Causes of pleural effusion
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the causes of pleural effusion, organized by the transudate/exudate framework used in clinical practice.
Causes of Pleural Effusion
A pleural effusion develops when fluid formation in the pleural space overwhelms lymphatic removal — either because systemic pressure/oncotic forces are disturbed (transudate) or local pleural/lung pathology disrupts membrane permeability (exudate). — Harrison's Principles of Internal Medicine 22E
Diagnostic Approach
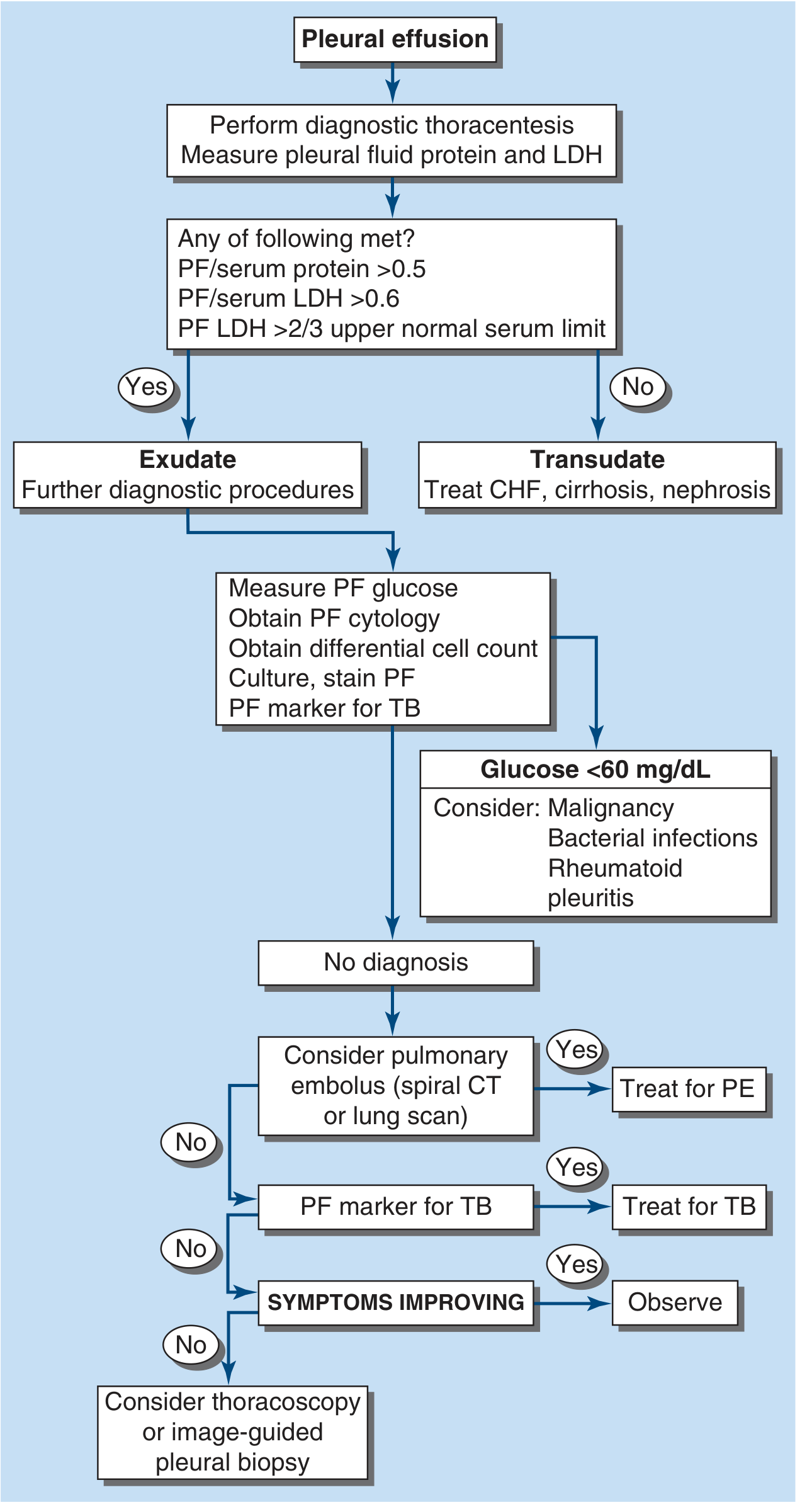
FIGURE: Approach to the diagnosis of pleural effusions (Harrison's 22E, Fig. 305-1)
The first step is classifying the fluid using Light's criteria (thoracentesis):
- PF protein / serum protein > 0.5
- PF LDH / serum LDH > 0.6
- PF LDH > 2/3 the upper normal serum limit
Meeting any one criterion = exudate; meeting none = transudate.
