investigations to be done in diarrhoea along with managemnt. with pharmacology
Diarrhoea: Investigations and Management with Pharmacology
Definition
- Acute diarrhoea: onset and duration <14 days (usually infectious)
- Persistent/chronic diarrhoea: >14 days (requires full evaluation)
Pathophysiology (Types of Diarrhoea)
| Type | Mechanism | Key Feature |
|---|---|---|
| Secretory | Increased Cl⁻/HCO₃⁻ secretion (e.g., cholera toxin, VIPoma) | Persists with fasting; stool pH >6; osmotic gap <50 |
| Osmotic | Unabsorbed solutes retain water (e.g., lactose intolerance, laxatives) | Stops with fasting; osmotic gap >125 |
| Inflammatory/Exudative | Mucosal damage with leukocytes/blood (e.g., IBD, Shigella) | Fever, blood/mucus in stool, fecal leukocytes positive |
| Motility | Rapid transit - reduced contact time | IBS, thyrotoxicosis, post-vagotomy |
| Malabsorptive | Fat/carbohydrate not absorbed | Steatorrhea, foul odour, weight loss |
INVESTIGATIONS
A. Bedside / Initial Screening Tests
| Test | Method | Purpose |
|---|---|---|
| Stool fecal leukocytes | Wright's or methylene blue stain | Identifies inflammatory diarrhoea (Shigella, Salmonella, C. difficile) |
| Fecal occult blood test (FOBT) | Immunochemical | Detects blood (dysentery, IBD, colorectal carcinoma) |
| Stool pH | pH determination | Low pH (<5.5) - carbohydrate malabsorption/lactose intolerance; laxative abuse |
| Fecal osmotic gap | 290 - 2×(fecal Na⁺ + fecal K⁺) | <50 = secretory; >125 = osmotic diarrhoea |
| Fecal fat (Sudan III stain / 72-hr collection) | Quantitative | Normal <7 g/day; >14 g suggests malabsorption; >32 g suggests pancreatic exocrine insufficiency |
| Fecal calprotectin / lactoferrin | Immunoassay | Marker of intestinal inflammation; elevated in IBD, infectious colitis |
B. Stool Microbiological Studies
| Test | Method | Detects |
|---|---|---|
| Stool culture & sensitivity | Culture, serotyping, NAAT | Salmonella, Shigella, Campylobacter, E. coli, Yersinia |
| C. difficile toxin A/B | NAAT (most sensitive), EIA | Antibiotic-associated/pseudomembranous colitis |
| Stool for ova and parasites | Concentration + stain + microscopy | Giardia, Entamoeba histolytica, Cryptosporidium, Cyclospora |
| Intestinal protozoa | Acid-fast stain, EIA, NAAT | Cryptosporidium, Isospora, Cyclospora (especially immunocompromised) |
| Viral gastroenteritis panel | EIA, NAAT | Rotavirus, Norovirus, Adenovirus, Astrovirus |
| Mycobacterium | Acid-fast stain + culture | TB enteritis, M. avium-intracellulare (HIV patients) |
| Electron microscopy | EM | Viral particles (special circumstance) |
C. Blood Investigations
| Test | Purpose |
|---|---|
| FBC (CBC) | Anaemia (blood loss, malabsorption), leukocytosis (infection/IBD), eosinophilia (parasites) |
| CRP / ESR | Inflammation marker |
| Serum electrolytes (Na⁺, K⁺, Cl⁻, HCO₃⁻) | Dehydration, electrolyte derangements (hypokalaemia in secretory diarrhoea) |
| Urea & Creatinine | Assess dehydration / prerenal AKI |
| Serum albumin | Protein-losing enteropathy, malnutrition |
| LFTs | Hepatitis, liver disease, cholestatic diarrhoea |
| Serum calcium, magnesium | Malabsorption; hypercalcaemia in sarcoidosis |
| TFTs (TSH, FT4) | Hyperthyroidism-related motility diarrhoea |
| HIV serology | EIA + Western blot; HIV enteritis, AIDS-related causes |
| Coeliac antibodies | Anti-tTG IgA, anti-endomysial IgA |
| Serum B12, folate, iron studies | Nutritional deficiencies from malabsorption |
D. Special/Hormonal Tests (Secretory/Endocrine Causes)
| Test | Purpose |
|---|---|
| Serum VIP (vasoactive intestinal peptide) | VIPoma (watery diarrhoea, hypokalaemia, achlorhydria) |
| Serum gastrin | Gastrinoma (Zollinger-Ellison syndrome) - diarrhoea in ~33% |
| 24-hr urine 5-HIAA or serum serotonin | Carcinoid syndrome |
| Serum calcitonin | Medullary carcinoma thyroid |
| Serum cortisol / ACTH | Adrenal insufficiency |
| Fasting serum 7αC4 or fecal bile acids | Bile acid diarrhoea (BAD) - elevated FGF-19 deficiency mechanism |
| Serum tryptase | Systemic mastocytosis |
E. Imaging
| Investigation | Indication |
|---|---|
| Abdominal X-ray | Toxic megacolon, obstruction, bowel dilatation |
| Abdominal Ultrasound | IBD, liver/biliary disease, pancreatic lesions |
| CT abdomen/pelvis (with contrast) | IBD, malignancy, mesenteric ischaemia, abscess, lymphadenopathy |
| Small bowel series / MR enterography | Crohn's disease, mucosal assessment |
| MRCP / ERCP | Pancreatic/biliary disease causing malabsorption |
F. Endoscopy
| Procedure | Indication |
|---|---|
| Flexible sigmoidoscopy | IBD (distal), C. difficile colitis, microscopic colitis |
| Colonoscopy + biopsy | Chronic diarrhoea, IBD, microscopic colitis, malignancy; essential in middle-aged/elderly with chronic bloody diarrhoea |
| Upper GI endoscopy + duodenal biopsy | Coeliac disease (villous atrophy), Giardia (duodenal aspirate), Whipple's disease |
| Capsule endoscopy | Small bowel mucosal disease |
G. Functional Tests (Chronic Diarrhoea)
- Hydrogen breath test - lactose/fructose malabsorption, small intestinal bacterial overgrowth (SIBO)
- SeHCAT scan (75Se-taurocholate) - bile acid malabsorption
- Secretin stimulation test - pancreatic exocrine insufficiency
- Faecal elastase - pancreatic insufficiency (non-invasive)
- D-xylose absorption test - small intestinal mucosal disease vs. luminal maldigestion
MANAGEMENT
Step 1: Assessment of Dehydration (WHO Classification)
| Degree | Features | Management |
|---|---|---|
| No dehydration | Normal | ORS at home; continue feeding |
| Some dehydration | 2 signs: restlessness, sunken eyes, thirst, poor skin turgor | ORS 75 mL/kg over 4 hours (Plan B) |
| Severe dehydration | All above + shock | IV Ringer's lactate 100 mL/kg (Plan C); 20 mL/kg bolus initially |
Step 2: Oral Rehydration Therapy (ORT) - Cornerstone
- Sodium: 75 mmol/L
- Chloride: 65 mmol/L
- Glucose (anhydrous): 75 mmol/L
- Potassium: 20 mmol/L
- Citrate: 10 mmol/L
- Osmolarity: 245 mOsm/L (reduced osmolarity)
- Mild (3-5% dehydration): 30-50 mL/kg over 4 hours
- Moderate (6-9%): 60-80 mL/kg over 4 hours
- Replace ongoing losses: 10 mL/kg per stool; 2 mL/kg per emesis
Step 3: Dietary Management
- Continue feeding - do NOT withhold food; age-appropriate diet
- BRAT diet (Banana, Rice, Applesauce, Toast) or soft diet
- Avoid lactose-containing products temporarily in acute gastroenteritis
- Zinc supplementation (10-20 mg/day for 10-14 days) in children in developing countries - reduces duration and severity
PHARMACOLOGY OF DIARRHOEA
1. Oral Rehydration Salts (ORS)
- Mechanism: Exploits intact Na⁺-glucose cotransport in small intestine enterocytes; water follows osmotically
- Remains effective even when electrogenic Na⁺ absorption is impaired
2. Antimotility Agents
Loperamide (Imodium)
- Class: Opioid receptor agonist (MOR - mu opioid receptor)
- Mechanism:
- Binds peripheral MOR on enteric neurons - reduces peristalsis
- Increases small intestinal and mouth-to-caecum transit time
- Increases anal sphincter tone
- Has antisecretory activity against cholera toxin and E. coli toxin (counters adenylyl cyclase stimulation via G-linked receptors)
- 40-50 times more potent than morphine as antidiarrhoeal; poorly crosses the BBB
- ADME: Oral (capsule/solution/chewable tablet); peak plasma at 3-5 hours; t½ ~11 hours; extensive hepatic metabolism
- Dose: Adults: 4 mg initially, then 2 mg after each loose stool; max 16 mg/day. Children: 2-5 yr: 3 mg/day max; 6-8 yr: 4 mg/day; 8-12 yr: 6 mg/day; not recommended <2 years
- Adverse effects: Constipation, abdominal bloating, nausea
