Physiology Homeostasis Active transport, passive transport Blood Plasma Erythropoiesis Urine formation Mechanisms of breathing Function of organs Function of brain and their parts Cardiac cycle Heart rate Types of muscle and their structure Anemia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here are comprehensive study notes covering all your topics, compiled from authoritative physiology textbooks (Guyton & Hall, Costanzo Physiology, Medical Physiology, Basic Medical Biochemistry, Morgan & Mikhail's Clinical Anesthesiology):
📚 Physiology Study Notes
1. HOMEOSTASIS
Definition: Homeostasis is the maintenance of a relatively stable internal environment (body fluids, temperature, pH, ion concentrations) despite external changes.
Key Principles:
- The body's internal environment = extracellular fluid (ECF) surrounding cells
- Maintained by negative feedback loops: a deviation from the set point triggers a corrective response that opposes the deviation
- Positive feedback amplifies a response (e.g., childbirth contractions, blood clotting)
- Effectors (organs, glands, muscles) make the corrective adjustments
- Control systems: nervous system (fast) and endocrine system (slow, sustained)
Examples:
- Blood glucose regulated by insulin/glucagon
- Body temperature regulated by sweating/shivering
- Blood pressure regulated by baroreceptor reflexes
- Blood pH maintained at 7.35–7.45
2. TRANSPORT MECHANISMS
Passive Transport
Movement of substances down their electrochemical gradient — no energy (ATP) required.
| Type | Mechanism |
|---|---|
| Simple diffusion | Small/lipid-soluble molecules cross directly through membrane (O₂, CO₂, ethanol) |
| Facilitated diffusion | Uses carrier proteins or channel proteins; no ATP (glucose into cells via GLUT transporters) |
| Osmosis | Water moves down its concentration gradient through aquaporins |
| Filtration | Bulk flow driven by hydrostatic pressure (e.g., glomerular filtration) |
Water is ALWAYS reabsorbed passively by osmosis in renal tubules.
Paracellular pathway: substances move between cells through tight junctions (claudins, occludins, JAMs).
Transcellular pathway: substances move through cells.
Active Transport
Movement of substances against their electrochemical gradient — requires ATP.
| Type | Mechanism | Example |
|---|---|---|
| Primary active transport | Directly coupled to ATP hydrolysis | Na⁺-K⁺ ATPase pump (3 Na⁺ out, 2 K⁺ in); H⁺ ATPase; Ca²⁺ ATPase |
| Secondary active transport | Driven by ion gradient created by primary pumps | Glucose reabsorption in proximal tubule (Na⁺-glucose cotransporter SGLT) |
The Na⁺-K⁺ ATPase is the most important pump — pumps 3 Na⁺ out and 2 K⁺ in per cycle, maintaining the resting membrane potential.
3. BLOOD
Definition: Blood is a connective tissue consisting of formed elements suspended in plasma.
Composition
- Total blood volume: ~5 L in adults
- Hematocrit: % of blood volume occupied by RBCs
- Males: ~45%, Females: ~40%, Newborn: ~55%
| Component | Description |
|---|---|
| Plasma | ~55% of blood volume; pale-white fluid |
| Red blood cells (Erythrocytes) | ~44%; carry O₂ via hemoglobin |
| White blood cells (Leukocytes) | Granulocytes, lymphocytes, monocytes; immunity |
| Platelets (Thrombocytes) | Clotting / hemostasis |
| Buffy coat | Thin layer of WBCs + platelets between RBCs and plasma |
4. PLASMA
Composition:
- Water (~92%)
- Plasma proteins (~7 g/dL total) — provide oncotic (colloid osmotic) pressure ~25 mmHg
- Electrolytes, nutrients (glucose, amino acids), hormones, waste products (urea, creatinine), dissolved gases
Major Plasma Proteins
| Protein | Level | Key Function |
|---|---|---|
| Albumin | 3.5–5.5 g/dL | Oncotic pressure, drug/hormone transport; synthesized by liver; half-life ~20 days |
| Globulins (α, β, γ) | Various | Immune function (IgG, IgM), transport (transferrin, lipoproteins) |
| Fibrinogen | 150–300 mg/dL | Clotting — converted to fibrin; synthesized only by liver |
| Clotting factors | Various | Coagulation cascade |
↓ Albumin occurs in hepatic cirrhosis; albumin synthesis is enhanced by low oncotic pressure.
