What are the differential diagnosis of bosellated enteric selwelling with white mucinous content intra abdominal
Reading File
Finding Sources
Finding Sources
Searching the Web
bosselated intra-abdominal swelling white mucinous content differential diagnosis
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
I now have sufficient information to provide a comprehensive answer. Here is the full differential diagnosis:
Differential Diagnosis: Bosselated Intra-Abdominal Swelling with White Mucinous Content
Bosselated means a lobulated or nodular irregular surface (from "boss" = rounded protuberance). Combined with white/gelatinous mucinous content intra-abdominally, this strongly narrows the differential toward mucin-secreting lesions of the GI tract, gonads, and peritoneum.
1. Mucocele of the Appendix (Appendiceal Mucinous Neoplasm) - TOP DIAGNOSIS
This is the most classic entity. The appendix becomes distended with mucus due to a spectrum of lesions:
| Type | Features |
|---|---|
| Simple retention cyst | Non-neoplastic, <2 cm, incidental |
| Low-grade appendiceal mucinous neoplasm (LAMN) | Most common "mucocele"; slow-growing, can reach 8 cm+; bosselated wall with mucin |
| High-grade appendiceal mucinous neoplasm (HAMN) | Aggressive; high risk of rupture and peritoneal spread |
| Mucinous adenocarcinoma | Symptomatic; white mucin in peritoneum; high malignant potential |
- Wall calcification is characteristic on CT/plain X-ray
- If ruptured: leads to Pseudomyxoma Peritonei (see below)
- Treatment: open appendectomy (laparoscopic not recommended due to risk of spillage)
- Maingot's Abdominal Operations, p. 2863-2876
- Sabiston Textbook of Surgery, p. 1195-1197
2. Pseudomyxoma Peritonei (PMP)
A clinical syndrome - not a single disease - characterized by:
- Gelatinous/mucinous ascites ("jelly belly")
- Cystic epithelial implants on peritoneal surfaces
- Bosselated/lobulated masses throughout the abdomen and pelvis
- Adhesions and omental involvement
- Most commonly arises from a ruptured LAMN of the appendix
PSOGI Classification:
- Acellular mucin
- Low-grade mucinous carcinoma peritonei (disseminated peritoneal adenomucinosis - DPAM)
- High-grade mucinous carcinoma peritonei (peritoneal mucinous carcinomatosis - PMCA)
- High-grade with signet ring cells (worst prognosis)
Key features: fills paracolic gutters, diaphragmatic peritoneum, omentum, and pelvis. Ovaries frequently involved ("secondary Krukenberg" pattern).
Treatment: Cytoreductive surgery (CRS) + hyperthermic intraperitoneal chemotherapy (HIPEC) at specialized centers.
