

IMG-20260709-WA0023.jpg
IMG-20260709-WA0021.jpg
Interpret properly the x-rays defining feature how to demonstrate during viva. Give proper finding related questions answer.
analyse_media
analyse_media
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have all the information needed for a comprehensive viva-oriented answer. Let me compose the full response.
X-Ray Interpretation: Barium Enema Studies - Complete Viva Guide
IMAGE 1 (Multi-panel Barium Enema Series) - Inflammatory Bowel Disease Pattern
Identify the Study First (Say This in Viva)
"This is a Barium Enema (BE) examination of the large bowel in a 35-year-old male (Naresh Kr. Dubey, dated 09-05-2013, performed at Digital Path Lab, Bokaro). The study appears to be a single-contrast BE with post-evacuation mucosal relief views. PA projections are shown."
Systematic Radiological Findings
1. Contrast Distribution
- Barium fills the rectum, sigmoid, descending colon, splenic flexure, transverse colon and hepatic flexure
- The ascending colon and caecum are NOT opacified - suggest either obstruction at hepatic flexure, severe spasm, or technical limitation
2. Haustral Pattern (KEY FINDING)
- Normal haustral sacculations are markedly reduced or absent in the descending and sigmoid colon
- This gives a "lead pipe" or "hose-pipe" colon appearance
- In the mucosal relief views (post-evacuation panels, lower right), the mucosa appears coarse, thickened and irregular
3. Mucosal Changes
- Cobblestone / reticular mucosal pattern visible in transverse and descending colon segments