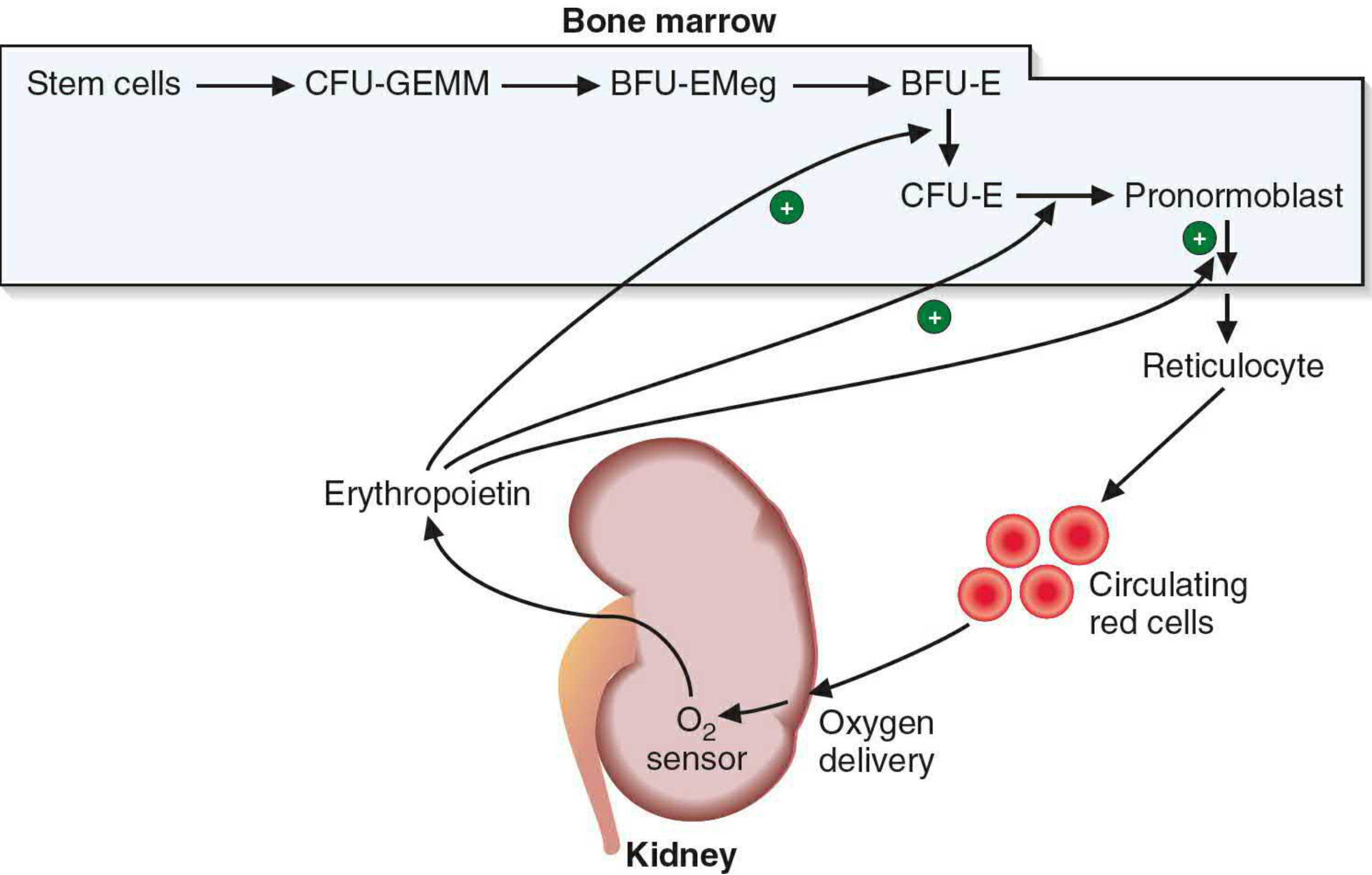
5. ERYTHROPOIESIS
Definition: The production of red blood cells (RBCs).
Stimulus: Reduced tissue oxygenation → kidneys release erythropoietin (EPO) → stimulates proliferation and maturation of erythroid progenitors in red bone marrow.
