Dandy Walker syndrome
Reading File
Finding Sources
Searching PubMed
"Dandy-Walker" syndrome malformation
Searching the Web
Dandy Walker syndrome pathology clinical features management 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Dandy-Walker Syndrome (DWS)
Definition & Overview
Dandy-Walker syndrome is a posterior fossa malformation characterized by a spectrum of congenital hindbrain anomalies. The classical triad consists of:
- Cystic dilatation of the fourth ventricle (which balloons into a large posterior fossa cyst)
- Aplasia or hypoplasia of the cerebellar vermis (with upward rotation of the vermian remnant)
- Enlarged posterior fossa with elevation of the tentorium and torcula (torcular herophili)
It is part of a broader spectrum - the Dandy-Walker complex - that ranges from the full malformation down to Dandy-Walker variant and mega cisterna magna. The condition is also known as Dandy-Walker malformation (DWM).
- Bradley and Daroff's Neurology in Clinical Practice, Grainger & Allison's Diagnostic Radiology, Creasy & Resnik's Maternal-Fetal Medicine
Epidemiology & Pathogenesis
- Incidence: ~1:30,000 births; accounts for 4-12% of all cases of infantile hydrocephalus
- Pathogenesis: Results from developmental arrest in the hindbrain occurring between 4 and 6 weeks of gestation
- The posterior fossa fails to develop normally: the fourth ventricle fails to open properly (particularly the foramen of Magendie), leading to cystic ballooning and vermian aplasia
- Associated heterotopia of the inferior olivary nuclei, pachygyria of the cerebral cortex, and other cerebral anomalies can co-occur
The Dandy-Walker Spectrum
| Entity | Features |
|---|---|
| Classic DWM | All three features: large posterior fossa, fourth ventricle cyst, vermian aplasia/hypoplasia |
| DW Variant (DWV) | Cystic posterior mass + variable vermian hypoplasia, but NO enlargement of posterior fossa |
| Blake Pouch Cyst | Posterior membranous area of fourth ventricle roof fails to perforate; vermis and hemispheres usually normal |
| Mega Cisterna Magna | Incidental infracerebellar CSF collection; normal cerebellum and fourth ventricle - clinically insignificant |
MRI Appearance
The images below are from Grainger & Allison's Diagnostic Radiology (Fig. 76.7):
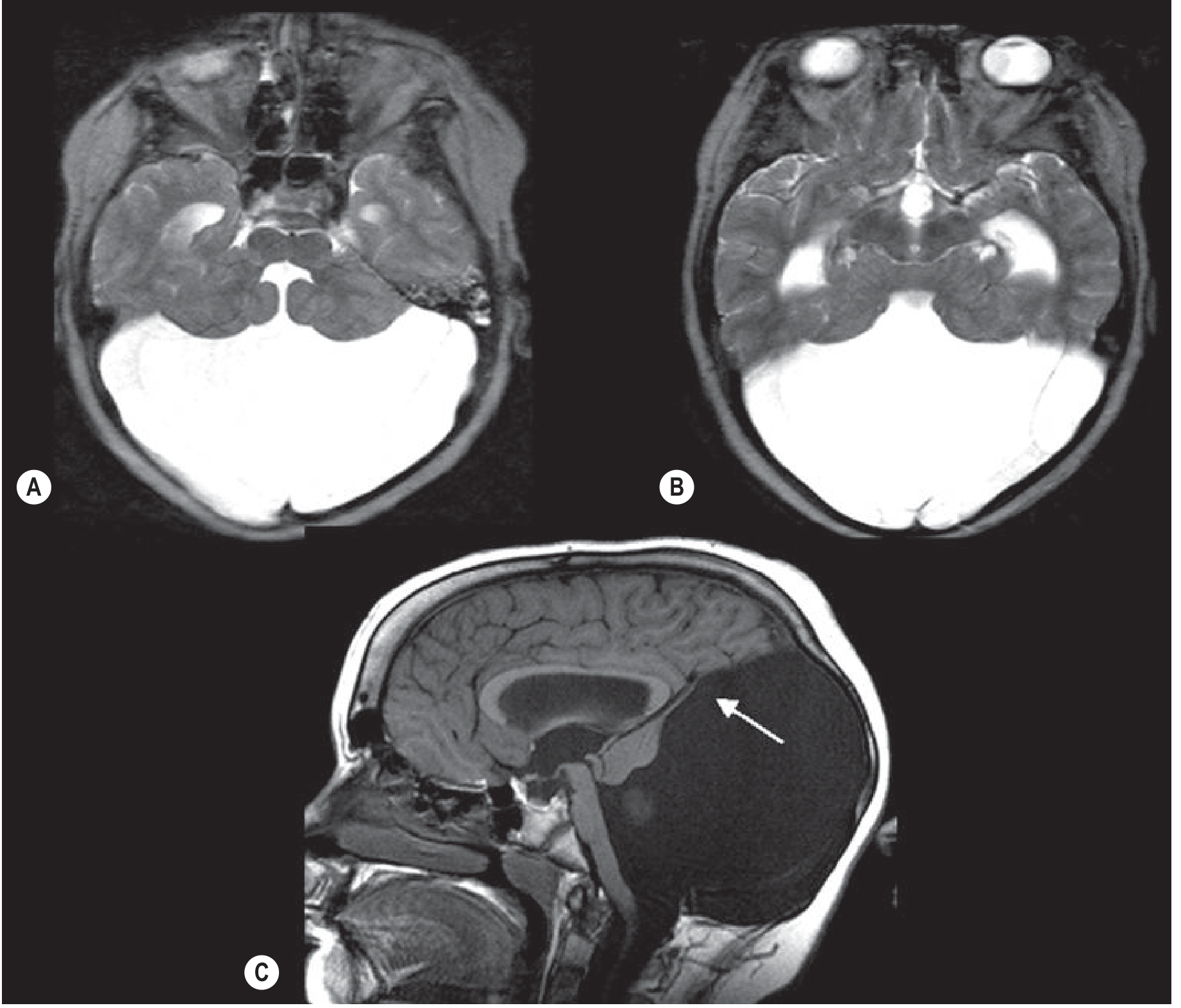
(A & B) Axial MRI: Fourth ventricle opens into a large posterior fossa cyst with associated hydrocephalus. (C) Sagittal MRI: Hypoplastic cerebellum with only a thin rim of cerebellar tissue forming the cyst wall (arrow); vein of Galen, straight sinus, and venous confluence are elevated above the lambdoid suture.