- Irregular surface contour suggesting ulceration or pseudopolyps
4. Calibre
- Generalised narrowing and reduced distensibility in descending and sigmoid segments
- No massive dilatation (no toxic megacolon pattern in this series)
Diagnosis: Chronic Ulcerative Colitis / Inflammatory Bowel Disease
The combination of:
- Loss of haustra
- Lead pipe appearance
- Continuous involvement from rectum upward
- Irregular thickened mucosa
- Absence of normal distensibility
...is the classical barium enema picture of chronic ulcerative colitis.
IMAGE 2 (Single Film - Massive Rectal Dilatation)
Identify the Study First
"This is a plain/single-contrast Barium Enema film showing the pelvis and lower abdomen in PA projection. There is a single large contrast pool occupying the entire pelvic and lower abdominal cavity."
Systematic Findings
1. Massive Megarectum / Megacolon
- The rectosigmoid region is aneurysm ally, massively dilated - the barium pool extends from the pelvis to the mid-abdomen
- The lumen occupies nearly the entire pelvic cavity, compressing adjacent structures
2. Loss of Haustra
- The dilated segment has completely smooth, featureless walls - no haustral markings visible
- This is due to chronic over-distension causing wall atrophy
3. Fecaloma / Fecal Load
- Within and around the barium pool, a mottled "soap-bubble" filling defect is visible
- This represents massive retained feces (fecaloma) mixed with contrast
4. Transition Zone (Critical Feature)