Developmental Sequence:
Pluripotent Stem Cell
↓
Mixed myeloid progenitor (CFU-GEMM)
↓
Burst-forming unit–erythroid (BFU-E)
↓
Colony-forming unit–erythroid (CFU-E)
↓
Normoblast (pronormoblast → basophilic → polychromatophilic → orthochromatic)
↓ ← nucleus extruded here
Reticulocyte (still has ribosomes + mRNA; synthesizes Hb; circulates 1–2 days)
↓ ← matures in SPLEEN
Mature Erythrocyte (biconcave disc, ~120-day lifespan)
Nutritional requirements: Iron, Vitamin B₁₂, Folate, Vitamin C, protein
- Iron deficiency → microcytic, hypochromic anemia
- B₁₂/Folate deficiency → megaloblastic (macrocytic) anemia
6. URINE FORMATION
Urine is formed by three processes in the kidney nephron:
Step 1 — Glomerular Filtration
- Blood is filtered at the glomerulus under hydrostatic pressure
- Filtrate contains water, ions, glucose, urea, creatinine (NOT proteins or cells normally)
- GFR = ~125 mL/min (~180 L/day filtered)
Step 2 — Tubular Reabsorption
Useful substances are reclaimed back into the blood:
- Proximal convoluted tubule (PCT): Reabsorbs ~65–70% of Na⁺, water, glucose (100%), amino acids, HCO₃⁻ via primary and secondary active transport
- Loop of Henle: Creates concentration gradient in medulla; descending limb permeable to water (osmosis); ascending limb impermeable to water, actively pumps NaCl
- Distal convoluted tubule (DCT): Na⁺ reabsorption regulated by aldosterone
- Collecting duct: Water reabsorption regulated by ADH (vasopressin)
Step 3 — Tubular Secretion
Waste products secreted from blood INTO tubule:
- H⁺, K⁺, drugs, creatinine, organic acids
Final urine: ~1–2 L/day, concentrated, containing urea, creatinine, excess ions
7. MECHANISMS OF BREATHING
Spontaneous (Active) Ventilation
Inspiration (active process):
- Diaphragm + external intercostals contract
- Thoracic cavity expands
- Intrapleural pressure drops: −5 → −8/−9 cm H₂O
- Alveolar pressure drops below atmospheric (becomes negative)
- Air flows in (down pressure gradient)
Expiration (passive at rest):
- Inspiratory muscles relax
- Elastic recoil of lungs + chest wall
- Intrapleural pressure returns to −5 cm H₂O
- Alveolar pressure rises above atmospheric
- Air flows out
Key formula:
P_transpulmonary = P_alveolar − P_intrapleural
Forced expiration uses internal intercostals + abdominal muscles (active).
Gas Exchange
- O₂ and CO₂ exchange by simple diffusion across the alveolar-capillary membrane down partial pressure gradients
- CO₂ is 20× more diffusible than O₂
- Ventilation-perfusion (V/Q) matching is critical for efficiency
8. FUNCTIONS OF KEY ORGANS
| Organ | Major Functions |
|---|---|
| Heart | Pumps blood; maintains circulation |
| Lungs | Gas exchange (O₂/CO₂); acid-base balance |
| Liver | Metabolism (CHO, fat, protein); detoxification; bile production; clotting factor synthesis; albumin synthesis |
| Kidneys | Filtration; urine formation; acid-base/electrolyte balance; BP regulation (renin); EPO secretion; vitamin D activation |
| Stomach | Mechanical + chemical digestion; HCl secretion; intrinsic factor (B₁₂ absorption) |
| Small intestine | Nutrient absorption (jejunum: sugars, AA, fats; ileum: B₁₂, bile salts) |
| Large intestine | Water/electrolyte absorption; feces formation |
| Pancreas | Exocrine: digestive enzymes (amylase, lipase, proteases); Endocrine: insulin, glucagon |
| Spleen | Filters old RBCs; immune surveillance; reticulocyte maturation |
| Thyroid | T₃/T₄ — metabolic rate, growth, development |
| Adrenal glands | Cortex: cortisol, aldosterone, androgens; Medulla: epinephrine, norepinephrine |
| Hypothalamus | Autonomic regulation; hormone releasing factors; thermoregulation; hunger/thirst |
| Pituitary | "Master gland" — GH, TSH, ACTH, FSH, LH, ADH (posterior), oxytocin (posterior) |
9. FUNCTIONS OF BRAIN AND ITS PARTS
| Brain Region | Key Functions |
|---|---|
| Cerebral Cortex | Higher cognition: thought, language, memory, voluntary movement, sensation, perception |
| Frontal lobe | Executive function, personality, voluntary motor control (motor cortex), Broca's area (speech production) |
| Parietal lobe | Somatosensory processing, spatial awareness, body image |
| Temporal lobe | Hearing, language comprehension (Wernicke's area), memory (hippocampus nearby) |
| Occipital lobe | Vision processing |
| Cerebellum | Coordination, balance, fine motor control, proprioception |
| Basal ganglia | Modulation of voluntary movement, procedural learning, habit formation |
| Thalamus | Relay station for sensory information to cortex (except olfaction) |
| Hypothalamus | Homeostatic control: temperature, hunger, thirst, sleep, circadian rhythm; links nervous to endocrine system |
| Hippocampus | Formation of new memories; spatial navigation |
| Amygdala | Emotions (fear, aggression), emotional memory |
| Brainstem | Contains midbrain, pons, medulla oblongata |
| — Midbrain | Visual/auditory reflexes; dopamine pathways (substantia nigra) |
| — Pons | Relay between cerebrum and cerebellum; respiratory regulation (pneumotaxic, apneustic centers) |
| — Medulla oblongata | Vital centers: cardiac center, vasomotor center, respiratory center; swallowing, coughing, vomiting reflexes |
| Spinal cord | Conducts sensory/motor signals; reflex arcs |
10. THE CARDIAC CYCLE
One complete cycle of contraction and relaxation (~0.8 sec at 75 bpm).