- Contraindications: Bloody diarrhoea or suspected invasive bacterial diarrhoea (may mask infection, delay clearance, increase risk of systemic invasion); avoid in C. difficile colitis; caution in young children
Diphenoxylate + Atropine (Lomotil)
- Mechanism: Diphenoxylate is a synthetic opioid (MOR agonist); reduces GI motility. Atropine added in subtherapeutic dose to deter abuse
- Use: Acute/chronic non-inflammatory diarrhoea
- Penetrates CNS more than loperamide - more CNS side effects
Codeine phosphate
- Opioid with antidiarrhoeal and analgesic effects; used for refractory diarrhoea; risk of dependence
3. Antisecretory Agents
Bismuth Subsalicylate (Pepto-Bismol)
- Mechanism: Antisecretory + anti-inflammatory + antimicrobial effects; in stomach low pH forms bismuth oxychloride; clay component may adsorb toxins; salicylate component has anti-inflammatory activity
- Uses: Traveller's diarrhoea (prevention and treatment), acute gastroenteritis, non-ulcer dyspepsia
- Dose: 30 mL or 2 tablets every 30-60 min, up to 8 times/day; each dose contains ~262 mg each of bismuth and salicylate
- Adverse effects: Black stools (bismuth sulfide - not melena), black tongue; salicylate absorbed - carries Reye's syndrome warning in children; tinnitus, CNS effects
- Note: 99% of bismuth unabsorbed; salicylate is absorbed
Racecadotril (Acetorphan)
- Mechanism: Prodrug - converted to thiorphan, an enkephalinase inhibitor (NEP inhibitor). Inhibits breakdown of enkephalins → increased enkephalin activity → reduced cAMP-driven intestinal secretion via delta opioid receptors (DOR). Pure antisecretory - does not affect motility
- Advantage: Does not cause rebound constipation; preferred in children
- Use: Acute secretory diarrhoea, especially in children
4. Antibiotics (Empiric and Targeted)
- Moderate-to-severe traveller's diarrhoea
- Suspected bacterial dysentery (Shigella, Campylobacter)
- C. difficile colitis
- Giardia, Entamoeba histolytica
- Immunocompromised patients
- Enterohemorrhagic E. coli (EHEC/O157:H7) - risk of HUS
- Uncomplicated viral gastroenteritis
- Mild, self-limiting bacterial diarrhoea
| Antibiotic | Dose | Indication |
|---|---|---|
| Ciprofloxacin | 500 mg BD × 3 days | Traveller's diarrhoea (fluoroquinolone 1st-line); Salmonella, Shigella |
| Norfloxacin | 400 mg BD × 3 days | Traveller's diarrhoea |
| Levofloxacin | 500 mg OD × 3 days | Traveller's diarrhoea |
| Azithromycin | 500 mg/day × 1-3 days (or 1000 mg single dose) | Traveller's diarrhoea (alternative); Campylobacter; preferred in children (10 mg/kg, max 500 mg single dose); regions with fluoroquinolone resistance |
| Rifaximin | 200 mg TDS × 3 days | Traveller's diarrhoea (non-invasive E. coli); minimal systemic absorption; IBS-D |
| Rifamycin | 388 mg BD × 3 days | Traveller's diarrhoea (alternative) |
| Metronidazole | 400-500 mg TDS × 5-7 days | Giardia, Entamoeba histolytica, C. difficile (mild) |
| Vancomycin (oral) | 125 mg QDS × 10 days | C. difficile colitis (severe/recurrent) |
| Fidaxomicin | 200 mg BD × 10 days | C. difficile (preferred - lower recurrence) |
| Tinidazole | 2 g single dose | Giardia |
5. Probiotics
- Mechanism: Restore commensal microflora; compete with pathogens; modulate immune response
- Evidence-based strains:
- Lactobacillus GG - effective in acute infectious diarrhoea, antibiotic-associated diarrhoea
- Saccharomyces boulardii - effective in antibiotic-associated and infectious diarrhoea
- Uses: Antibiotic-associated diarrhoea, C. difficile (adjunct), acute gastroenteritis
6. Drugs for Specific Syndromes
Diarrhoea-Predominant IBS (IBS-D)
| Drug | Class | Mechanism | Dose |
|---|---|---|---|
| Alosetron | 5-HT3 antagonist | Blocks 5-HT3 receptors on enteric neurons → reduces colonic contractility, decreases transit, increases fluid absorption | 1 mg/day × 4 wks; max 1 mg BD. FDA restricted to women with severe IBS-D |
| Eluxadoline (Viberzi) | Mixed opioid receptor drug | MOR agonist + DOR antagonist + KOR agonist; reduces abdominal pain and diarrhoea without causing rebound constipation | 100 mg BD with food (gallbladder intact); 75 mg BD (no gallbladder) |
| Rifaximin | Non-absorbable antibiotic | Gut-restricted RNA polymerase inhibitor; reduces bacterial dysbiosis in IBS-D | 550 mg TDS × 2 weeks |
7. Anti-parasitic Drugs
| Drug | Parasite | Dose |
|---|---|---|
| Metronidazole | Giardia, E. histolytica | 400-500 mg TDS × 5-7 days |
| Tinidazole | Giardia | 2 g single dose (more effective) |
| Nitazoxanide | Cryptosporidium, Giardia | 500 mg BD × 3 days |
| Diloxanide furoate | E. histolytica (luminal - post-metronidazole) | 500 mg TDS × 10 days |
8. Zinc Supplementation
- WHO recommendation: 10 mg/day (<6 months); 20 mg/day (>6 months) for 10-14 days in children with acute diarrhoea
- Reduces severity, duration, and recurrence risk
Summary Algorithm
Acute Diarrhoea (<14 days)
├── Mild/No dehydration → ORS + continue diet + zinc (children)
├── Bloody/fever/severe → Stool culture + antibiotics (targeted)
├── Traveller's diarrhoea → Fluoroquinolone or Azithromycin
├── Antibiotic-associated → Check C. difficile; vancomycin/fidaxomicin
└── Suspected viral → Supportive only; no antibiotics
Chronic Diarrhoea (>14 days)
├── Osmotic gap → check for osmotic cause (dietary, laxative)
├── Fecal leukocytes/calprotectin ↑ → Colonoscopy; consider IBD
├── Steatorrhea → Malabsorption workup (biopsy, ERCP, breath tests)
├── Secretory (hormonal) → Serum VIP, gastrin, 5-HIAA, calcitonin
└── IBS-D → Loperamide / Alosetron / Eluxadoline / Rifaximin
- Henry's Clinical Diagnosis and Management by Laboratory Methods - Table 23.4 (Lab investigations)
- Harrison's Principles of Internal Medicine 22E - Chronic diarrhoea chapter
- Rosen's Emergency Medicine - Acute diarrhoea, dehydration management
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Antidiarrheal pharmacology (loperamide, bismuth, racecadotril, alosetron, eluxadoline, antibiotics)
- Goldman-Cecil Medicine - Postoperative diarrhoea, C. difficile
provide defenition, types, causes, pathology, diagnostic approach , management along with pharmacology for dysentry
Dysentery: Complete Clinical Guide
1. DEFINITION
- Stools are small in volume (not watery and large)
- Visible blood + mucus in stool
- Tenesmus - painful ineffectual urge to defecate
- Systemic features: fever, malaise, toxaemia
2. TYPES / CLASSIFICATION
A. By Causative Agent
| Type | Causative Organism |
|---|---|
| Bacillary (Shigellosis) | Shigella spp. - most common cause of epidemic dysentery |
| Amoebic dysentery | Entamoeba histolytica |
| Campylobacter dysentery | Campylobacter jejuni |
| Salmonella dysentery | Salmonella spp. (non-typhoidal) |
| E. coli dysentery | Enteroinvasive E. coli (EIEC); Enterohemorrhagic E. coli (EHEC/O157:H7) |
| Schistosomal dysentery | Schistosoma mansoni (bilharzial dysentery - endemic in Nile Delta and tropics) |
| C. difficile colitis | Clostridioides difficile (pseudomembranous colitis) |
B. By Duration
| Type | Duration |
|---|---|
| Acute | <2 weeks (usually bacterial) |
| Chronic/Recurrent | >2 weeks or recurring (usually amoebic or IBD) |
C. By Severity
| Mild | Moderate | Severe |
|---|---|---|
| Few bloody stools, low-grade fever | Multiple bloody stools, significant fever, tenesmus | Toxaemia, dehydration, complications (HUS, toxic megacolon) |
3. CAUSES (Aetiology)
Bacterial
| Organism | Notes |
|---|---|
| Shigella dysenteriae (Group A) | Most severe; produces Shiga toxin; can cause HUS |
| Shigella flexneri (Group B) | Common in developing countries; most studied |
