomy. AME Medical Journal
- Dhingra PL - Diseases of Ear, Nose and Throat (6th ed.) - Tracheostomy chapter
- Hazarika P - Textbook of Ear, Nose and Throat - Tracheostomy
RGUHS Exam Tip: This is a 50-mark long essay, so cover all sections above. The examiner expects: (a) definition + historical note, (b) anatomy, (c) indications/contraindications in tabular/box format, (d) step-by-step technique with a flowchart, (e) types of PDT, (f) complications (classified as immediate/early/late), (g) post-operative care, (h) comparison with surgical tracheostomy, and (i) recent advances. Drawing a neat flowchart of the procedure and the complications classification diagram will fetch full marks. Citing Cummings (Box 7.3) and Scott-Brown's (Fig. 72.6) demonstrates textbook familiarity expected at the RGUHS MS ENT level.
This is a shared conversation. Sign in to Orris to start your own chat.