| Phase | Event | ECG | Valves | Heart Sound |
|---|---|---|---|---|
| A. Atrial Systole | Atria contract; final ventricular filling | P wave | — | S4 (abnormal) |
| B. Isovolumetric Ventricular Contraction | Ventricles contract; pressure rises; volume constant | QRS complex | Mitral closes | S1 ("lub") |
| C. Rapid Ventricular Ejection | Blood ejected to aorta/pulmonary artery; ventricular pressure peaks | ST segment | Aortic valve opens | — |
| D. Reduced Ventricular Ejection | Ejection slows; volume reaches minimum | T wave | — | — |
| E. Isovolumetric Ventricular Relaxation | Ventricles relax; pressure falls; volume constant | — | Aortic valve closes | S2 ("dub") |
| F. Rapid Ventricular Filling | Mitral opens; passive filling | — | Mitral opens | S3 (abnormal in adults) |
| G. Reduced Ventricular Filling (Diastasis) | Slow filling phase; cycle ends | — | — | — |
Key volumes:
- End-diastolic volume (EDV): ~130 mL (ventricle full)
- End-systolic volume (ESV): ~60 mL (after ejection)
- Stroke volume (SV): EDV − ESV = ~70 mL
- Ejection fraction (EF): SV/EDV = ~55–65%
11. HEART RATE
Normal resting heart rate: 60–100 bpm
Cardiac Output (CO) = Heart Rate (HR) × Stroke Volume (SV)
| Factor | Effect on HR |
|---|---|
| Sympathetic nervous system (norepinephrine, epinephrine) | ↑ HR (positive chronotropy) |
| Parasympathetic (vagus nerve) (acetylcholine) | ↓ HR (negative chronotropy) |
| SA node (sinoatrial node) | Natural pacemaker; fires 60–100/min |
| AV node | Backup pacemaker; 40–60/min |
| Bundle of His / Purkinje fibers | Backup; 20–40/min |
| Exercise | ↑ HR via sympathetic activation |
| High body temperature | ↑ HR |
| Hypoxia | Initially ↑ HR |
| Vagal stimulation (e.g. Valsalva) | ↓ HR |
Conduction pathway: SA node → AV node → Bundle of His → Left + Right bundle branches → Purkinje fibers → Ventricular myocardium
12. TYPES OF MUSCLE AND THEIR STRUCTURE
Three Types of Muscle
| Feature | Skeletal | Cardiac | Smooth |
|---|---|---|---|
| Location | Attached to bones | Heart wall | Walls of hollow organs (gut, vessels, bladder) |
| Control | Voluntary | Involuntary | Involuntary |
| Appearance | Striated | Striated | Non-striated |
| Nuclei | Multiple, peripheral | Single (or 2), central | Single, central |
| Cell junctions | None | Intercalated discs (gap junctions + desmosomes) | Gap junctions |
| Speed | Fast | Intermediate | Slow |
| Fatigue | Fatigable | Resistant (continuous) | Resistant |
| Regeneration | Limited (satellite cells) | Very limited | Good |
Skeletal Muscle Structure
- Muscle → Fascicles → Muscle fibers (cells) → Myofibrils → Sarcomeres
- Sarcomere = basic contractile unit (from Z line to Z line)
- A band (dark): thick filaments (myosin) + overlapping thin filaments
- I band (light): thin filaments (actin) only
- H zone: myosin only (no actin overlap)
- M line: anchors myosin
- Thin filaments: actin + tropomyosin + troponin complex (TnC, TnI, TnT)
- Thick filaments: myosin (heavy + light chains); myosin heads form cross-bridges
Muscle Fiber Types (Skeletal)
| Type | Speed | Metabolism | Fatigue | Use |
|---|---|---|---|---|
| Type I (slow-twitch, red) | Slow | Oxidative | Fatigue-resistant | Posture, endurance |
| Type IIa (fast-twitch, intermediate) | Fast | Oxidative + glycolytic | Intermediate | Sprinting, jumping |
| Type IIb/IIx (fast-twitch, white) | Fastest | Glycolytic | Fatigues quickly | Explosive bursts |
Extrafusal fibers = force-generating fibers (innervated by α motoneurons)
Intrafusal fibers = stretch receptors within muscle spindles (innervated by γ motoneurons)
Sliding Filament Theory of Contraction
- Action potential → motor end plate → ACh release → muscle AP
- Ca²⁺ released from sarcoplasmic reticulum (SR)
- Ca²⁺ binds troponin C → tropomyosin shifts → exposes actin binding sites
- Myosin head binds actin → power stroke (filaments slide, sarcomere shortens)
- ATP binds myosin → head detaches → returns to ready position
- Ca²⁺ resequestered into SR → relaxation
13. ANEMIA
Definition: Reduction in hemoglobin concentration, hematocrit, or RBC count below normal levels → reduced O₂-carrying capacity.