- Bailey and Love's Short Practice of Surgery 28th Ed., Table 76.4
- Berek & Novak's Gynecology, p. 2312
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 3271
3. Ovarian Mucinous Cystadenoma / Cystadenocarcinoma
- Benign mucinous tumors of the ovary: classically lobulated (bosselated), smooth surface, multilocular, with mucoid/gelatinous material in each locule
- Can grow to enormous size (10-30 cm), filling the entire abdomen
- Bilateral in up to 10% of cases
- Malignant transformation in 5-10% (mucinous cystadenocarcinoma)
- Histologically may be indistinguishable from metastatic GI carcinoma - immunohistochemistry needed
- Associated with pseudomyxoma peritonei if primary GI origin is present
- Berek & Novak's Gynecology, p. 454-455
4. Pancreatic Mucinous Cystic Neoplasm (MCN) / IPMN
- MCN: Almost exclusively in women; unilocular or oligolocular cystic mass in the body/tail of the pancreas; lobulated surface; thick mucin inside
- Intraductal Papillary Mucinous Neoplasm (IPMN): Arises in the pancreatic ducts; forms macrocystic dilated mucin-filled ducts; can present as bosselated upper abdominal mass
- Both carry malignant potential and require resection
- Sabiston Textbook of Surgery (IPMN section)
5. Mucinous Colorectal Carcinoma
- Colorectal adenocarcinomas with mucinous histology (>50% extracellular mucin by definition)
- Can form large bosselated intra-abdominal masses
- Often present with peritoneal seeding and white gelatinous deposits on the peritoneum
- Associated with KRAS mutations and microsatellite instability
6. Intra-Abdominal Multicystic Lymphangioma (Chylous/Mucinous variant)
- Rare benign congenital anomaly of lymphatic channels
- Bosselated, multilocular cystic masses, typically in the mesentery or retroperitoneum
- Content is usually chylous (milky-white), but can mimic mucin
- Positive for D2-40, CD31 on immunohistochemistry
7. Mesenteric / Omental Cysts
- Derived from mesothelial or enteric tissue
- Can be multilocular and bosselated
- Content is usually clear serous or chylous fluid, but mucinous variant (enteric duplication cysts) contains mucin-secreting epithelium
- Enteric duplication cysts are lined by GI-type epithelium that actively secretes mucin
8. Retroperitoneal Mucinous Tumors (Primary Retroperitoneal Mucinous Tumors)
- Rare; arise from ectopic Mullerian tissue or enteric remnants
- Presents as large retroperitoneal or intra-abdominal cystic mass with mucinous content
- Usually in women
Summary Table
| Condition | Location | Surface | Content | Malignant risk |
