Describe patjophysiological changes in ear and paranasal sinus in flight and diving
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material. Let me compile the full answer from all sources gathered.
Pathophysiological Changes in the Ear and Paranasal Sinuses During Flight and Diving
The unifying physical principle is Boyle's Law: at constant temperature, the volume of a gas varies inversely with pressure. As ambient pressure increases (descent in water, or aircraft pressurization) or decreases (ascent in water, or aircraft climbing/cabin depressurization), the gas volumes in all body air-containing spaces must change accordingly. If equalization fails, tissue injury results - this is barotrauma.
I. THE EAR
A. External Ear
The external auditory canal is normally open to ambient pressure, so external ear barotrauma is uncommon. However, if the canal is occluded by cerumen impaction, otitis externa, tight-fitting ear plugs, or a close-fitting wetsuit hood, a sealed air pocket forms. On descent, this trapped gas contracts, creating a relative negative pressure in the canal. The tympanic membrane is then subjected to negative pressure on its outer surface while the middle ear (if equalized) is at ambient pressure. This pulls the drum outward, causing ecchymosis, edema, and possible haemorrhage of the drum and canal skin - termed "reversed ear" or "reverse squeeze."
B. Middle Ear Barotrauma (Barotitis Media / "Ear Squeeze")
This is the most common medical problem in scuba diving and a very common complaint in air travel.
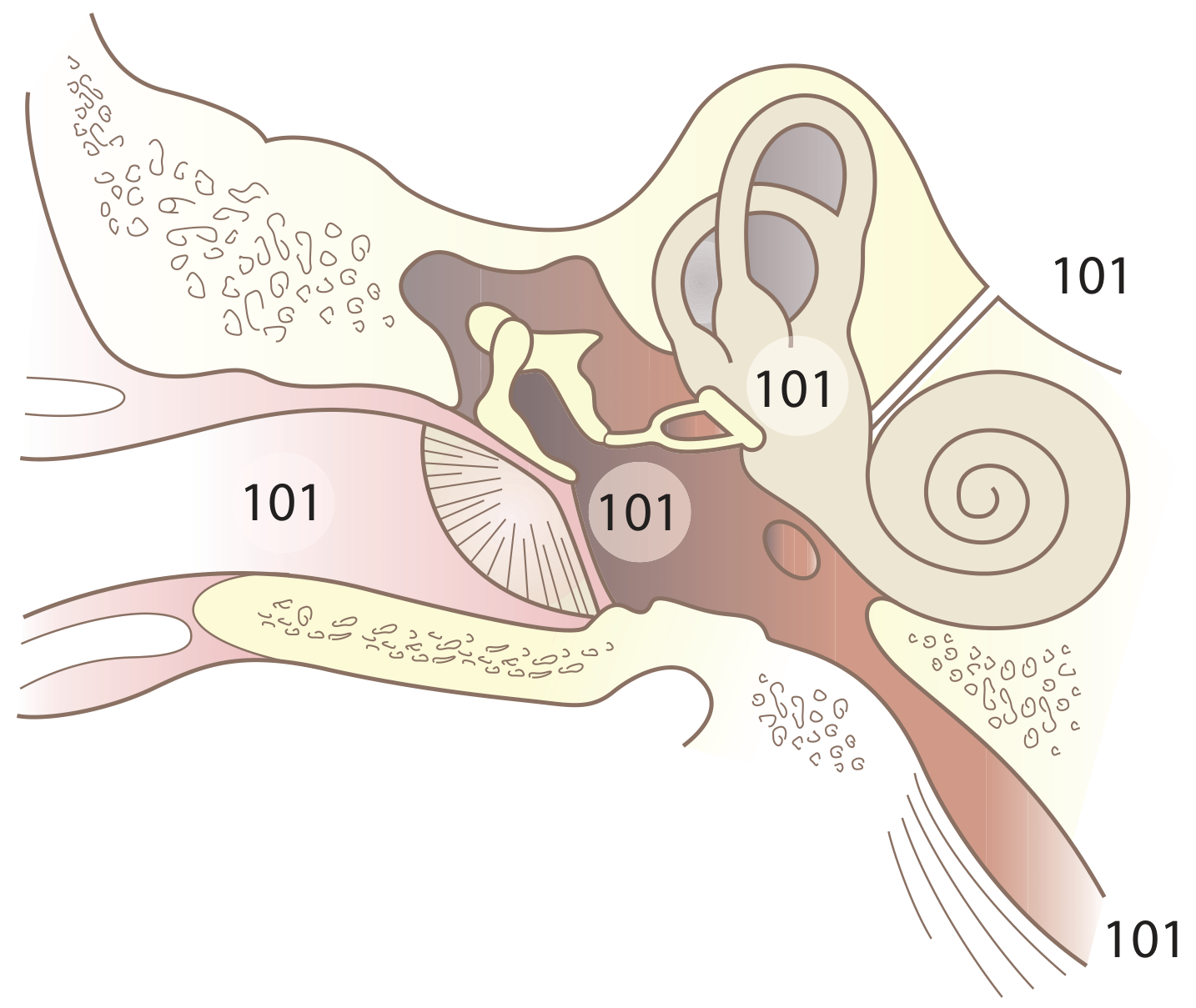
Anatomy and Normal Physiology
The middle ear is an air-filled space whose only outlet to the atmosphere is the Eustachian tube, which connects the middle ear to the nasopharynx. Under normal conditions, the Eustachian tube is kept closed by the surrounding mucosal folds; it opens briefly with swallowing, yawning, or voluntary muscle action (tensor and levator palati muscles) to equalize pressure.