| Shigella sonnei (Group D) | Common in industrialized countries; milder disease |
| Shigella boydii (Group C) | Rare; mainly in Indian subcontinent |
| Campylobacter jejuni | Most common bacterial enteric pathogen in high-income countries |
| Salmonella spp. | Invasive; associated with exudative bloody diarrhoea |
| EIEC / EHEC O157:H7 | EHEC especially dangerous - can cause HUS; antibiotics CONTRAINDICATED |
| Yersinia enterocolitica | Invades ileocaecal region; may mimic Crohn's disease/appendicitis |
Parasitic
| Organism | Notes |
|---|---|
| Entamoeba histolytica | Worldwide distribution; transmitted via contaminated water; chronic course; can cause liver abscess |
| Schistosoma mansoni | Bilharzial dysentery; rectal papillomas; fistulae-in-ano |
| Trichuris trichiura (heavy load) | Worm load causes dysentery, rectal prolapse |
Other
- Clostridioides difficile - Antibiotic-associated pseudomembranous colitis
- Ulcerative colitis - Non-infectious inflammatory cause of bloody diarrhoea mimicking dysentery
- Ischaemic colitis - Particularly in elderly
4. PATHOLOGY
A. Bacillary Dysentery (Shigella) - Detailed Pathogenesis
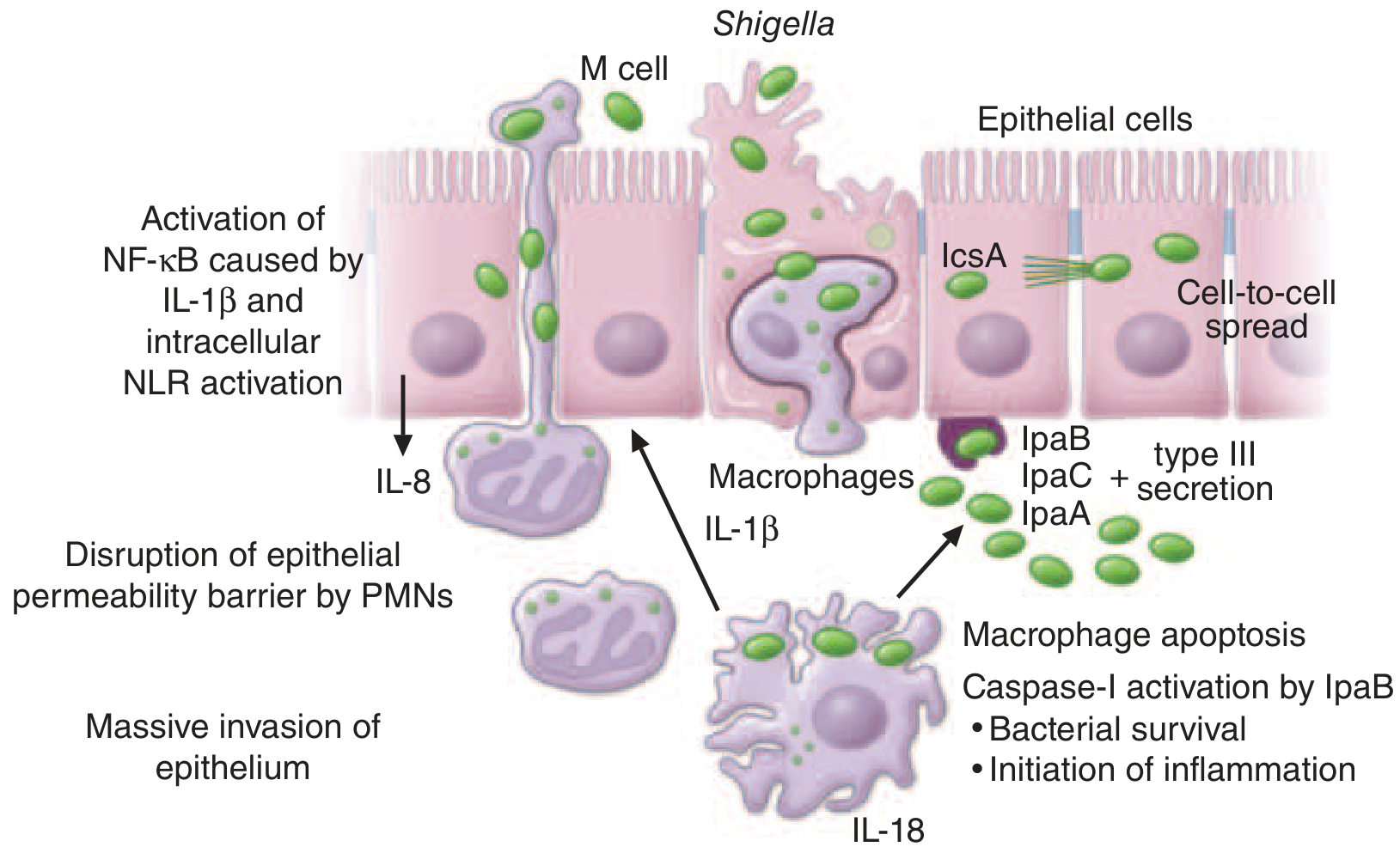
- Entry via M cells: Shigella selectively adheres to and transcytoses through follicle-associated M cells (lack brush border) overlying mucosal lymphoid nodules
- Macrophage apoptosis: Bacteria enter subepithelial macrophages, escape the phagosome, and activate caspase-1 via IpaB - inducing macrophage apoptosis (releases IL-18 and IL-1β)
- Basolateral invasion of enterocytes: Released bacteria contact the basolateral surface of enterocytes; Type III secretion system injects IpaA, IpaB, IpaC, IpaD proteins into the host cell
- Actin polymerization and intracellular spread: IcsA (VirG) protein on the bacterial surface recruits N-WASP to polymerize actin, propelling bacteria through cytoplasm and into neighbouring cells (cell-to-cell spread)
- Massive inflammatory response: Infected epithelial cells release IL-8, massively recruiting PMNs, which further destabilize the epithelial barrier, exacerbating inflammation
- NF-κB activation: Intracellular NLR (NOD-like receptor) activation + IL-1β drives NF-κB signalling → acute colitis
- Phase 1 (watery): Active secretion/abnormal water reabsorption in jejunum - due to enterotoxin ShET-1 and early mucosal inflammation
- Phase 2 (dysenteric): Colonic mucosal invasion - bloody, mucopurulent stools with tenesmus
- Acute purulent proctitis with multiple small shallow ulcers (bacillary dysentery - Bailey & Love)
- Edematous, hemorrhagic colonic mucosa
- Ulcerations with overlying exudates (pseudomembrane-like)
- Mainly affects distal colon and rectum
B. Amoebic Dysentery - Pathology
- Ingestion of cysts via contaminated water/food
- Cysts excyst in small intestine → trophozoites in large intestine
- Trophozoites invade colonic mucosa via proteolytic enzymes (cysteine proteases) and amoebapores (pore-forming peptides) → lysis of epithelial cells, goblet cells, and mucosal glands
- Flask-shaped (bottleneck) ulcers: Trophozoites burrow through epithelium, creating ulcers with markedly undermined edges and a yellow necrotic floor with blood and pus
- Trophozoites may be seen ingesting erythrocytes (erythrophagocytosis - pathognomonic)
- Distribution: mainly distal sigmoid colon and rectum; can involve entire colon
- Hepatic amoebiasis (liver abscess) - most common extraintestinal complication
- Amoeboma: granulation tissue mass (mimics colonic carcinoma)
- Toxic megacolon (0.5% of cases)
- Haemorrhage, stricture formation, perforation
- Pericolitis with adhesions → intestinal obstruction
- Intussusception and necrotizing colitis (in children)
5. CLINICAL FEATURES
Bacillary Dysentery (Shigellosis) - Four Phases:
| Phase | Features |
|---|---|
| Incubation | 1-4 days (range up to 8 days) |
| Watery diarrhoea | Transient fever, watery loose stools, malaise, anorexia, nausea/vomiting |
| Dysentery | Bloody mucopurulent stools, severe tenesmus, abdominal cramps, high fever (40-41°C in children), urgency; dehydration is NOT a major feature (unlike cholera) |
| Post-infectious | Resolution over 1 week without treatment; with antibiotics resolves in days |
- HUS (S. dysenteriae type 1): Microangiopathic haemolytic anaemia + thrombocytopenia + acute renal failure
- Toxic megacolon: Severe inflammation extending transmurally; colon dilatation
- Rectal prolapse - especially in malnourished children
- Hypoglycaemia, hyponatraemia (metabolic)
- Bacteraemia (rare; <5%; mainly malnourished/HIV patients)
- Ekiri syndrome (toxic encephalopathy in Japanese children)
- Reactive arthritis (post-dysentery HLA-B27 associated)
- Seizures, delirium, coma (children <5 years)
Amoebic Dysentery Features:
- Slower onset (3-4 weeks after infection) vs. bacterial (1-2 days)
- Lower fever or no fever (fever present in minority)
- Abdominal tenderness + increasingly severe diarrhoea
- Proctoscopy and sigmoidoscopy not painful (contrast to bacillary)
- More often chronic course with exacerbations after prolonged symptom-free periods
6. DIAGNOSTIC APPROACH
Step 1: History
- Travel history, food/water source, contact history
- Antibiotic use (C. difficile)
- Duration, character of stool (blood, mucus, volume)
- Onset speed - bacterial: 1-2 days; amoebic: weeks
Step 2: Physical Examination
- Temperature, dehydration signs
- Abdominal tenderness (LIF/suprapubic)
- Rectal examination / proctoscopy / sigmoidoscopy
Step 3: Stool Investigations
| Test | Method | Purpose |
|---|---|---|
| Stool microscopy (fresh) | Wet mount + iodine stain | Trophozoites (with ingested RBCs in amoebiasis) or cysts; PMNs in bacterial dysentery |
| Stool culture (Gold standard for bacterial) | Mac-Conkey, Hektoen, SS agar; incubation 12-18h at 37°C | Isolate Shigella, Salmonella, Campylobacter, Yersinia |
| Stool antigen test (ELISA) | E. histolytica-specific antigen (galactose/GalNAc lectin) | Distinguishes E. histolytica from E. dispar (which is non-pathogenic but morphologically identical) |
| PCR / NAAT | Shigella-specific virulence gene sequences | Increasing use; high sensitivity; not yet globally standardized |
| C. difficile toxin A/B | NAAT (most sensitive), EIA | Antibiotic-associated colitis |
| Stool for ova and parasites | Concentration, stain, microscopy | Schistosoma, Trichuris |
| Fecal leukocytes | Wright's/methylene blue stain | Presence confirms invasive/inflammatory cause |
- Shigellosis: Many PMNs per field; no trophozoites
- Amoebiasis: Erythrophagocytic trophozoites; very few PMNs
Step 4: Blood Investigations
| Test | Purpose |
|---|---|
| FBC | Leukocytosis (bacterial), anaemia (haemorrhage/HUS), thrombocytopenia (HUS) |
| Serum electrolytes | Hyponatraemia, hypokalaemia |
| Serum urea/creatinine | HUS, dehydration |
| Blood film / Coombs' test | Microangiopathic haemolytic anaemia in HUS |
| LFTs, imaging (USS/CT) | Amoebic liver abscess |
| Serology (amoeba) | Anti-amoebic antibodies (useful for extraintestinal amoebiasis) |
Step 5: Endoscopy / Imaging
| Procedure | Indication/Findings |
|---|---|
| Proctoscopy / Sigmoidoscopy | Bacillary: acute purulent proctitis, shallow ulcers, edematous hemorrhagic mucosa; Amoebic: NOT painful; flask-shaped ulcers with undermined edges |
| Colonoscopy + biopsy | Chronic cases; distinguish from IBD; histology for trophozoites |
| Abdominal X-ray | Toxic megacolon (colon >6 cm) |
| USS / CT abdomen | Amoebic liver abscess |
| Stool PCR / culture-based typing (PulseNet) | Outbreak investigation |
7. MANAGEMENT
General / Supportive