- There is an abrupt calibre change between the massively dilated rectosigmoid and the relatively collapsed, narrow descending colon superiorly
- This is the classic "transition zone" - the hallmark of Hirschsprung's disease
- Below = narrow, aganglionic segment; Above = dilated, ganglion-containing bowel
5. Proximal Bowel
- Upper abdomen shows gas-filled loops with mottled fecal pattern
- Small bowel displaced superiorly due to mass effect of the dilated rectosigmoid
Diagnosis: Hirschsprung's Disease (Congenital Aganglionic Megacolon) OR Idiopathic Megacolon/Megarectum
Compare with the textbook image (Sleisenger & Fordtran, Fig 98.22A):
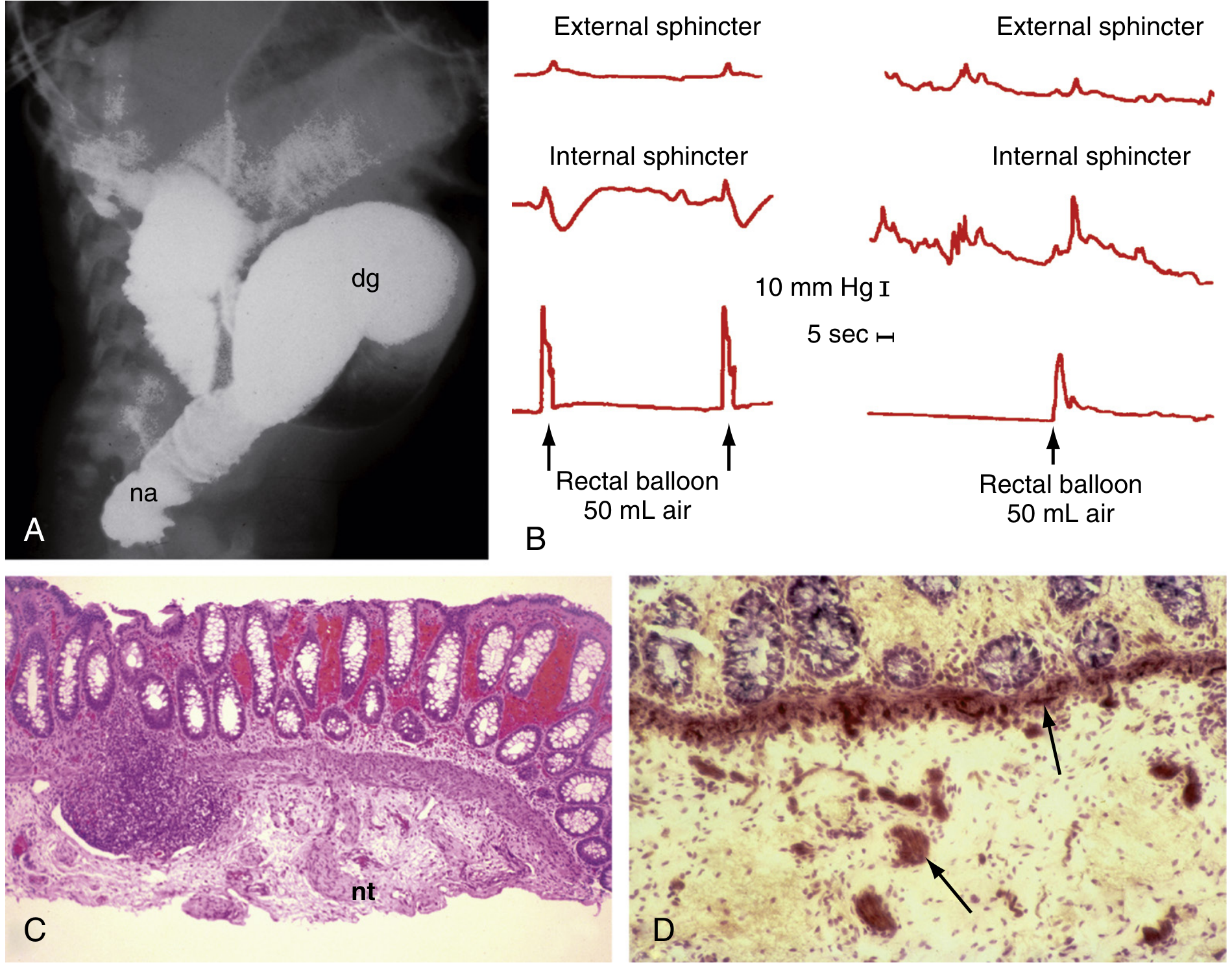
Fig 98.22A - Barium enema in Hirschsprung's disease: note narrow distal aganglionic segment (na) and dilated proximal ganglionic segment (dg) - Sleisenger & Fordtran's GI & Liver Disease
And the classic infant barium enema image:
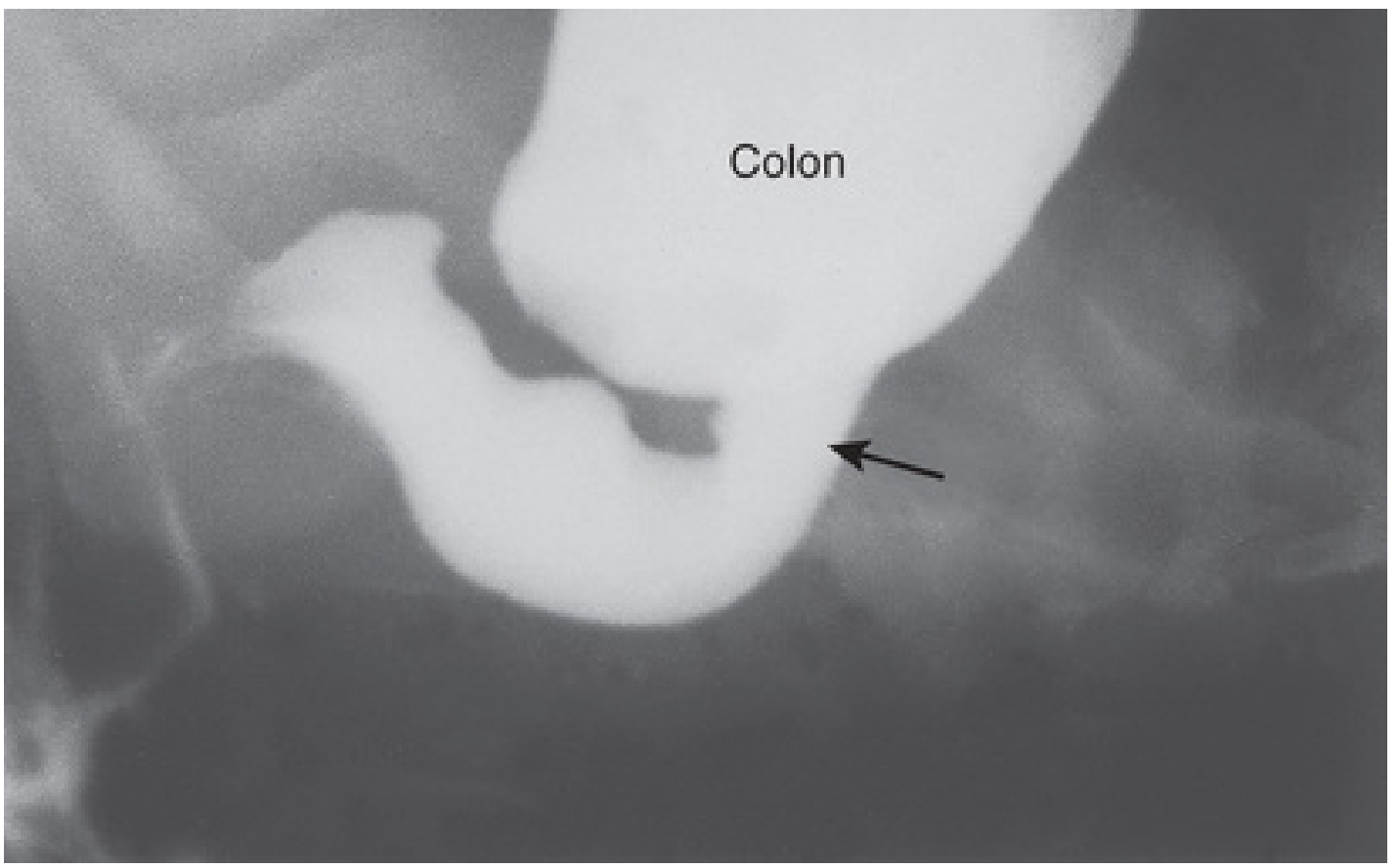
Fig 11.27 - Hirschsprung's disease barium enema in infant: narrow distal segment, dilated proximal colon, transition zone (arrow) - The Developing Human (Moore)
Complete Viva Q&A - How to Present and Answer
Q1: "What is this investigation?"
A: "This is a Barium Enema examination - a retrograde contrast study of the large bowel using barium sulfate introduced via the rectum under fluoroscopic control. Image 1 is a multi-view series showing single-contrast and mucosal relief views. Image 2 appears to be a single-contrast fill phase film."
Q2: "What are the projections and views shown?"
