Management of acute pancreatic
Reading File
Finding Sources
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Searching PubMed
"acute pancreatitis" AND treatment
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile a thorough, well-organized response.
Management of Acute Pancreatitis
Acute pancreatitis (AP) is an inflammatory condition of the pancreas that ranges from a mild, self-limiting illness to a life-threatening emergency with multi-organ failure. About 85-90% of cases are mild and resolve spontaneously within 3-7 days. The remaining 10-15% develop moderate-to-severe or critical disease requiring intensive care.
- Harrison's Principles of Internal Medicine, 22nd ed., p. 2791
- Schwartz's Principles of Surgery, 11th ed., p. 1471
1. Severity Classification
Revised Atlanta Classification (RAC)
| Category | Features | Mortality |
|---|---|---|
| Mild | No organ failure (OF), no local complications | <1% |
| Moderately Severe | Transient OF (<48 h) and/or local complications | ~10% |
| Severe | Persistent OF (>48 h) | 20-40% |
| Critical | Persistent OF + infected necrosis | >50% |
Severity Scoring Systems
BISAP Score (score ≥3 indicates high risk):
- B - BUN >25 mg/dL
- I - Impaired mental status
- S - SIRS (≥2 of 4 criteria)
- A - Age >60 years
- P - Pleural effusion
SIRS Criteria (≥2 required):
- Core temp <36°C or >38°C
- Heart rate >90 bpm
- Respirations >20/min or PCO2 <32 mmHg
- WBC >12,000/µL, <4,000/µL, or >10% bands
Other markers: APACHE II ≥8 at 24 h, hematocrit >44%, admission BUN >20 mg/dL, CRP >100 mg/L.
2. Initial Assessment and Monitoring
All patients with suspected AP should be admitted. High-risk patients (failure to respond to initial resuscitation) require HDU/ICU admission with:
- Invasive monitoring of vital signs, CVP, urine output, blood gases
- Frequent labs: LFTs, renal function, clotting, serum calcium, blood glucose, hematocrit, BUN every 8-12 h
- CECT abdomen if organ failure, clinical deterioration, or signs of sepsis develop
CT in AP:
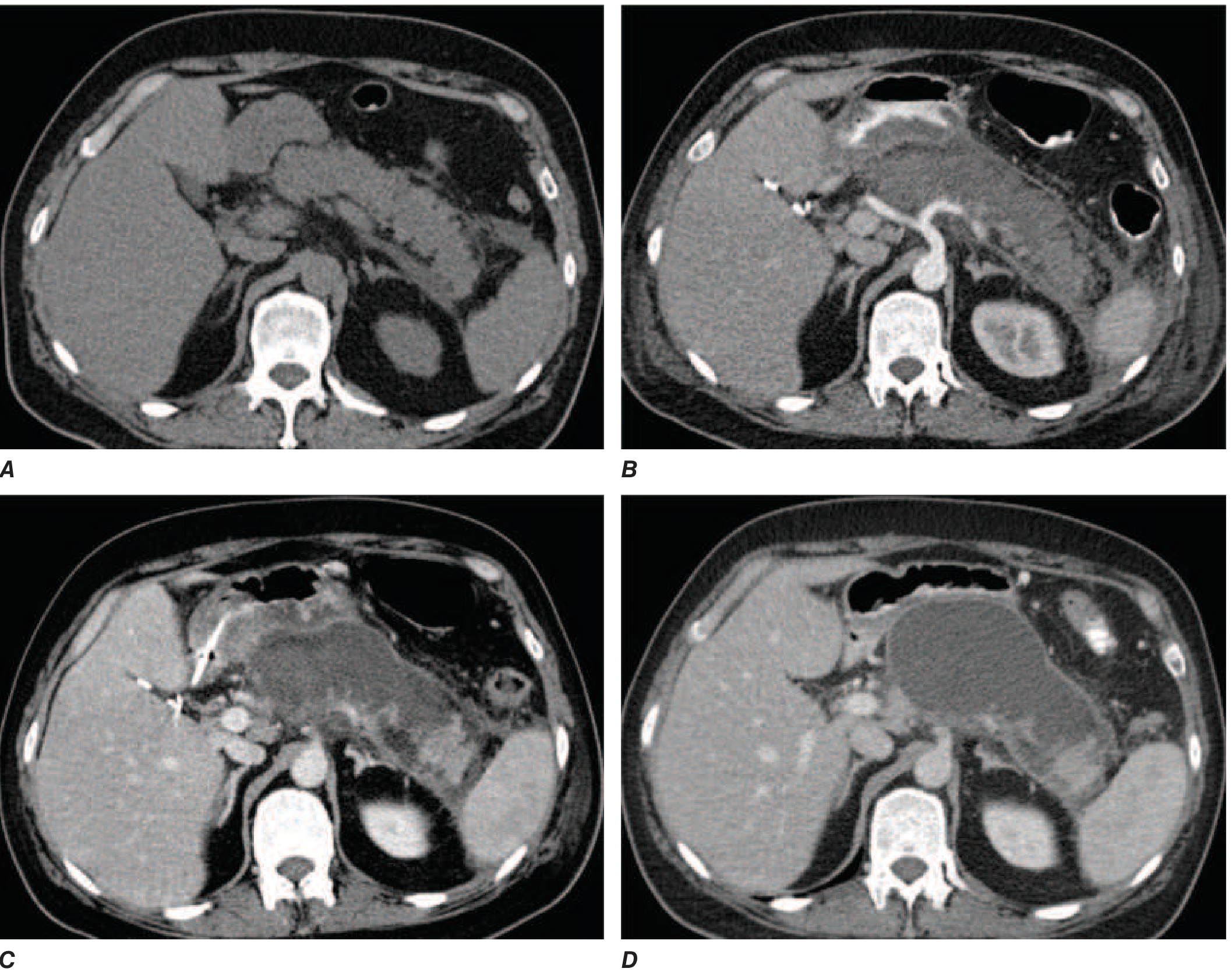