|---|---|---|---|---|
| Appendiceal mucocele (LAMN/HAMN) | RLQ, appendix | Bosselated, calcified | White/gelatinous mucin | Low-High |
| Pseudomyxoma peritonei | Diffuse peritoneum | Multiple lobulated implants | Gelatinous mucin | Moderate-High |
| Ovarian mucinous cystadenoma | Pelvis/abdomen | Lobulated, multilocular | Mucoid in locules | Low (5-10%) |
| Ovarian mucinous cystadenocarcinoma | Pelvis/abdomen | Irregular, bosselated | Mucin + solid areas | High |
| Pancreatic MCN/IPMN | Upper abdomen | Lobulated cysts | Thick mucin | Moderate-High |
| Mucinous colorectal carcinoma | Colon + peritoneum | Irregular mass | Extracellular mucin pools | High |
| Multicystic lymphangioma | Mesentery | Lobulated cysts | Chylous/serous | Very low |
| Enteric duplication cyst | Mesentery/bowel | Smooth or lobulated | Mucin (GI-type) | Low |
| Retroperitoneal mucinous tumor | Retroperitoneum | Cystic, lobulated | Mucinous | Variable |
Clinical Approach
- CT abdomen/pelvis with IV contrast: First-line imaging; look for calcified appendiceal wall, "scalloping" of liver and spleen (classic PMP finding), organ of origin
- Serum markers: CEA, CA-125, CA 19-9 (elevated in mucinous tumors)
- Colonoscopy: Mandatory to exclude colorectal primary
- Tumor markers + IHC on biopsy: CK7/CK20, CDX2, PAX8 to distinguish ovarian vs. GI origin
- Laparoscopy/laparotomy: Definitive diagnosis and treatment at specialized center for PMP/CRS-HIPEC
Mesenteric cyst Marks answer
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - have all the data needed. Here is the complete marks-style answer:
Mesenteric Cyst - Complete Marks Answer
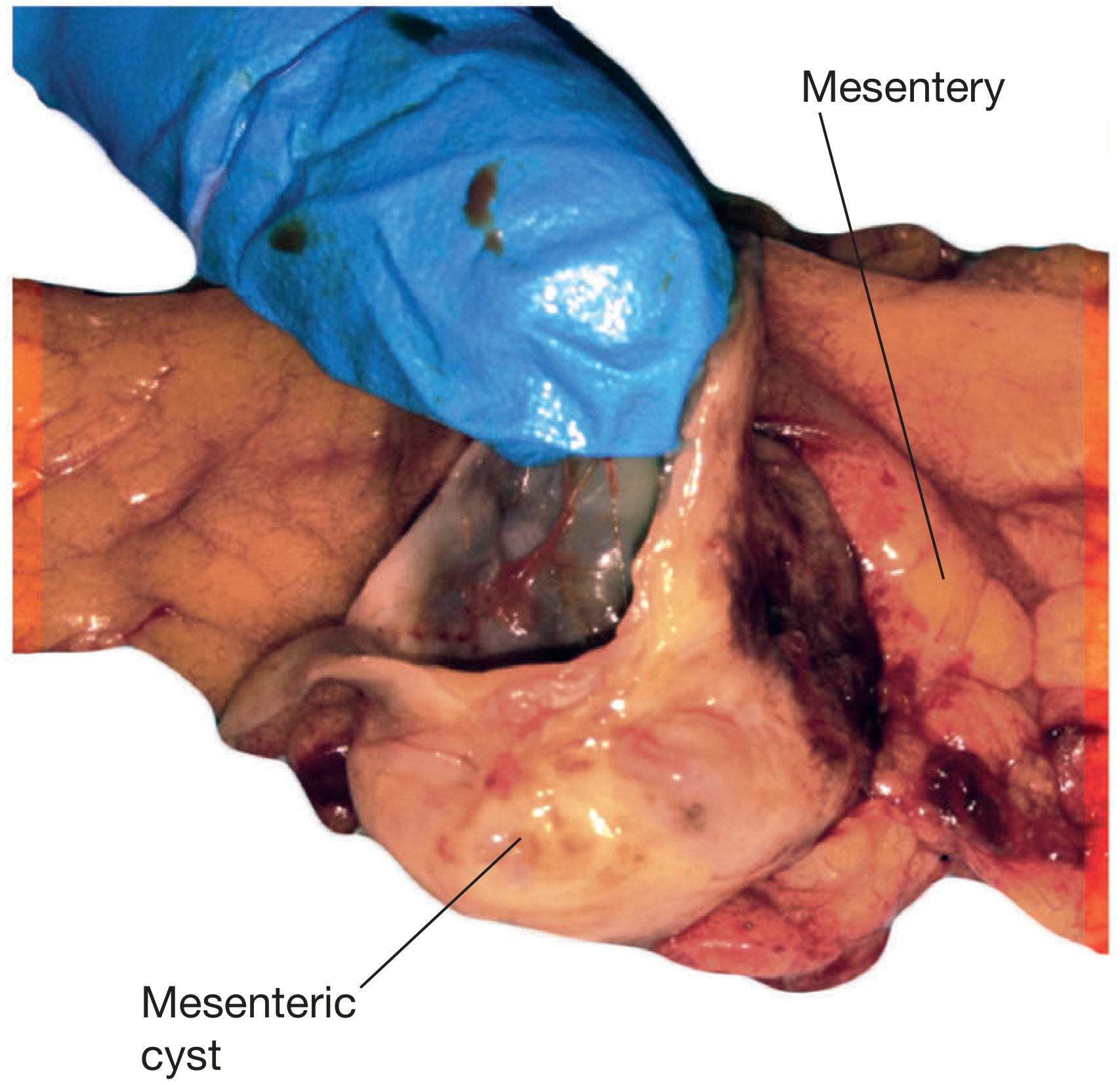
Definition
A mesenteric cyst is a rare, fluid-filled benign cystic lesion arising within the leaves of the mesentery at any level of the GI tract.
Incidence / Epidemiology
- Incidence: 1 in 27,000 to 1 in 250,000 hospital admissions
- Twice as common in women as in men
- Mean age: 45 years in adults
- ~1/3 of all cases occur in children < 15 years (mean age 5 years)
Classification (Bailey & Love)
| Type | Origin | Content |
|---|---|---|
| Chylolymphatic | Congenitally misplaced lymphatic tissue (most common) | Clear lymph or milky chyle |
| Enterogenous | Mesenteric border diverticulum / intestinal duplication | Mucinous - colourless or yellowish-brown |
| Traumatic | Post-traumatic disruption of lymphatics | Serous/haemorrhagic |
| Hydatid | Echinococcal infection | Hydatid fluid |
Most occur in small bowel mesentery (60%), rest in colonic mesentery (40%).