Pathophysiology on Descent (Compression)
As a diver descends or an aircraft pressurizes, ambient pressure rises. The middle ear pressure becomes increasingly negative relative to ambient unless the Eustachian tube opens to allow air in. The sequence of events (illustrated in Farmer & Thomas's classic model):
| Pressure Differential | Structural Event |
|---|---|
| ~8.7 kPa (60 mmHg) at ~0.86 m depth | Tympanic membrane distends inward; sensation of fullness and pain |
| ~13 kPa (90 mmHg) at ~1.3 m depth | "Eustachian locking" - levator palati muscles can no longer overcome the external closing pressure |
| Beyond locking | Mucosal congestion and edema of middle ear mucosa; transudation of fluid; vascular engorgement |
| Further descent | Haemorrhage into middle ear; tympanic membrane may rupture; flooding with cold water causes caloric vertigo |
The Teed classification grades the severity of barotitis:
- Grade 0: No otoscopic change, only subjective symptoms
- Grade 1: Injection of the malleus handle and periphery of TM
- Grade 2: Injection of entire TM
- Grade 3: Haemorrhage within the substance of TM
- Grade 4: Free haemorrhage in the middle ear (haemotympanum)
- Grade 5: Perforation of TM
The key mechanism is that when the Eustachian tube cannot be opened (blocked by mucosal inflammation from URTI, allergy, or physical obstruction), the increasing ambient pressure drives the drum inward. The ambient pressure is reflected in the middle ear vasculature, increasing transmural pressures, causing transudation and mucosal engorgement. This further worsens Eustachian tube dysfunction, creating a vicious cycle.
Pathophysiology on Ascent (Decompression)
During ascent, middle ear air pressure rises above ambient. Normally this causes passive venting through the Eustachian tube (air flows down a pressure gradient into the pharynx, approximately every 13.25 m of ascent in flight). If, however, the Eustachian tube has become swollen from prior mild barotrauma during descent, this passive venting cannot occur. The result:
- Tympanic membrane bulges outward (instead of inward as in descent)
- A traction force is applied via the ossicular chain to the oval window
- Simultaneously an inward (compressive) force acts on the round window membrane
- Perilymphatic pressure decreases as ambient pressure decreases, increasing the trans-window pressure gradient
- Risk of perilymphatic fistula (oval/round window rupture) on ascent
C. Inner Ear Barotrauma (Compression Barotrauma)
This is less common but more serious. Three distinct pathological entities are recognized in histopathological studies:
1. Inner Ear Haemorrhage
- Results from rupture of small vessels within the cochlea or labyrinth
- Produces transient or mild vestibular symptoms and mild-to-moderate sensorineural hearing loss (SNHL)
- Generally good prognosis for recovery
2. Labyrinthine Membrane Tears
- Tears of Reissner's membrane or other intralabyrinthine membranes
- Presents similarly to an acute Ménière's attack: sudden severe vertigo, tinnitus, and characteristic low-frequency SNHL (the mixing of endolymph and perilymph caused by membrane tears disrupts cochlear potentials)
- Temporal bone studies confirm Reissner's membrane rupture and haemorrhage around the round window membrane, with rupture of utricle and saccule in severe cases
- Hearing loss is typically permanent
- Has been documented in airline passengers as well as divers
3. Perilymphatic Fistula (Round/Oval Window Rupture)
This is the most important complication. The mechanism involves two pathways:
Implosive route (more common on descent):
- If a forced Valsalva maneuver successfully opens the Eustachian tube after prolonged closure, there is a sudden sharp rise in middle ear pressure
- This pressure surge is transmitted directly to the oval and round window membranes
- Rupture of the round window membrane or disruption of the stapes footplate/annular ligament follows
- Perilymph leaks into the middle ear
Explosive route:
- If the Eustachian tube remains closed during a forced Valsalva, the rise in intrathoracic and intracranial pressure is transmitted via the patent cochlear aqueduct or internal auditory meatus to the perilymph
- This dramatically increases perilymphatic pressure from within, rupturing the round window membrane outward into the middle ear
Experimental studies in cats show round window rupture occurs at pressure gradients of 16-40 kPa (120-300 mmHg). Predisposing factors include congenital weakness of the annular ligament, prior stapes surgery, and large cochlear/vestibular aqueducts.
Clinical presentation: Sudden severe SNHL, tinnitus, and severe vertigo after a forced Valsalva. This is a surgical emergency in many cases.