FIGURE: Evolution of acute necrotizing pancreatitis on CT. A - mild peripancreatic stranding on admission; B - extensive intrapancreatic necrosis at 1 week (lack of contrast enhancement); C - acute necrotic collection (ANC) at 2 weeks; D - walled-off necrosis (WON) replacing the pancreas at several weeks. - Harrison's Principles, p. 2790
3. Fluid Resuscitation
The single most important early intervention. Goals: restore circulating volume, normalize BP, and maintain urine output >0.5 mL/kg/h.
- Preferred fluid: Lactated Ringer's (LR) - shown to lower CRP and reduce systemic inflammation vs. normal saline
- Regimen: Initial bolus ~10-15 mL/kg, then 1.5-2 mL/kg/h
- A recent RCT showed aggressive resuscitation (15-20 mL/kg bolus + 2-3 mL/kg/h) increased fluid overload risk without improving outcomes vs. the less aggressive strategy
- Re-assess every 6-8 h; measure hematocrit + BUN every 8-12 h to guide adequacy
- Caution in elderly and those with cardiac/renal disease - over-resuscitation risk is higher
4. Analgesia
- IV narcotic analgesics (opioids) are the standard for pain control
- There is no evidence that morphine worsens AP (the old concern about sphincter of Oddi spasm has not been proven clinically significant)
- Adequate analgesia is a key pillar of early management
5. Nutritional Support
Major paradigm shift - "resting the pancreas" by prolonged NPO is no longer supported.
- Enteral nutrition (EN) is the preferred route - oral/nasogastric or nasojejunal feeding
- EN maintains gut mucosal integrity, prevents bacterial translocation, and reduces infectious complications
- Nasogastric (NG) feeding is equally effective as nasojejunal (NJ) and much easier to place
- Parenteral nutrition (PN) is reserved for cases where EN is not tolerated or not possible
- For mild AP, refeeding orally can begin once nausea/vomiting and pain have subsided (often within 24-72 h)
- For severe AP requiring nutritional support, EN should be started within 24-48 h of admission
6. Antibiotics
Prophylactic antibiotics are NOT routinely recommended for AP - multiple RCTs have failed to show benefit.