Key radiological signs:
- Large posterior fossa cyst continuous with the fourth ventricle
- Absent or hypoplastic vermis with upward rotation
- Cerebellar hemispheres splayed apart
- Elevated tentorium and torcula (torcula above the lambdoid suture - visible on plain X-ray, CT, and MRI)
- Hydrocephalus with dilatation of the aqueduct and lateral/third ventricles
Associated Anomalies
Present in 60% of prenatally diagnosed cases and 50-70% in postnatal series. These significantly influence prognosis:
CNS anomalies (most common):
- Hydrocephalus (70-80%)
- Agenesis or dysgenesis of the corpus callosum
- Holoprosencephaly
- Cephaloceles
- Cortical migration disorders (heterotopias, lissencephaly)
Non-CNS anomalies:
- Congenital heart disease
- Craniofacial, renal, limb, and abdominal wall anomalies
- Diaphragmatic hernia
- Ambiguous genitalia
- Fetal growth restriction
Chromosomal anomalies:
- Trisomy 9, 21, 18, 13; triploidy; 6p and 3q22-q24 deletion
Genetic syndromes:
- Walker-Warburg syndrome (congenital muscular dystrophy)
- Joubert syndrome (ciliopathy)
- Meckel-Gruber syndrome
- Some lissencephaly types (tubulopathies)
Clinical Features
Symptoms typically appear by age 1, though neonates may be asymptomatic at birth:
- Macrocephaly (if severe ventriculomegaly present at birth)
- Signs of raised intracranial pressure: bulging fontanelle, prominent scalp veins, "sunsetting" eyes
- Motor deficits: delayed motor development, hypotonia, ataxia, spastic diplegia
- Developmental delay / intellectual disability (approximately half of survivors)
- Seizures
- Associated structural findings (spastic diplegia and intellectual disability relate more to associated brain malformations than to the hydrocephalus itself)
Diagnosis
Prenatal (ultrasound/MRI):
- Large cisterna magna communicating with fourth ventricle
- Absent or hypoplastic vermis
- Cerebellar hemispheres splayed
- Elevated tentorium and torcular herophili
- Ventriculomegaly
Key differential diagnoses:
- Posterior fossa arachnoid cyst (does NOT communicate with fourth ventricle)
- Blake pouch cyst
- Mega cisterna magna
- Isolated vermian hypoplasia
- Joubert syndrome (molar tooth sign)
Management
Antenatal
- Detailed anatomic survey + fetal neurosonography
- Fetal echocardiography
- Genetic counseling; karyotype + microarray studies
- Fetal MRI (to exclude associated anomalies)
- Consultation: maternal-fetal medicine, neonatology, pediatric neurology
- Serial scans to monitor ventriculomegaly progression
Obstetric
- Vaginal delivery is not contraindicated
- Cesarean for routine obstetric indications or macrocephaly
- Cephalocentesis can decompress the head for vaginal delivery in severe hydrocephaly
Postnatal
- Neonatal head ultrasound + MRI to confirm prenatal findings
- Ventriculoperitoneal (VP) shunt - treatment of choice for progressive hydrocephalus (present in 80% by 3 months)
- Some centers use endoscopic third ventriculostomy + cyst fenestration as an alternative to shunting
- Genetic testing if not done prenatally
- Pediatric neurology consultation
- Multidisciplinary rehabilitation (physiotherapy, occupational therapy, special education)
Prognosis
- Intrauterine fetal demise: ~14%
- Infant mortality: 10-66% overall
- Isolated DWS: ~37% mortality
- With multiple malformations: ~63% mortality
- Two or more affected organ systems: 6x higher mortality than isolated DWS
- 80% develop hydrocephalus by 3 months
- Major causes of death: infection, uncontrolled hydrocephalus, shunt complications
- Neurodevelopmental outcomes: Up to one-third of survivors can develop normally. Favorable outcome is associated with: no associated CNS/extra-CNS anomalies and a normal lobulated vermis
Recent Literature
A 2025 updated literature review (Ocampo-Navia et al., Child's Nervous System) and a 2025 systematic review and meta-analysis on fetal posterior fossa anomalies (Parisi et al., Ultrasound Obstet Gynecol) confirm that outcomes are strongly influenced by the presence of associated anomalies and that neurodevelopmental prognosis remains heterogeneous. The bibliometric analysis by Alrefaie et al. (2024) highlights surgical management of hydrocephalus and prenatal diagnosis as dominant research areas.
This is a shared conversation. Sign in to Orris to start your own chat.