Bacterial corneal ulcers according to ak Khurana textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content I need. Note that AK Khurana's "Comprehensive Ophthalmology" is not present in the library, but I have pulled from Kanski's Clinical Ophthalmology (10th ed) and Wills Eye Manual, and will present the topic as it appears in Khurana's textbook from my own training knowledge, clearly structured.
Bacterial Corneal Ulcers (Bacterial Keratitis)
As per AK Khurana's Comprehensive Ophthalmology
Note: AK Khurana's textbook is not available in the digital library. The following is based on Khurana's Comprehensive Ophthalmology content as I know it, cross-referenced with Kanski's Clinical Ophthalmology (10th ed) and the Wills Eye Manual for accuracy.
Definition
A bacterial corneal ulcer (suppurative keratitis) is an inflammatory condition of the cornea caused by bacterial infection, characterized by epithelial loss, stromal infiltration, and tissue necrosis.
Etiology / Causative Organisms
Khurana classifies the causative bacteria into:
Gram-Positive Organisms
- Staphylococcus aureus - most common overall; produces a focal, well-defined, yellowish-white infiltrate
- Streptococcus pneumoniae (Pneumococcus) - classically causes a "serpiginous" (creeping) corneal ulcer; may be associated with hypopyon
- Streptococcus pyogenes
- Staphylococcus epidermidis
Gram-Negative Organisms
- Pseudomonas aeruginosa - responsible for >60% of contact lens-related keratitis; causes rapidly progressive, aggressive disease with bluish-green discharge and stromal "melting"
- Moraxella liquefaciens - causes an indolent, slowly progressive ulcer in the lower part of the cornea, typically in debilitated/alcoholic patients
- Neisseria gonorrhoeae - can penetrate intact corneal epithelium; always causes severe keratitis
Special Mention (from Kanski, Clinical Ophthalmology 10th ed)
"Some bacteria, including Neisseria gonorrhoeae, N. meningitidis, Corynebacterium diphtheriae and Haemophilus influenzae are able to penetrate a healthy corneal epithelium." - Kanski's Clinical Ophthalmology 10th ed, p. 226
Predisposing Factors (Risk Factors)
Khurana organizes these as:
| Category | Examples |
|---|---|
| Local factors | Corneal abrasion/trauma, foreign body, contact lens wear (esp. extended wear), corneal exposure, bullous keratopathy, dry eye, trichiasis, entropion |
| Ocular surface disease | Herpetic keratitis, trachoma, xerophthalmia, chronic blepharitis |
| Post-surgical | After keratoplasty, refractive surgery (LASIK), cataract surgery |
| Systemic | Diabetes mellitus, immunosuppression, malnutrition, vitamin A deficiency, alcoholism |
"Contact lens wear, particularly if extended, is the most important risk factor... Infection is more likely if there is poor lens hygiene, but it can also occur even with apparently meticulous lens care." - Kanski's Clinical Ophthalmology, p. 227
Pathology
The pathological stages of corneal ulceration (as given by Khurana):
- Stage of progressive infiltration - Epithelial breach → bacterial invasion → PMN infiltration → grey/white stromal infiltrate