- Oral rehydration therapy (ORT) - WHO ORS (245 mOsm/L) is the mainstay; IV fluids only for severe dehydration/coma/shock
- Shigellosis rarely causes significant dehydration - but remains important in endemic settings
- Nutrition: Start as early as possible; malnutrition is the primary risk factor for death
- Isolation: Source isolation; strict hand hygiene; sodium hypochlorite decontamination
- Zinc supplementation (children): 10-20 mg/day × 10-14 days
- AVOID antimotility agents (loperamide, diphenoxylate) in dysentery - risk of toxic megacolon, prolonged fever, increased HUS risk in EHEC
Management of Complications
| Complication | Management |
|---|---|
| Toxic megacolon | Medical/surgical assessment; correct anaemia, K⁺ deficit; NG aspiration; colectomy if no improvement after 48-72 h |
| Rectal prolapse | Manual reduction (knee-chest position); osmotic reduction with warm saturated MgSO₄ gauze |
| HUS | Water restriction; discontinue ORS and K⁺-rich nutrition; hemofiltration / peritoneal dialysis |
| Intestinal perforation | Emergency surgery + intensive medical support |
| Amoebic liver abscess | Metronidazole ± drainage |
8. PHARMACOLOGY
A. Antibiotics for Bacillary Dysentery
IMPORTANT: As an invasive disease, shigellosis requires antibiotic treatment. However, multidrug resistance is now a dominant factor in treatment decisions.
First-Line: Fluoroquinolones
| Drug | Dose (Adult) | Dose (Children) | Duration |
|---|---|---|---|
| Ciprofloxacin | 500 mg BD | 30 mg/kg/day in 2 divided doses | 3 days |
| Norfloxacin | 400 mg BD | - | 3 days |
| Ofloxacin | 200 mg BD | - | 3 days |
Alternative/Second-Line
| Drug | Dose | Notes |
|---|---|---|
| Azithromycin | 500 mg OD × 3 days (adults); 10-20 mg/kg/day × 3 days (children) | Preferred in regions with fluoroquinolone resistance; drug of choice for children with dysentery |
| Ceftriaxone | 50-100 mg/kg/day IV × 2-5 days | Severe/hospitalized cases; children with MDRSA (multi-drug resistant Shigella) |
| Pivmecillinam | 400 mg TDS × 5 days | Active against most Shigella spp. |
| Trimethoprim-sulfamethoxazole | No longer recommended | Widespread resistance |
| Ampicillin/Amoxicillin | No longer recommended | High resistance rates globally |
Antibiotics by Organism (Goldman-Cecil Table 265-7)
| Organism | Treatment |
|---|---|
| Shigella | Ciprofloxacin 500 mg BD × 3 days (adults) |
| Campylobacter | Azithromycin 500 mg OD × 3 days |
| Salmonella (non-typhoidal) | Ciprofloxacin 20 mg/kg/day × 7 days; OR Azithromycin 20 mg/kg/day × 7 days |
| EHEC (O157:H7) | AVOID antibiotics - increase risk of HUS |
| C. difficile (mild) | Metronidazole 400-500 mg TDS × 10 days |
| C. difficile (severe) | Vancomycin 125 mg QDS × 10 days (oral) |
| C. difficile (recurrent/preferred) | Fidaxomicin 200 mg BD × 10 days (lower recurrence rate) |
B. Treatment of Amoebic Dysentery
Step 1: Tissue Amoebiasis (Active Dysentery/Invasive Disease)
| Drug | Mechanism | Dose | Notes |
|---|---|---|---|
| Metronidazole (1st line) | 5-nitroimidazole; reduced by microbial electron transport proteins in anaerobes → toxic free radicals → DNA strand breaks | 500-750 mg TDS × 7-10 days | Drug of choice; covers trophozoites in tissue and intestinal wall |
| Tinidazole (preferred alternative) | Same class and mechanism as metronidazole; longer half-life, better tolerated | 2 g OD × 3-5 days | Fewer GI side effects; single daily dosing; preferred over metronidazole |
- Rapidly absorbed orally; t½ 8 hours; >50% hepatic metabolism; excreted in urine
- Adverse effects: Nausea, vomiting, diarrhoea, metallic taste (very common), headache, dizziness, vertigo, numbness
- Disulfiram-like reaction with alcohol (avoid alcohol during and 48h after course)
- Can cause peripheral neuropathy in high doses / prolonged use
- Longer half-life → shorter dosing regimen
- Less GI side effects
- Same alcohol warning (disulfiram-like reaction)
Step 2: Luminal Amoebiasis (Eradication of Cysts - MANDATORY after tissue therapy)
Neither metronidazole nor tinidazole reliably eradicates intraluminal cysts - therefore a luminal amoebiocide MUST always follow tissue therapy to prevent relapse.
| Drug | Mechanism | Dose |
|---|---|---|
| Paromomycin (preferred) | Poorly absorbed aminoglycoside; acts within gut lumen; inhibits ribosomal protein synthesis | 500 mg TDS × 7-10 days |
| Diloxanide furoate | Direct luminal amoebiocide; mechanism not fully established | 500 mg TDS × 10 days; also effective as sole treatment for asymptomatic cyst carriers |
| Iodoquinol | Luminal amoebiocide; mechanism unclear | 650 mg TDS × 20 days |
- Metronidazole or Tinidazole (tissue) THEN
- Paromomycin or Diloxanide furoate (luminal cyst eradication)
C. Treatment of Schistosomal Dysentery
| Drug | Dose | Notes |
|---|---|---|
| Praziquantel | 40 mg/kg in 2 divided doses × 1 day (S. mansoni/haematobium); 60 mg/kg in 3 doses × 1 day (S. japonicum) | Drug of choice; specialist in tropical medicine should supervise |
D. Treatment of C. difficile Colitis (Antibiotic-Associated Dysentery)
| Severity | Drug | Dose |
|---|---|---|
| Mild-moderate | Metronidazole | 400-500 mg TDS × 10 days |
| Severe | Vancomycin (oral) | 125 mg QDS × 10 days |
| Recurrent/Preferred | Fidaxomicin | 200 mg BD × 10 days |
| Refractory | Faecal microbiota transplant (FMT) | Restores healthy microbiota |
E. Drugs to AVOID in Dysentery
| Drug | Reason to Avoid |
|---|---|
| Antimotility agents (loperamide, diphenoxylate) | Prolong fever in shigellosis; increase risk of toxic megacolon; suspected to increase HUS risk in EHEC |
| Antibiotics in EHEC O157:H7 | Increase risk of HUS (Shiga toxin release during bacterial lysis) |
| Trimethoprim-sulfamethoxazole | Widespread Shigella resistance worldwide |
| Nalidixic acid | Widespread quinolone resistance in Shigella |
Summary: Bacillary vs. Amoebic Dysentery
| Feature | Bacillary (Shigella) | Amoebic (E. histolytica) |
|---|---|---|
| Onset | Acute (1-4 days) | Gradual (3-4 weeks) |
| Fever | High (40-41°C) | Often absent/low |
| Course | Usually self-limited (1 week) | Chronic with relapses |
| Stool microscopy | Many PMNs; no trophozoites | Erythrophagocytic trophozoites; few PMNs |
| Sigmoidoscopy | Painful; hemorrhagic mucosa; small shallow ulcers | Not painful; flask-shaped undermined ulcers |
| Dehydration | Rare | Rare |
| Liver abscess | No | Yes (extraintestinal spread) |
| Treatment | Ciprofloxacin / Azithromycin | Metronidazole THEN Paromomycin |
- Harrison's Principles of Internal Medicine 22E - Shigellosis chapter (Chapters 172, 230)
- Goldman-Cecil Medicine - Amebic Dysentery, Table 265-7
- Bailey and Love's Short Practice of Surgery 28th Ed - Bacillary and Amoebic dysentery pathology
- Sherris & Ryan's Medical Microbiology 8th Ed - Shigella pathogenesis
- Robbins & Kumar Basic Pathology - Infectious Enterocolitis
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Metronidazole, antiprotozoal drugs
provide defenition, types, causes, pathology, diagnostic approach , management along with pharmacology for IBS
Irritable Bowel Syndrome (IBS): Complete Clinical Guide
1. DEFINITION
- Functional constipation (chronic idiopathic constipation)
- Functional diarrhoea
- Functional abdominal bloating/distension
- Functional dyspepsia
2. EPIDEMIOLOGY
- Global prevalence: 4.1% (Rome IV criteria); up to 9% using older Rome III criteria
- More common in women (5.2%) than men (2.9%) - odds ratio ~1.7
- More prevalent in patients under 50 years and those with lower socioeconomic status
- Up to 50% of individuals with IBS symptoms do not seek healthcare