Antibiotics are indicated for:
- Proven or suspected infected pancreatic necrosis (fine-needle aspiration guided by CT, or clinical signs of infection - fever, rising WBC, deterioration at 2-4 weeks)
- Cholangitis - treat promptly
- Concurrent infections - urinary tract infection, pneumonia, line infection
When required, regimens include:
- IV imipenem-cilastatin (penetrates pancreatic tissue well)
- Ciprofloxacin + metronidazole
- Cefuroxime (IV)
- Duration: guided by cultures; prophylactic use should not exceed 14 days
7. Managing the Etiology
Gallstone Pancreatitis
- ERCP within 72 hours is indicated for severe gallstone pancreatitis or when cholangitis or biliary obstruction is present
- Cholecystectomy should be performed during the same admission for mild gallstone pancreatitis (prevents recurrence)
- For severe/necrotizing gallstone pancreatitis, timing of cholecystectomy must be individualized (usually deferred until resolution of acute inflammation)
Hypertriglyceridemia
- Aggressively lower triglycerides; insulin infusion and/or plasmapheresis may be needed
Alcohol-related AP
- Treat withdrawal prophylactically; counsel regarding cessation
8. Local Complications
Classification of Fluid Collections
| Timing | Content | Sterile | Infected |
|---|---|---|---|
| <4 weeks (no wall) | Fluid | Acute pancreatic fluid collection (APFC) | Infected APFC |
| <4 weeks (no wall) | Solid ± fluid | Acute necrotic collection (ANC) | Infected ANC |
| >4 weeks (defined wall) | Fluid | Pseudocyst | Infected pseudocyst |
| >4 weeks (defined wall) | Solid ± fluid | Walled-off necrosis (WON) | Infected WON |
Schwartz's Principles of Surgery, p. 1471
Management of Necrotizing Pancreatitis
- Sterile necrosis: conservative management; most resolves without intervention
- Infected necrosis (peaks at 3-4 weeks): step-up approach
- Percutaneous or endoscopic drainage first
- If drainage fails: minimally invasive necrosectomy (video-assisted retroperitoneal debridement - VARD, or endoscopic transluminal necrosectomy)
- Open necrosectomy reserved for failure of minimally invasive approaches
- Necrotizing AP carries >50% median rate of organ failure; mortality rises to ~50% with multi-organ failure
Pseudocyst
- Most resolve spontaneously
- Drainage indicated if: symptomatic, enlarging, infected, causing biliary/gastric obstruction
- Preferred: endoscopic transgastric or transduodenal drainage (EUS-guided)
Pancreatic Duct Disruption
- Presents as pancreatic ascites (high amylase in ascitic fluid) or enlarging fluid collection
- Confirmed by MRCP or ERCP
- Bridging pancreatic stent placement >90% effective; non-bridging stents less effective (25-50%)
9. Systemic Complications and Organ Support
| System | Complication | Management |
|---|---|---|
| Respiratory | ARDS, pleural effusion, atelectasis | O2, mechanical ventilation if needed |
| Cardiovascular | Hypotension, hypovolemia | Aggressive fluids, vasopressors/inotropes |
| Renal | Oliguria, AKI | Fluids, hemofiltration/dialysis |
| Hematologic | DIC | Supportive, FFP/platelets |
| Metabolic | Hyperglycemia, hypocalcemia | Insulin, IV calcium gluconate |
| Vascular | Splenic vein thrombosis, pseudoaneurysm | Angiography + embolization for bleeding |
10. Summary: Early Management of Severe AP (Bailey & Love, Table 72.4)
- Admit to HDU/ICU
- IV analgesics
- Aggressive fluid resuscitation with LR
- Supplemental oxygen
- Invasive monitoring (vital signs, CVP, urine output, blood gases)
- Frequent lab monitoring (LFTs, renal, clotting, Ca2+, glucose)
- Nasogastric tube only if vomiting
- Antibiotics if cholangitis or proven infection
- CECT if organ failure, deterioration, or sepsis signs
- ERCP within 72 h for severe gallstone pancreatitis or cholangitis
- Enteral (nasogastric) nutrition when nutritional support required
- Organ-specific supportive therapy (inotropes, ventilation, hemofiltration)
11. Follow-Up and Discharge Planning
- Screen for diabetes mellitus (endocrine insufficiency)
- Screen for exocrine pancreatic insufficiency (steatorrhea, weight loss)
- Assess for recurrent cholangitis or infected fluid collections
- Identify and address the underlying etiology to prevent recurrence (25% of patients experience at least one recurrence)
- Alcohol cessation counseling for alcohol-related AP
- Interval cholecystectomy for gallstone-related AP if not done during admission
Key references:
- Harrison's Principles of Internal Medicine, 22nd ed. (2025) - Chapter 359, pp. 2790-2793
- Schwartz's Principles of Surgery, 11th ed. - Chapter 33, pp. 1471-1472
- Bailey and Love's Short Practice of Surgery, 28th ed. - Table 72.4
- iLATAM-AP 2026 Guidelines - Ibero-Latin American Acute Pancreatitis Guidelines (PMID 42216617, June 2026)
This is a shared conversation. Sign in to Orris to start your own chat.