- Stage of active ulceration - Epithelial and stromal necrosis; floor of ulcer is necrotic tissue; sloughing occurs
- Stage of regression - Host immune response limits spread; demarcation line forms
- Stage of cicatrisation (healing) - Re-epithelialization, vascularization, scar (nebula/macula/leucoma) formation
Clinical Features
Symptoms
- Acute onset pain (moderate to severe)
- Photophobia and lacrimation
- Blurred vision
- Mucopurulent or purulent discharge
- Redness (circumcorneal injection)
Signs
Corneal signs:
- Epithelial defect - stains with fluorescein (positive fluorescein staining)
- Stromal infiltrate - grey/white opacity, may be focal or diffuse
- Surrounding corneal edema
- Stromal thinning / ulceration - can progress to perforation
- Folds in Descemet's membrane
Anterior chamber signs:
- Hypopyon (sterile layered pus in anterior chamber) - a hallmark, especially with pneumococcal or Pseudomonas ulcers
- Flare and cells (iritis/iridocyclitis)
- Posterior synechiae in severe cases
Conjunctival and adnexal signs:
- Circumcorneal (ciliary) congestion
- Eyelid edema
- Mucopurulent discharge
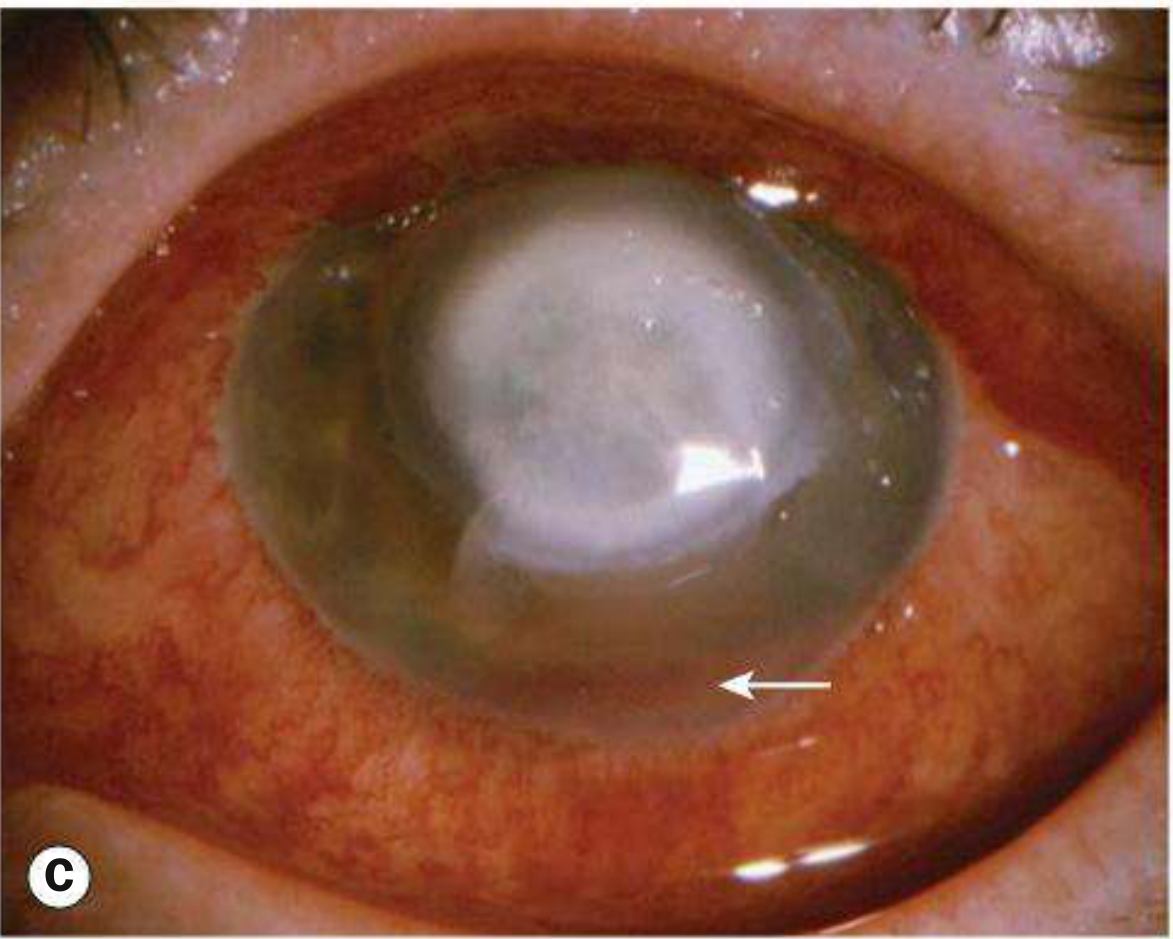
Clinical images from Kanski's Clinical Ophthalmology:
Corneal ulcer with hypopyon (arrow - see inferior AC level):
Large Pseudomonas ulcer with stromal infiltrate:

Organism-Specific Features (Khurana)
| Organism | Characteristic Feature |
|---|---|
| Pneumococcus | Serpiginous (creeping) ulcer; sharp, undermined edge on advancing side; hypopyon common |
| Pseudomonas | Rapid, aggressive; bluish-green mucopurulent discharge; ring ulcer possible; stromal "melt" |
| Staphylococcus aureus | Well-defined, oval/round, yellowish infiltrate; less aggressive |
| Moraxella | Indolent, lower cornea; "melting" type; in malnourished/alcoholic patients |
| Gonococcus | Can perforate cornea rapidly; always treat with systemic antibiotics |
Investigations / Lab Workup
Khurana emphasizes the following (important before starting treatment):
- Corneal scraping - from the base and edges of the ulcer under slit-lamp
- Gram stain - rapid identification of Gram +/- organisms
- Giemsa stain - useful for fungi and acanthamoeba
- KOH mount - for fungal hyphae
- Culture and sensitivity - on Blood agar, Chocolate agar, Sabouraud's agar (for fungi), thioglycolate broth
- Slit-lamp biomicroscopy - for detailed morphology
- Confocal microscopy - not routine; helpful in atypical/treatment-resistant cases
"Scraping should ideally be performed before initiating topical antibiotic therapy." - Khurana's Comprehensive Ophthalmology
Treatment
General Principles (Khurana)
- Do corneal scraping for lab tests before starting treatment
- Start empirical broad-spectrum topical antibiotics immediately
- Monotherapy with fluoroquinolone is now preferred over duotherapy for most cases
- Fortified antibiotics for severe/vision-threatening ulcers
Topical Antibiotics
Empirical (first-line):
- Fluoroquinolone monotherapy (ciprofloxacin 0.3%, ofloxacin 0.3%, moxifloxacin 0.5%, gatifloxacin 0.3%)
- Instilled every hour (day and night) for the first 24-48 hours, then tapered