D. Alternobaric Vertigo
A distinct entity occurring during ascent when middle ear pressures become unequal between the two ears (asymmetric Eustachian tube function). The differential pressure stimulates one labyrinth asymmetrically, producing sudden disorienting vertigo during ascent, which can be dangerous during diving (risk of drowning) or in pilots. It is:
- Short-lived and self-correcting
- Very common in mild forms
- Without residual audiological or neurological sequelae
E. Barotraumatic Facial Palsy
Rare but recognized. The pressure differential in the middle ear can be transmitted directly to the facial nerve via natural dehiscences in the Fallopian (facial) canal. Symptoms are relieved by pressure-equalization tubes or improvement of Eustachian tube function. - Cummings Otolaryngology
F. Decompression Sickness - Inner Ear (Type II DCS)
In diving (not flight barotrauma per se), rapid ascent without decompression stops allows dissolved nitrogen to come out of solution and form bubbles in soft tissues and blood vessels, including the labyrinthine vasculature and perilymph. This causes:
- Sensorineural deafness
- Tinnitus
- Vertigo ("staggers")
- Disequilibrium
This is distinct from barotrauma and represents a different pathophysiological mechanism (bubble formation rather than mechanical pressure injury).
II. PARANASAL SINUSES
Mechanism
The paranasal sinuses (frontal, maxillary, ethmoid, sphenoid) are air-filled cavities that communicate with the nasal cavity through narrow ostia. Unlike the Eustachian tube which requires active muscle action to open, sinus ostia equalization is passive - gas simply flows in and out. However, when ostia are obstructed (by mucosal edema, polyps, deviated septum, URTI, or allergic rhinitis), pressure equalization fails.
Sinus Barotrauma ("Sinus Squeeze" / Aerosinusitis)
On descent (compression):
- When a sinus ostium is occluded, the gas within the sinus cannot equilibrate as ambient pressure rises
- The sinus mucosa is subjected to a relative negative pressure (the sinus pressure lags behind rising ambient pressure)
- Mucosal blood vessels become engorged (venous congestion) and eventually rupture into the sinus lumen
- Haemorrhage into the sinus cavity follows, with transudation of fluid
- The result is mucosal edema, submucosal haemorrhage, and bloody secretions
On ascent (decompression):
- If a ball-valve obstruction exists (allowing air to enter but not leave, or vice versa), or if the sinus filled with blood/fluid on descent, gas cannot escape on ascent
- Expanding gas in the sinus increases pressure, causing pain
- Epistaxis is characteristic on ascent as engorged mucosal vessels bleed
Sinus-Specific Features
| Sinus | Clinical Feature |
|---|---|
| Frontal | Most commonly affected; severe frontal pain over sinus |
| Maxillary | Pain over cheek; if maxillary branch of trigeminal nerve compressed during ascent → infraorbital paresthesias (usually resolve in 2-3 hours) |
| Sphenoid | Headache following a dive may indicate sphenoid sinus barotrauma - atypical presentation |
| Ethmoid | Pain at the bridge of nose; less commonly affected |
Complications
- Persistent blood in the sinus provides a culture medium for bacteria → bacterial sinusitis
- Sphenoid sinus barotrauma is particularly dangerous due to proximity to optic chiasm, cavernous sinus, pituitary, and cranial nerves II-VI
- Maxillary sinus barotrauma can mimic dental pain (referred pain via superior alveolar branches)
Aerosinusitis in Aviation
The same mechanism applies to air travel. During descent (cabin pressure increasing), blocked sinus ostia prevent equalization. Flight crew and passengers with acute sinusitis, allergic rhinitis, or nasal polyps are at risk. The use of topical vasoconstrictors before descent (e.g., xylometazoline nasal spray) is the standard preventive measure.
Summary Table
| Structure | Phase | Mechanism | Pathological Change |
|---|---|---|---|
| External ear | Descent | Canal occluded (cerumen/hood) → negative pressure in canal | TM pulled outward, canal haemorrhage |
| Middle ear | Descent | Blocked Eustachian tube → negative middle ear pressure | TM pushed inward, mucosal edema/haemorrhage → haemotympanum → TM perforation |
| Middle ear | Ascent | Blocked Eustachian tube → positive middle ear pressure | TM pushed outward, risk of oval/round window fistula |
| Inner ear | Descent | Forced Valsalva → implosive/explosive pressure surge | Round/oval window rupture, perilymphatic fistula, SNHL, vertigo |
| Inner ear | Ascent | Unequal ET function | Alternobaric vertigo |
| Inner ear | Ascent | Nitrogen bubble formation (DCS) | SNHL, tinnitus, "staggers" |
| Paranasal sinuses | Descent | Blocked ostium → negative pressure | Mucosal engorgement, haemorrhage into sinus |
| Paranasal sinuses | Ascent | Gas expansion in blocked sinus | Pain, epistaxis, risk of sinusitis |
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2 | Murray & Nadel's Textbook of Respiratory Medicine | Tintinalli's Emergency Medicine | Cummings Otolaryngology Head and Neck Surgery | ROSEN's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.