A: "PA (postero-anterior) projection, abdomen. The multi-panel series includes filled views and post-evacuation mucosal relief views, which are the most informative for mucosal detail."
Q3: "What is the KEY abnormality in Image 1?"
A: "The most striking abnormality is the loss of normal haustral pattern in the descending and sigmoid colon, giving a 'lead-pipe' or 'hosepipe' appearance. Additionally, the mucosal relief views show irregular, thickened, cobblestone mucosa consistent with chronic inflammatory bowel disease. The bowel wall appears narrowed and non-distensible."
Q4: "What do you mean by 'lead-pipe colon'?"
A: "Normally the colon has regular sacculations called haustra, formed by the tenia coli bunching the wall. In chronic ulcerative colitis, fibrosis and muscular hypertrophy obliterate these sacculations, resulting in a smooth, tube-like, non-distensible colon - resembling a lead pipe. This indicates longstanding, burnt-out chronic colitis."
Q5: "What is the classic barium enema finding sequence in ulcerative colitis?"
A:
- Early: Fine granular mucosa (due to mucosal oedema/hyperemia), loss of normal sharp mucosal lines
- Active: Spiculation (collar-stud ulcers projecting beyond bowel wall), pseudopolyps (islands of surviving mucosa surrounded by ulceration)
- Chronic: Loss of haustra, lead-pipe colon, foreshortening, widened presacral space
Q6: "What is the KEY abnormality in Image 2?"
A: "There is massive dilatation of the rectosigmoid colon forming a huge barium pool occupying the entire pelvis. The dilated segment has completely smooth walls with no haustra. There is an abrupt transition to a narrow, collapsed segment proximally. This transition zone is the critical finding, representing the junction between the aganglionic (distal, narrow) and ganglionic (proximal, dilated) bowel - characteristic of Hirschsprung's disease."
Q7: "Describe the transition zone - where is it and what does it signify?"
A: "The transition zone is the funnel-shaped area where the narrow aganglionic distal segment widens abruptly into the dilated proximal bowel. It is best seen on the lateral view of the rectum or on 24-hour delayed films. It represents the pathophysiological boundary - below it, there are no ganglion cells (Auerbach's and Meissner's plexuses absent), causing persistent tonic contraction and functional obstruction. Above it, normal peristalsis continues into obstructed, progressively dilating bowel."
Q8: "What is the rectosigmoid index?"
A: "The rectosigmoid index (RSI) is measured on the barium enema - it is the ratio of the diameter of the sigmoid colon to the diameter of the rectum. Normally the sigmoid is wider than the rectum (RSI >1.0). In Hirschsprung's disease, the rectum is wider than the sigmoid (RSI <1.0) because the aganglionic narrow segment includes the rectum. An RSI <1 supports Hirschsprung's diagnosis."
Q9: "What is the pathology of Hirschsprung's disease?"
A: "Hirschsprung's disease (congenital aganglionic megacolon) results from failure of neural crest cell migration into the distal bowel wall during the 5th-7th weeks of intrauterine life. This causes absence of ganglion cells in the myenteric (Auerbach's) and submucosal (Meissner's) plexuses in a variable length of distal bowel - always including the rectum. The aganglionic segment remains in tonic contraction, causing functional obstruction and proximal dilatation. The RET proto-oncogene is the major susceptibility gene." - Schwartz's Principles of Surgery, 11th ed.
Q10: "How do you confirm the diagnosis of Hirschsprung's disease?"
A: "The gold standard is rectal suction biopsy. Samples are taken at 1 cm, 2 cm, and 3 cm from the dentate line. Histology shows: (1) absence of ganglion cells in Meissner's plexus, (2) hypertrophied nerve bundles, (3) increased acetylcholinesterase (AChE) staining in the lamina propria and muscularis mucosae. Barium enema supports but cannot confirm the diagnosis - manometry showing absent recto-anal inhibitory reflex (RAIR) is also useful." - Schwartz's, p.392-396
Q11: "What is the mottled/soap-bubble appearance in Image 2?"