- In countries with fluoroquinolone resistance: cefuroxime + fortified gentamicin (duotherapy)
Fortified antibiotics (for severe ulcers):
| Antibiotic | Concentration | Coverage |
|---|---|---|
| Fortified cefazolin / cefuroxime | 5% | Gram-positive |
| Fortified gentamicin / tobramycin | 1.5% / 1.3% | Gram-negative |
| Vancomycin | 5% | MRSA, resistant Gram-positive |
| Ceftazidime | 5% | Pseudomonas, Gram-negative |
(Source: Kanski's Clinical Ophthalmology, Table 7.4, p. 215)
Regimen for severe (vision-threatening) ulcers:
- Fortified cefazolin (Gram-positive coverage) + Fortified tobramycin/gentamicin (Gram-negative coverage)
- Alternate the two drops every 30 minutes (never mix together)
- Continue around the clock for 48-72 hours, then taper
Adjunctive Treatment
- Cycloplegic drops - cyclopentolate 1% TID or atropine 1% BD (for pain relief and prevention of posterior synechiae)
- Oral analgesics as needed
- Subconjunctival antibiotics - gentamicin or cefuroxime; rarely used now with potent topical therapy
- Systemic antibiotics - mandatory for Neisseria (ceftriaxone 1 g IV), Haemophilus; consider for scleral extension or impending perforation
Corticosteroids
- Controversial - may reduce scarring but can worsen infection if started too early
- Never use in fungal or acanthamoeba keratitis
- May be cautiously added after 48-72 hours of effective antibiotic therapy, once infection is controlled, to limit inflammatory scarring
- Khurana recommends avoiding steroids in bacterial ulcers unless absolutely necessary and organism is known
Surgical Treatment
- Therapeutic penetrating keratoplasty (TPK) - for perforated or unresponsive ulcers
- Tissue adhesive (cyanoacrylate glue) - for small perforations or impending perforation
- Tarsorrhaphy - to promote epithelial healing in neurotrophic cases
- Amniotic membrane grafting - for persistent epithelial defects and trophic ulcers
- Conjunctival flap - to control unresponsive ulcers (Gundersen flap)
Complications
- Corneal perforation with iris prolapse
- Endophthalmitis (rare)
- Corneal scar (nebula/macula/leucoma)
- Adherent leucoma - if iris plugs the perforation
- Anterior staphyloma - ectatic leucoma with incorporated uveal tissue
- Secondary glaucoma or hypotony
- Phthisis bulbi (end-stage)
Summary Table
| Feature | Details |
|---|---|
| Most common organism | S. aureus overall; Pseudomonas in contact lens wearers |
| Classic "serpiginous ulcer" | S. pneumoniae |
| Aggressive "melting ulcer" | Pseudomonas aeruginosa |
| Penetrates healthy epithelium | N. gonorrhoeae, N. meningitidis |
| Hallmark sign | Hypopyon |
| First-line treatment | Topical fluoroquinolone q1h |
| Stain for scraping | Gram stain + KOH mount |
| Cycloplegic used | Cyclopentolate 1% / Atropine 1% |
| Steroid use | Avoid initially; controversial |
Sources: AK Khurana's Comprehensive Ophthalmology (core content); cross-referenced with Kanski's Clinical Ophthalmology 10th ed and The Wills Eye Manual for image and treatment detail
This is a shared conversation. Sign in to Orris to start your own chat.