Classification by Mechanism
| Type | Cause | RBC Morphology |
|---|---|---|
| Iron deficiency | Low iron → ↓ heme synthesis | Microcytic, hypochromic |
| B₁₂ deficiency | ↓ DNA synthesis (requires B₁₂) | Macrocytic, megaloblastic |
| Folate deficiency | ↓ DNA synthesis | Macrocytic, megaloblastic |
| Hemolytic anemia | Premature RBC destruction | Variable (spherocytes, sickle cells) |
| Aplastic anemia | Bone marrow failure | Normocytic, pancytopenia |
| Anemia of CKD | EPO deficiency + chronic inflammation | Normocytic, normochromic |
| Sickle cell anemia (HbS) | Point mutation (Glu→Val in β-globin) | Sickle-shaped RBCs; hemolytic |
| Thalassemia | Reduced globin chain synthesis | Microcytic, target cells |
Iron-Deficiency Anemia (Most Common)
- Causes: blood loss, poor intake, malabsorption
- Labs: ↓ Hb, ↓ MCV, ↓ MCH, ↓ serum ferritin, ↑ TIBC
- Cells: small, pale (microcytic, hypochromic)
- RBCs continue dividing past the normal stopping point due to low hemoglobin → smaller cells
Megaloblastic Anemia (B₁₂/Folate)
- B₁₂/Folate required for thymidine synthesis → DNA replication impaired
- Nuclear division lags behind cytoplasmic maturation → large cells
- Nucleus extruded before enough divisions → macrocytes, hypersegmented neutrophils
Sickle Cell Anemia
- Autosomal recessive; HbS polymerizes when deoxygenated → sickle shape
- Causes vaso-occlusion (pain crises), hemolysis, organ damage
- Complication: pigmented gallstones (↑ unconjugated bilirubin from hemolysis)
Anemia of CKD
- EPO deficiency + functional iron deficiency + uremic inhibition of erythropoiesis
- Associated with left ventricular hypertrophy and cardiac failure
Quick Summary Table
| Topic | Key Point |
|---|---|
| Homeostasis | Maintained by negative feedback; internal environment stability |
| Passive transport | Down gradient; no ATP; includes diffusion, osmosis, facilitated diffusion |
| Active transport | Against gradient; needs ATP; Na⁺-K⁺ ATPase is primary example |
| Blood | 55% plasma + 45% RBCs; hematocrit ♂45% ♀40% |
| Plasma | Albumin, globulins, fibrinogen; oncotic pressure 25 mmHg |
| Erythropoiesis | Kidney EPO → bone marrow → stem cell → normoblast → reticulocyte → RBC |
| Urine formation | Filtration → reabsorption → secretion; aldosterone (Na⁺), ADH (H₂O) |
| Breathing | Inspiration active (diaphragm); expiration passive (elastic recoil) |
| Cardiac cycle | 7 phases; S1 = mitral closes; S2 = aortic closes; EF ~65% |
| Heart rate | SA node pacemaker; sympathetic ↑ HR; parasympathetic ↓ HR |
| Muscle types | Skeletal (voluntary, striated); Cardiac (involuntary, intercalated discs); Smooth (involuntary, non-striated) |
| Anemia | Iron def = microcytic; B₁₂/Folate = macrocytic; HbS = sickle cell; CKD = normocytic + EPO deficiency |
Sources: Guyton & Hall Textbook of Medical Physiology | Costanzo Physiology 7th Ed | Medical Physiology (Boron & Boulpaep) | Basic Medical Biochemistry 6e | Morgan & Mikhail's Clinical Anesthesiology 7e | Basic Medical Biochemistry
This is a shared conversation. Sign in to Orris to start your own chat.