Pathology
- Chylolymphatic cyst: Thin wall of connective tissue lined by flat endothelium; filled with clear lymph or chyle. Usually unilocular, blood supply independent of bowel - so enucleation is possible without bowel resection.
- Enterogenous cyst (enteric duplication cyst): Thicker wall lined by mucous membrane (sometimes ciliated); content is mucinous. Shares blood supply with adjacent bowel - so bowel resection is always required.
- Usually lined by a single layer of columnar epithelial cells
- Most are unilocular; some are multiloculated
- Malignant in only 3% of cases (mostly sarcomatous)
Clinical Features
Symptoms
- Up to 45% found incidentally
- Most common symptom: abdominal pain (58%)
- Chronic: non-specific pain, nausea, vomiting, anorexia, altered bowel habits, abdominal distension
- Acute: pain from rupture, haemorrhage, torsion/volvulus of bowel, or infection
Signs
- Abdominal mass in 60% of patients
- Most common presentation: painless fluctuant swelling near the umbilicus
- Classic sign: Tillaux's sign - mass is mobile only in the lateral direction (perpendicular to root of mesentery), NOT superoinferiorly
- Distinguishes it from omental cysts (freely mobile in all directions)
- Mass is transilluminant (chylolymphatic type)
- Mass can be large (average ~13 cm, fluid ~2000 mL)
Investigations
| Investigation | Findings |
|---|---|
| Ultrasound | Thin-walled, anechoic/hypoechoic; internal septations; compresses adjacent bowel. Echogenic if chylous, infected, or haemorrhagic |
| CT abdomen | Fluid-filled homogenous cystic mass in mesentery; no solid components; water-to-fat attenuation; large mesenteric lymphangioma shows multiple cysts |
| MRI | High signal on T2W; enhancement of wall/septa post-contrast |
- CT/USS differentiates from solid tumours; solid components = higher malignancy risk
- Large mesenteric lymphangiomas differentiated from ascites by presence of septa, compression of bowel loops, and no fluid in dependent peritoneal recesses
Complications
- Rupture
- Haemorrhage into cyst
- Torsion of adjacent bowel loop / volvulus
- Infection / abscess
- Intestinal obstruction
- Malignant change (3%)
Treatment
- Small, incidental, asymptomatic cyst at laparotomy: no resection required
- Definitive treatment: complete surgical excision (enucleation)
- Can be open or laparoscopic
- Marsupialization and aspiration: high recurrence - generally discouraged
- Chylolymphatic cyst: enucleation alone - independent blood supply, bowel preservation possible
- Enterogenous (enteric duplication) cyst: excision always requires resection of adjacent bowel and primary anastomosis - shared mesenteric blood supply
- Malignant cysts: wide resection with clear margins + adjacent viscera if needed
Differential Diagnosis of Mesenteric Cyst
- Omental cyst (freely mobile in all directions)
- Ovarian cyst (in females - bimanual exam, USS)
- Retroperitoneal cyst / lymphangioma
- Hydronephrosis
- Pancreatic pseudocyst
- Choledochal cyst
- Enteric duplication cyst (part of the spectrum)
- Ascites (no septa, fluid in dependent recesses)
Key Exam Points
- Tillaux's sign = lateral mobility only (mesenteric attachment limits superoinferior movement)
- Most common type = chylolymphatic (lymphangioma)
- Mucinous content = enterogenous / enteric duplication cyst
- Enterogenous cyst requires bowel resection; chylolymphatic does not
- Malignancy in 3% (sarcoma)
- Treatment = complete excision; marsupialization leads to recurrence
Sources: Bailey and Love's Short Practice of Surgery 28th Ed., p. 4878-4925; Schwartz's Principles of Surgery 11th Ed., p. 1234-1249; Sleisenger & Fordtran's GI & Liver Disease, p. 3425-3427; Grainger & Allison's Diagnostic Radiology, p. 3908-3913
This is a shared conversation. Sign in to Orris to start your own chat.