A: "The mottled 'soap-bubble' filling defect within the barium pool represents a fecaloma - a massive accumulation of retained fecal material mixed with contrast. Barium coats the irregular fecal surface, creating this characteristic mottled pattern. It indicates long-standing functional obstruction and severe fecal retention."
Q12: "What are the indications and contraindications of barium enema?"
A:
- Indications: Evaluation of colonic polyps, inflammatory bowel disease extent, diverticular disease, suspected colonic carcinoma, Hirschsprung's disease, colonic obstruction
- Contraindications: Toxic megacolon (risk of perforation), suspected free perforation, acute severe ulcerative colitis, recent deep rectal biopsy (<5 days), bowel perforation, peritonitis
- S Das Manual of Clinical Surgery, 13th ed. - "If plain X-ray shows colonic dilatation (megacolon), barium studies should be judged carefully"
Q13: "What is the difference between single-contrast and double-contrast barium enema?"
A:
- Single-contrast: Barium alone fills the colon - good for demonstrating calibre, strictures, large filling defects, transition zones, and megacolon
- Double-contrast (air-contrast): Barium coats the mucosa, then air inflates the colon - far superior for detecting small polyps, early mucosal changes, pseudopolyps in IBD, and early ulceration. It is the preferred technique for screening and IBD assessment unless megacolon is suspected
Q14: "What else can cause megacolon on barium enema?"
A:
- Hirschsprung's disease (aganglionic - transition zone present distally)
- Idiopathic/psychogenic megacolon (older patients, no transition zone, rectum dilated)
- Chagas disease (South American trypanosomiasis destroying myenteric plexus)
- Chronic constipation / laxative abuse
- Hypothyroidism / electrolyte imbalance
- Toxic megacolon (complicating UC or Crohn's - transverse colon >6 cm, thumb-printing, mucosal islands)
- Neurogenic / spinal cord injury
Q15: "How would you differentiate Hirschsprung's from idiopathic megacolon on barium enema?"
A:
| Feature | Hirschsprung's | Idiopathic Megacolon |
|---|---|---|
| Age at presentation | Usually neonatal/infancy | Childhood/adult |
| Transition zone | Present (distal narrow segment) | Absent |
| Rectum | Narrow (aganglionic) | Dilated |
| Rectosigmoid index | <1 (rectum narrower than sigmoid) | >1 |
| 24-hr delayed film | Retained barium in narrow segment | Barium passes |
| Rectal biopsy | No ganglion cells | Normal ganglion cells |
Q16: "What mucosal pattern is shown in the post-evacuation views (Image 1)?"
A: "The post-evacuation mucosal relief views show the mucosa coated by a thin layer of residual barium. In this case the mucosal pattern is irregular, thickened, and coarse - with a cobblestone or granular texture. This is indicative of chronic colonic inflammation, as seen in IBD. In normal bowel, the post-evacuation view shows fine, parallel mucosal folds with regular haustral impressions."
How to Present at Viva - The Template
- Identify: "This is a barium enema examination..." - state patient details, date, institution
- Describe technique: Single vs double contrast, projection, phases shown
- Systematic review:
- Rectum → Sigmoid → Descending → Transverse → Ascending → Caecum
- Haustra, calibre, mucosal pattern, filling defects, strictures, transition zones
- State the KEY finding prominently
- Give the diagnosis with reasoning
- Offer differential diagnoses
- State what investigation confirms the diagnosis
Summary Box for Quick Revision
| Feature | Image 1 (Multi-panel) | Image 2 (Single film) |
|---|---|---|
| Diagnosis | Chronic Ulcerative Colitis / IBD | Hirschsprung's Disease / Idiopathic Megacolon |
| Key finding | Lead-pipe colon, loss of haustra, mucosal irregularity | Massive megarectum, transition zone, fecaloma |
| Confirmatory test | Colonoscopy + biopsy | Rectal suction biopsy (AChE staining) |
| Classic sign name | Lead-pipe / hosepipe colon | Bird's beak / funnel transition zone |
| Contraindication to BE | Toxic megacolon | If perforation suspected |
This is a shared conversation. Sign in to Orris to start your own chat.