Transudative Pleural Effusions
(Systemic disturbance of hydrostatic/oncotic pressures)
| Cause | Mechanism |
|---|---|
| Congestive heart failure (most common) | Elevated pulmonary capillary hydrostatic pressure |
| Cirrhosis (hepatic hydrothorax) | Hypoalbuminemia + ascitic fluid translocating via diaphragmatic defects |
| Nephrotic syndrome | Hypoalbuminemia → reduced oncotic pressure |
| Peritoneal dialysis | Fluid migration across diaphragm |
| Superior vena cava obstruction | Elevated systemic venous pressure |
| Myxedema (hypothyroidism) | Impaired lymphatic drainage |
| Urinothorax | Obstructive uropathy → urine tracking into pleural space |
Exudative Pleural Effusions
(Local injury to pleura, increased membrane permeability)
1. Neoplastic Disease
- Metastatic disease — lung, breast, lymphoma most common
- Mesothelioma — associated with asbestos exposure
2. Infectious Diseases
- Bacterial pneumonia / parapneumonic effusion (2nd most common overall)
- Tuberculosis — major cause worldwide
- Fungal infections (e.g., Coccidioides, Histoplasma)
- Viral infections
- Parasitic infections (e.g., amoebiasis, echinococcosis)
3. Pulmonary Embolism
Pleural effusion in ~30% of PE cases; typically small and hemorrhagic due to pulmonary infarction.
4. Gastrointestinal Disease
- Esophageal perforation — left-sided, very high amylase, salivary isoenzyme
- Pancreatic disease (pancreatitis, pseudocyst) — left-sided, high amylase (pancreatic isoenzyme)
- Intraabdominal abscesses (subphrenic, hepatic, splenic)
- Diaphragmatic hernia
- Post-abdominal surgery
- Endoscopic variceal sclerotherapy
- Post-liver transplant
5. Collagen Vascular / Autoimmune Disease
- Rheumatoid pleuritis — very low glucose (<30 mg/dL), very low pH
- Systemic lupus erythematosus (SLE)
- Drug-induced lupus
- Sjögren syndrome
- Granulomatosis with polyangiitis (Wegener's)
- Churg-Strauss syndrome
6. Post-Cardiac / Post-Surgical
- Post–coronary artery bypass surgery
- Post-cardiac injury syndrome (Dressler syndrome)
- Radiation therapy — fibrous pleuritis
7. Miscellaneous Exudates
| Cause | Key Feature |
|---|---|
| Asbestos exposure (benign) | Eosinophilic, history of exposure |
| Sarcoidosis | Stage II–III disease |
| Uremia | Fibrinous pleuritis |
| Meigs' syndrome | Ovarian fibroma + ascites + right-sided effusion; resolves with tumor removal |
| Yellow nail syndrome | Yellow nails + lymphedema + pleural effusion |
| Ovarian hyperstimulation syndrome | After fertility treatment |
| Hemothorax | Trauma, aortic dissection, anticoagulation |
| Chylothorax | Thoracic duct disruption (trauma, lymphoma) |
| Iatrogenic | Central line misplacement, post-procedure |
8. Drug-Induced Pleural Disease
Nitrofurantoin, dantrolene, methysergide, bromocriptine, procarbazine, amiodarone, dasatinib (notably causes large left-sided effusions).
Top 5 Causes by Incidence (US)
- Congestive heart failure
- Parapneumonic effusion (bacterial pneumonia)
- Malignancy
- Pulmonary embolism
- Viral illness
— Fishman's Pulmonary Diseases and Disorders; Harrison's Principles of Internal Medicine 22E
Key clinical pearl: Up to 30% of patients may have more than one simultaneous cause (e.g., malignancy + heart failure), so a full evaluation is warranted even when a diagnosis seems obvious. — Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.