- Generates ~4.4 million annual physician visits in the US alone
- Associated with significant work absenteeism and impaired productivity
- IBS-D and IBS-M each account for 35-40% of cases; IBS-C ~25%; IBS-U <5%
3. TYPES / SUBTYPES
| Subtype | Bristol Stool Form | Prevalence |
|---|---|---|
| IBS-C (Constipation-predominant) | >25% of stools are types 1-2 (hard/lumpy) AND <25% are types 6-7 | ~25% |
| IBS-D (Diarrhoea-predominant) | >25% are types 6-7 (loose/watery) AND <25% are types 1-2 | 35-40% |
| IBS-M (Mixed bowel habits) | >25% are types 1-2 AND >25% are types 6-7 | 35-40% |
| IBS-U (Unclassified) | Does not meet criteria for C, D, or M | <5% |
- Women with IBS are more likely to have IBS-C (OR 2.38)
- Men with IBS are more likely to have IBS-D (OR 0.45 in women, i.e., men predominate)
- Women's symptoms can worsen premenstrually when oestrogen and progesterone decline
4. CAUSES AND RISK FACTORS
A. Predisposing Factors
| Factor | Details |
|---|---|
| Genetic predisposition | IBS clusters in families; relatives 1.75-2.75× more likely to be affected. Polymorphisms in serotonin transporter gene (5-HTTLPR), CRF receptor 1 (CRF-1R), cannabinoid receptors, COMT, interleukins, and TNF-α |
| Female sex | Twofold increased prevalence; hormonal modulation |
| Age <50 years | Peak incidence in young to middle-aged adults |
| Lower socioeconomic status | Also associated with higher anxiety/depression |
B. Precipitating Factors
| Factor | Details |
|---|---|
| Post-infectious IBS (PI-IBS) | Develops after bacterial, viral, or parasitic gastroenteritis; 10-25% of patients develop IBS after acute GI infection. Risk factors: female sex, prolonged illness, psychological distress at time of infection |
| Adverse childhood experiences | Physical/sexual abuse, neglect - major risk factor; trauma alters gut-brain axis |
| Psychological stress | HPA axis dysregulation; stress exacerbates gut permeability, motility, immune activation |
| Food triggers | Fatty/high-carbohydrate meals, coffee, alcohol, spicy foods, lactose, gluten, FODMAPs |
| Antibiotics | Alter gut microbiota composition; risk factor for IBS development |
| Dietary pattern | High-fat, low-fibre diet |
5. PATHOBIOLOGY (Pathophysiology)
A. Visceral Hypersensitivity (Central Mechanism)
- Patients have lowered pain thresholds to luminal distension (balloon distension studies show pain at lower volumes than healthy controls)
- Allodynia: Perception of pain with normally non-painful stimuli
- Central sensitization: Altered brain processing of visceral afferent signals
- Brain imaging shows activation of emotional arousal centres (amygdala, anterior cingulate cortex) during rectal distension rather than the pain inhibitory areas (prefrontal cortex) seen in controls
- Endogenous pain modulation is impaired: Reduced activation of descending inhibitory pathways; reduced activation of PFC during rectal distension
- Structural brain changes: Greater volume/cortical thickness of sensorimotor cortex correlating with symptom severity
B. Altered GI Motility
- Colonic transit is slower in IBS-C and faster in IBS-D
- Exaggerated colonic responses to meals (gastrocolic reflex), cholecystokinin (CCK), and mechanical stimuli
- Increased high-amplitude propagating contractions (HAPCs) in some patients
C. Mucosal Immune Activation
- Increased mast cells adjacent to sensory neurons in colonic mucosa
- Mast cells release histamine → activate afferent nerves → peripheral sensitization → increased abdominal pain
- Increased T lymphocytes in colonic mucosa
- Elevated mucosal colonic nerves expressing substance P, TRPV1 cannabinoid receptors, and protease-activated receptors
D. Increased Intestinal Permeability (Leaky Gut)
- Some patients have decreased tight junction protein expression in jejunum and colon
- Increased permeability linked to greater visceral hyperalgesia, abdominal pain severity, and altered bowel habits
- Likely mediated by immune activation (mast cells + T cells) and food allergens
- Also linked to non-classical food allergies and postprandial symptoms
E. Dysbiosis (Gut Microbiota Imbalance)
- IBS fecal microbiota shows:
- Increased: Enterobacteriaceae, Lactobacillaceae, Bacteroides (produce organic acids, reduce mucosal glycoproteins)
- Decreased: Clostridiales, Faecalibacterium prausnitzii, Bifidobacterium (produce butyrate - anti-inflammatory, epithelial energy source)
- ~25% of IBS patients have bile acid diarrhoea (BAD) due to impaired ileal bile acid reabsorption
F. Serotonin (5-HT) Dysregulation
- ~95% of body's serotonin is in enterochromaffin cells of the gut
- Serotonin regulates motility, secretion, and visceral sensation
- Altered serotonin transporter (SERT) expression in IBS:
- Low SERT expression → excess 5-HT → IBS-D (increased secretion and motility)
- High SERT expression → rapid 5-HT reuptake → IBS-C
- This forms the basis for 5-HT-targeted pharmacotherapy
G. Dysregulated Stress Response
- Hyperactivated hypothalamic-pituitary-adrenal (HPA) axis in IBS compared to controls
- Stress increases visceral sensitivity, gut motility, gut permeability, and mucosal immune responses
- Explains worsening of IBS during periods of psychological stress
H. Genetic/Epigenetic Factors
- Polymorphisms in 5-HTTLPR, CRF-1R, cannabinoid receptors, COMT
- Alterations in gene methylation and non-coding microRNA expression
6. CLINICAL FEATURES
Core Symptoms (Required for Diagnosis)
- Recurrent abdominal pain: Crampy, lower abdominal, often related to defecation
- Altered bowel habits: Diarrhoea, constipation, or alternating
- Associated with defecation: Pain relieved or worsened by passing stool
- Bloating/abdominal distension: Very common; often worsens through the day
Supportive Symptoms
| Symptom | Detail |
|---|---|
| Abnormal stool frequency | ≤3/week or >3/day |
| Abnormal stool form | Hard/lumpy or loose/watery |
| Straining or urgency | |
| Feeling of incomplete evacuation | |
| Passing mucus per rectum | |
| Postprandial symptoms | ~63-67% have meal-related symptoms; worse with fatty/carbohydrate-rich food, coffee, alcohol, spicy food |
Extraintestinal Manifestations (Frequent Comorbidities)
- Functional: Functional dyspepsia, functional heartburn (coexist in ~1/3)
- Pain syndromes: Fibromyalgia, chronic pelvic pain, chronic fatigue syndrome
- Urological: Interstitial cystitis, painful bladder syndrome
- Neurological: Migraine headaches, temporomandibular joint disorder
- Gynaecological: Dysmenorrhoea
- Psychological: Anxiety, depression, somatization (major comorbidities)
- Sleep disturbances: Especially when GI symptoms are severe
7. DIAGNOSTIC APPROACH
Rome IV Diagnostic Criteria (2016) - Gold Standard
- Related to defecation
- Associated with a change in frequency of stool
- Associated with a change in form (appearance) of stool
IBS Diagnostic Algorithm (Goldman-Cecil, Fig. 123-1):
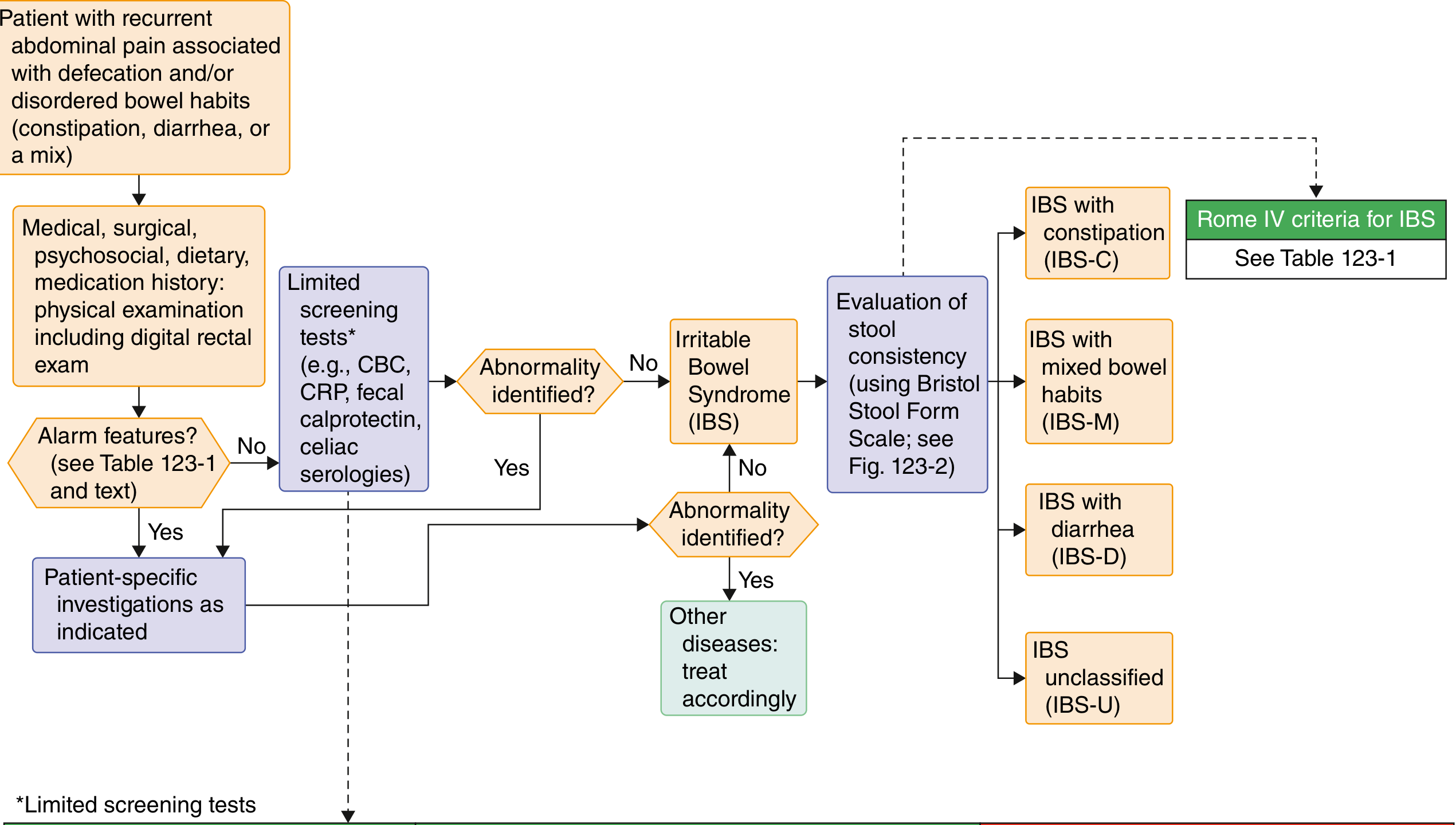
Alarm Features (Red Flags) - REQUIRE FURTHER INVESTIGATION
| Alarm Feature | Concern |
|---|---|
| New onset symptoms age ≥50 years | Colorectal cancer |
| Unintentional weight loss | Malignancy, IBD, coeliac |
| Haematochezia or melaena (not haemorrhoids) | Malignancy, IBD |
| Nocturnal diarrhoea | Organic disease |
| Anaemia | Malignancy, IBD, coeliac |
| Palpable abdominal mass or lymphadenopathy | Malignancy |
| Family history of colorectal cancer, IBD, or coeliac disease | Inherited risk |
Investigations
| Test | Population | Purpose |
|---|---|---|
| FBC (CBC) | All IBS | Rule out anaemia (IBD, coeliac, malignancy) |
| CRP / ESR | IBS-D | Exclude IBD (low CRP makes IBD less likely) |
| Fecal calprotectin / lactoferrin | IBS-D | Sensitive marker of intestinal inflammation; >100 µg/g suggests IBD |
| Coeliac serologies (anti-tTG IgA ± IgA level) | IBS-D | Exclude coeliac disease (prevalence ~4× higher in IBS-D) |
| Bile acid diarrhoea testing (SeHCAT, fasting 7αC4, fecal bile acids) | IBS-D with suspected BAD | ~25% of IBS-D patients have BAD |
| Giardia stool antigen | IBS-D in endemic areas | Exclude infectious cause |
| Anorectal physiology testing | IBS-C refractory | Exclude defaecatory disorder (dyssynergic defaecation) |
| TSH | All IBS (if clinically indicated) | Thyroid dysfunction mimics IBS |
| Not Recommended | Reason |
|---|---|
| Routine stool cultures/ova & parasites | Unless history suggests infection |
| Routine colonoscopy in patients <45 years without alarm features | Low yield; IBS is a positive diagnosis |
| Food allergy or intolerance testing (IgE panels) | No established diagnostic value |
| Lactulose or glucose hydrogen breath testing (SIBO) | Limited utility; results confounded by altered transit |
| Anti-CdtB / antivinculin serologies | Low sensitivity; major societies do not recommend routinely |
| Test | Use |
|---|---|
| Colonoscopy + biopsy | Age ≥45-50, alarm features, rule out microscopic colitis (normal mucosa, abnormal biopsy - lymphocytic/collagenous colitis) |
| Lactose hydrogen breath test | If lactose intolerance suspected |
| Upper GI endoscopy + duodenal biopsy | If coeliac serology positive or clinical suspicion high |
| Pelvic floor / anorectal manometry + balloon expulsion test | IBS-C not responding to treatment; suspect defaecatory disorder |
| Colonic transit study (radio-opaque markers or scintigraphy) | Refractory IBS-C; quantify transit delay |
| Psychological assessment | Depression, anxiety, somatization, eating disorders |
8. MANAGEMENT
Step 1: Patient Education and Reassurance
- Explain the functional nature of IBS; reassure no malignancy
- Set realistic expectations - IBS is chronic but not progressive or life-threatening
- Address psychological concerns; validate symptoms
Step 2: Dietary Modification (First-Line)
| Intervention | Evidence | Notes |
|---|---|---|
| Low-FODMAP diet | Strong - improves global IBS symptoms | FODMAPs = Fermentable Oligosaccharides, Disaccharides, Monosaccharides And Polyols; especially helpful in IBS-D and bloating; requires dietitian supervision; followed by gradual food reintroduction |
| Soluble fibre (psyllium) | Moderate - especially IBS-C | Up to 25-35 g/day; start low and titrate; insoluble fibre (wheat bran) NOT recommended - can worsen bloating |
| Avoid triggers | Expert consensus | Food/symptom diary for 1-2 weeks; avoid fatty meals, caffeine, alcohol, spicy foods |
| Gluten-free diet | Limited evidence | Trial if gluten consistently triggers symptoms (after coeliac excluded) |
| Lactose restriction | Moderate | If lactose intolerance confirmed |
Step 3: Psychological Therapies (Highly Effective)
| Therapy | Evidence | Notes |
|---|---|---|
| Cognitive Behavioural Therapy (CBT) | Strongest evidence | Addresses catastrophizing, maladaptive illness behaviours; NNT ~4-5; reduces symptom severity and improves quality of life |
| Gut-directed hypnotherapy | Strong - 7 RCTs | Hypnosis directed at intestinal relaxation and motility control; NNT 5; effects persist at 12 months; 73% of responders continue using techniques |
| Psychodynamic psychotherapy | Moderate evidence | Addresses underlying psychological conflicts |
| Mindfulness therapy | Emerging evidence | Improves bowel symptoms and HRQOL in women with IBS |
| Relaxation training | Moderate evidence | Reduces autonomic hyperarousal |
9. PHARMACOLOGY
A. Drugs for PAIN AND SPASM
1. Antispasmodics (First-Line for Abdominal Pain)
| Drug | Mechanism | Dose | NNT | Notes |
|---|---|---|---|---|
| Hyoscine butylbromide (Buscopan) | Anticholinergic (muscarinic M1/M3 antagonist); reduces smooth muscle spasm | 10 mg TDS | 3 (2-25) | Poorly absorbed systemically; fewer anticholinergic side effects than atropine |
| Dicyclomine HCl (Merbentyl) | Anticholinergic + direct smooth muscle relaxant | 20-40 mg QDS | 4 (2-25) | |
| Otilonium bromide | Calcium channel blocker on smooth muscle; also anticholinergic | 40 mg TDS (before meals) | 5 (4-11) | |
| Pinaverium bromide | Calcium channel antagonist - selective for GI smooth muscle | 50-100 mg TDS | 4 (3-6) | |
| Drotaverine | PDE-4 inhibitor → increased cAMP → smooth muscle relaxation | 80 mg TDS | 2 (2-3) | |
| Alverine citrate + simethicone | Antispasmodic + anti-flatulent | 60 mg + 300 mg TDS | 8 (4-33) |
2. Peppermint Oil
- Mechanism: L-menthol - acts as calcium channel antagonist on gut smooth muscle → relaxation; also TRPV1 agonist → reduces visceral hypersensitivity; mild local anaesthetic effect
- Dose: ≥200 mg TDS (enteric-coated capsules to prevent lower oesophageal sphincter relaxation and heartburn)
- NNT: 4 (3-6) for abdominal pain and global IBS symptoms
- Recommended by: ACG, CAG, AGA, NICE
- Adverse effects: Heartburn/reflux (if non-enteric-coated), perianal burning
B. Drugs for IBS-D (Diarrhoea-Predominant)
1. Loperamide
- Mechanism: Peripheral mu-opioid receptor (MOR) agonist → reduces intestinal motility + increases anal sphincter tone + antisecretory activity
- Dose: 2-4 mg as needed; max 16 mg/day
- Evidence: Reduces stool frequency and improves consistency; does NOT significantly reduce abdominal pain - used as an adjunct to other IBS-D therapies
- Caution: Do not use in IBS as monotherapy for pain
2. Alosetron (Lotronex) - 5-HT3 Antagonist
- Mechanism: Potent antagonist of 5-HT3 receptors on enteric neurons; reduces colonic contractility, decreases colonic transit, increases fluid and electrolyte absorption, reduces visceral hypersensitivity
- Dose: 0.5-1 mg BD; start at 0.5 mg BD × 4 weeks; max 1 mg BD
- Indication: FDA-approved for severe IBS-D in women who have failed conventional therapy
- Adverse effects: Ischaemic colitis (3/1000 patients - serious adverse effect), severe constipation, nausea, GI discomfort
- Restricted access: Requires physician certification and detailed patient consent/education protocol due to risk of ischaemic colitis (discontinued treatment required immediately if symptoms develop)
3. Eluxadoline (Viberzi) - Mixed Opioid Receptor Agent
- Mechanism: MOR agonist + DOR antagonist + KOR agonist - acts locally in enteric nervous system; reduces abdominal pain and diarrhoea without causing rebound constipation
- Dose: 100 mg BD with food (gallbladder intact); 75 mg BD (no gallbladder)
- Adverse effects: Pancreatitis (especially in patients without a gallbladder - sphincter of Oddi spasm), constipation, nausea, abdominal pain
- Contraindicated in: Biliary duct obstruction, sphincter of Oddi disease/dysfunction, pancreatitis history, absent gallbladder (relative), severe constipation, alcohol dependence
4. Rifaximin - Non-absorbable Antibiotic
- Mechanism: Non-absorbed rifamycin-class antibiotic; inhibits bacterial RNA polymerase β subunit → bactericidal effect within GI lumen without systemic absorption; reduces dysbiosis and SIBO
- Dose for IBS-D: 550 mg TDS × 14 days (may repeat up to 2 courses)
- Evidence: Reduces bloating, abdominal discomfort, and diarrhoea in non-constipating IBS; ~40% response rate
- Advantage: Minimal systemic side effects; low risk of Clostridium difficile
- ACG recommendation: Strong recommendation for non-constipating IBS
5. Bile Acid Sequestrants (for IBS-D with BAD)
| Drug | Class | Dose |
|---|---|---|
| Cholestyramine | Bile acid sequestrant | 2-4 g/day, titrate to max 24 g/day |
| Colestipol | Bile acid sequestrant | 1 g BD |
| Colesevelam | Bile acid sequestrant | 2 tablets (625 mg) TDS |
C. Drugs for IBS-C (Constipation-Predominant)
1. Osmotic Laxatives
- Polyethylene glycol (Macrogol/Movicol): Improves stool frequency and consistency but does NOT reduce abdominal pain; safe, OTC, inexpensive; side effects: bloating, abdominal pain, nausea
2. Lubiprostone (Amitiza)
- Mechanism: Chloride channel (ClC-2) activator on intestinal epithelium → increased luminal chloride secretion → fluid secretion into intestinal lumen → softens stool and increases motility
- Dose: 8 µg BD for IBS-C (lower dose than for chronic idiopathic constipation)
- Evidence: Improves constipation, stool consistency, straining, abdominal pain, bloating
- Adverse effects: Nausea (most common; reduced by taking with food), diarrhoea, dyspepsia
- Contraindicated in pregnancy (possible foetal harm - category C)
3. Linaclotide (Linzess)
- Mechanism: Guanylate cyclase-C (GC-C) receptor agonist on intestinal epithelium → increases intracellular cGMP → activates CFTR chloride channel → secretion of chloride and bicarbonate into intestinal lumen → increased fluid and motility. Also decreases firing of visceral sensory C-fibres via cGMP → reduces abdominal pain (dual action)
- Dose: 290 µg OD (30 min before first meal of day) for IBS-C
- Adverse effects: Diarrhoea (most common; dose-dependent), abdominal pain
- FDA approved for IBS-C and chronic idiopathic constipation
4. Plecanatide (Trulance)
- Mechanism: Structurally similar to uroguanylin; GC-C receptor agonist (same mechanism as linaclotide but pH-sensitive - greater activity in the alkaline small intestine)
- Dose: 3 mg OD
- Evidence: Similar benefits to linaclotide in IBS-C
- Adverse effects: Diarrhoea
5. Tenapanor (Ibsrela)
- Mechanism: Minimally absorbed inhibitor of Na⁺/H⁺ exchanger isoform 3 (NHE3) in the gut → blocks sodium (and therefore water) reabsorption → increased luminal fluid → softer stools and increased motility
- Dose: 50 mg BD for IBS-C
- Adverse effects: Diarrhoea
6. Prucalopride (Resolor)
- Mechanism: Selective, high-affinity 5-HT4 receptor agonist on enteric neurons → triggers prokinetic activity throughout the colon; stimulates peristaltic reflex
- Dose: 1-2 mg OD
- Primarily approved for chronic constipation; used off-label in IBS-C
- Adverse effects: Headache, nausea, diarrhoea, abdominal pain
D. Brain-Gut Neuromodulators (for PAIN in ALL IBS subtypes)
1. Tricyclic Antidepressants (TCAs)
- Drugs: Amitriptyline, imipramine, doxepin, desipramine, nortriptyline
- Mechanism: Block serotonin and noradrenaline reuptake → enhance descending pain inhibition; also anticholinergic effects → slow gut transit (beneficial in IBS-D)
- Dose for IBS: Low doses, 10-25 mg at bedtime (sub-antidepressant doses for pain modulation); can titrate up to 75-100 mg
- Evidence: NNT = 4.5 (3.5-7) for global IBS symptoms; especially effective for abdominal pain
- Preferred agents: Desipramine or nortriptyline (less sedation, less constipation, less dry mouth than amitriptyline)
- Especially useful: IBS-D (anticholinergic slows transit); also for sleep disturbance
- Adverse effects: Dry mouth, sedation, constipation (problematic in IBS-C), blurred vision, urinary retention, weight gain, cardiac arrhythmia (at higher doses)
- Recommended by: ACG (1A), CAG (1A) - highest quality evidence
2. Selective Serotonin Reuptake Inhibitors (SSRIs)
- Drugs: Fluoxetine, sertraline, paroxetine, citalopram
- Mechanism: Block serotonin reuptake transporter (SERT) → increased synaptic serotonin → modulates gut motility (accelerates transit) and CNS pain processing; enhances descending inhibitory pathways
- Dose: 10-100 mg daily (standard antidepressant doses)
- Evidence: NNT = 5 (3-16.5) for global IBS symptoms; less effective than TCAs for abdominal pain reduction; may be useful in IBS-C (prokinetic effect); fewer side effects than TCAs
- Adverse effects: Nausea, insomnia, sexual dysfunction, GI side effects, serotonin syndrome (rare)
- Recommended by: ACG (2C), CAG (2C)
3. Serotonin-Noradrenaline Reuptake Inhibitors (SNRIs)
- Drugs: Duloxetine, venlafaxine
- Mechanism: Dual reuptake inhibition of serotonin and noradrenaline → enhanced descending pain inhibition; especially effective for comorbid pain conditions (fibromyalgia, chronic pelvic pain)
- Use: Patients with IBS + chronic pain who cannot tolerate TCAs
- Adverse effects: Nausea, sweating, hypertension, serotonin syndrome risk
E. Probiotics
- Mechanism: Restore commensal gut microbiota; improve dysbiosis; produce short-chain fatty acids (butyrate); modulate mucosal immune response; reduce visceral hypersensitivity
- Evidence: NNT = 7 (5-12) for global IBS symptoms (37 RCTs, n=4403); most useful for bloating
- Best-studied strains: Bifidobacterium infantis 35624, Lactobacillus plantarum, Lactobacillus GG, Saccharomyces boulardii
- Recommended by: ACG (2C), CAG (2C)
- Combination products may be more effective than single strains (NNT 19 for combinations, though CI wide)
F. Summary Pharmacology by Subtype
| Symptom/Subtype | First-Line Drugs | Second-Line |
|---|---|---|
| Abdominal pain (all) | Antispasmodics, peppermint oil | TCAs, SSRIs, SNRIs |
| IBS-D | Loperamide (stool) + TCA (pain) | Alosetron (women, severe), Eluxadoline, Rifaximin |
| IBS-C | Psyllium fibre, PEG, Linaclotide | Lubiprostone, Plecanatide, Tenapanor |
| Bloating | Low-FODMAP diet, Probiotics | Rifaximin |
| Psychological comorbidity | CBT, SSRIs | SNRIs, hypnotherapy |
| Bile acid diarrhoea | Cholestyramine, Colesevelam | Obeticholic acid (experimental) |
Summary: IBS at a Glance
| Feature | Detail |
|---|---|
| Nature | Functional GI disorder - no structural abnormality |
| Core symptom | Recurrent abdominal pain + altered bowel habits |
| Diagnosis | Positive diagnosis using Rome IV criteria; limited selected tests; NOT diagnosis of exclusion |
| Pathophysiology | Gut-brain dysregulation, visceral hypersensitivity, altered motility, dysbiosis, mucosal immune activation |
| Subtypes | IBS-C, IBS-D, IBS-M, IBS-U (based on Bristol Stool Form Scale) |
| Treatment | Stepwise: Education → Diet (FODMAP) → Psychological therapy → Pharmacotherapy based on dominant symptom |
| Key drugs for pain | Antispasmodics (hyoscine), peppermint oil, TCAs (low dose) |
| Key drugs for IBS-D | Loperamide, alosetron, eluxadoline, rifaximin, bile acid sequestrants |
| Key drugs for IBS-C | Linaclotide, lubiprostone, plecanatide, tenapanor |
| Prognosis | Chronic but not progressive; does not increase colorectal cancer risk |
- Goldman-Cecil Medicine - Chapters 123 (IBS), including Rome IV criteria table and diagnostic algorithm
- Yamada's Textbook of Gastroenterology 7th Ed - Chapter 67 (comprehensive IBS pathobiology, treatment tables, NNT data)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease - Functional bowel disorders
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Alosetron, eluxadoline, linaclotide, rifaximin, lubiprostone pharmacology
provide defenition, types, causes, pathology, diagnostic approach , management along with pharmacology for INTESTINAL WORM INFESTATION
Intestinal Worm Infestation (Intestinal Helminthiasis): Complete Clinical Guide
1. DEFINITION
- Unlike protozoa, helminths are macroscopic multicellular organisms
- They cannot multiply within the human host (except Strongyloides and Capillaria) - disease severity is related to worm burden (intensity of infection)
- They produce eggs/larvae passed in faeces to continue the life cycle in soil or water
- Most infections are asymptomatic in low worm burdens; symptoms increase proportionately with worm load
2. CLASSIFICATION / TYPES
A. By Organism Type
| Class | Common Name | Examples |
|---|---|---|
| Nematodes (Roundworms) | Roundworms | Ascaris, hookworm, Enterobius, Trichuris, Strongyloides, Trichinella |
| Cestodes (Tapeworms) | Tapeworms | Taenia solium, T. saginata, Diphyllobothrium, Echinococcus |
| Trematodes (Flukes) | Flukes | Schistosoma, Fasciolopsis, Clonorchis, Opisthorchis |
B. Common Intestinal Nematodes (Focus of This Guide)
| Organism | Common Name | Site in Gut |
|---|---|---|
| Ascaris lumbricoides | Giant roundworm | Small intestine |
| Trichuris trichiura | Whipworm | Caecum, large intestine |
| Enterobius vermicularis | Pinworm / Threadworm | Large intestine, perianal area |
| Necator americanus | New world hookworm | Small intestine |
| Ancylostoma duodenale | Old world hookworm | Small intestine (duodenum/jejunum) |
| Strongyloides stercoralis | Threadworm | Duodenojejunal mucosa |
| Trichinella spiralis | Trichina worm | Small intestine (larvae → muscle) |
| Capillaria philippinensis | Capillaria | Small intestine |
C. Common Intestinal Cestodes (Tapeworms)
| Organism | Common Name | Transmission |
|---|---|---|
| Taenia solium | Pork tapeworm | Undercooked pork |
| Taenia saginata | Beef tapeworm | Undercooked beef |
| Diphyllobothrium latum | Fish tapeworm | Raw fish |
| Hymenolepis nana | Dwarf tapeworm | Fecal-oral |
3. CAUSES AND TRANSMISSION
Fecal-Oral Route (Most Common)
| Worm | Transmission Route | Key Risk |
|---|---|---|
| Ascaris | Ingestion of embryonated eggs from soil-contaminated food/water | Playing in contaminated soil; unwashed vegetables |
| Trichuris | Ingestion of embryonated eggs from contaminated soil | Same as Ascaris |
| Enterobius | Ingestion of eggs; perianal-to-hand-to-mouth; fomites; bedding | Children in daycare/schools; entire household transmission |
| Hymenolepis nana | Fecal-oral; no intermediate host needed | Autoinfection possible |
Skin Penetration Route
| Worm | Transmission | Key Risk |
|---|---|---|
| Necator americanus | Filariform larvae penetrate bare skin (feet) from contaminated soil | Walking barefoot in tropical areas |
| Ancylostoma duodenale | Skin penetration OR oral ingestion of larvae | Barefoot exposure + undercooked vegetables |
| Strongyloides stercoralis | Filariform larvae penetrate skin; also perianal autoinfection | Unique: autoinfection means lifelong persistence without reexposure |
Meat Consumption
| Worm | Source | Key Risk |
|---|---|---|
| Taenia solium | Undercooked pork | Cysticercosis if eggs ingested (vs. just pork) |
| Taenia saginata | Undercooked beef | |
| Trichinella spiralis | Undercooked pork, bear, walrus, horse meat | |
| Diphyllobothrium latum | Raw or undercooked freshwater fish |
Special Routes
- Anisakiasis: Ingestion of raw saltwater fish (sushi/sashimi)
- Capillaria: Raw freshwater fish
4. PATHOLOGY (Organ-by-Organ)
A. ASCARIS LUMBRICOIDES
- Ingestion of embryonated eggs from contaminated soil/food
- Larvae hatch in small intestine → penetrate intestinal mucosa → portal venules → liver → right heart → pulmonary capillaries
- Too large for pulmonary capillaries → rupture into alveolar spaces → coughed up → swallowed → reach small intestine
- Mature into adults in small intestine (2-3 months from ingestion to oviposition)
- Adults live 1-2 years, survive by muscular swimming against intestinal flow (do NOT burrow into mucosa)
- Intestinal phase: Abdominal pain, nausea, vomiting; obstruction with heavy loads (bolus of worms in small intestine); malnutrition and growth stunting in children
- Larval migration phase (Loeffler's syndrome): Cough, wheezing, eosinophilia, transient pulmonary infiltrates on CXR
- Complications: Intestinal obstruction, biliary obstruction (worms migrating into bile duct/pancreatic duct), cholangitis, pancreatitis, perforation, volvulus, appendicitis
- Eosinophilia is prominent during larval migration phase
B. TRICHURIS TRICHIURA (Whipworm)
- Unembryonated eggs passed in stool → embryonate in soil (15-30 days)
- Infective eggs ingested → hatch in small intestine → larvae mature and establish as adults in caecum and ascending colon
- Anterior thin ends thread through and anchor in colonic mucosa; posterior ends remain free in lumen
- Adults live ~1 year; females produce eggs 60-70 days after infection
- Light infections: Asymptomatic
- Moderate infections: Nausea, abdominal pain, diarrhoea, growth stunting
- Heavy infections (>800 worms): Entire colonic lumen parasitized → significant mucosal damage, blood loss, anaemia; "dysentery syndrome" with bloody diarrhoea mimicking Shigella; tenesmus; rectal prolapse (hallmark of heavy Trichuris load)
- Moderate eosinophilia in heavy infections (adults anchored in mucosa present antigens to GALT)
C. ENTEROBIUS VERMICULARIS (Pinworm/Threadworm)
- Eggs ingested (hand-to-mouth, fomites, bedding, inhalation) → hatch in small intestine → mature in large intestine
- Female migrates nocturnally to perianal area to deposit 10,000-11,000 eggs in perianal skin folds
- Eggs are immediately infective (no soil maturation required)
- Reinfection: scratching → eggs under fingernails → fecal-oral transmission
- Perianal pruritus (especially nocturnal) - cardinal symptom
- Vulvovaginitis in girls (ectopic migration)
- Insomnia, irritability, restlessness
- Appendicitis (rare; ectopic worms in appendix)
- Light infections usually asymptomatic
- No eosinophilia (adults confined to intestinal lumen; no tissue invasion)
D. HOOKWORM (Necator americanus and Ancylostoma duodenale)
- Eggs passed in faeces → hatch in soil within 48 hours → rhabditiform larvae (free-living) → develop into infective filariform larvae within 1 week
- Filariform larvae penetrate bare skin (usually feet)
- Lymphohematogenous transport → right heart → lungs → rupture into alveoli → coughed up → swallowed → small intestine
- Attach to small bowel mucosa using teeth/cutting plates; suck blood and villous tissue
- Prepatent period: 6-8 weeks
- Ancylostoma duodenale: 0.2 mL/worm/day (more serious)
- Necator americanus: 0.03 mL/worm/day
- Additional blood loss from migration and old attachment sites
- Skin (ground itch): Pruritic maculopapular rash at larval entry site; serpiginous tracks
- Pulmonary (Loeffler's): Transient cough, eosinophilia, mild pneumonitis (less severe than Ascaris)
- Intestinal phase: Epigastric pain, nausea, bloating 1-2 months after heavy infection
- Chronic heavy infection: Iron-deficiency anaemia (hypochromic microcytic) - the major clinical consequence; hypoproteinaemia/hypoalbuminaemia with oedema (face, extremities, abdomen); fatigue, weakness, dyspnoea
- "Wakana disease" (Ancylostoma): Nausea, vomiting, dyspnoea after oral larval ingestion
- Eosinophilia peaks at 5-9 weeks (when adults appear in intestine)
E. STRONGYLOIDES STERCORALIS
- Filariform larvae penetrate skin → lungs → swallowed → embed in duodenojejunal mucosa
- Parthenogenetic female worms (1-2 mm; no males in humans) produce eggs in mucosa → rhabditiform larvae pass in faeces OR
- Autoinfection: Rhabditiform larvae → filariform larvae in bowel → penetrate colonic wall or perianal skin → re-enter circulation and repeat the cycle
- Uncomplicated strongyloidiasis: Often asymptomatic; cutaneous larva currens (serpiginous, erythematous, pruritic, moves up to 10 cm/h); midepigastric pain resembling peptic ulcer disease; nausea, diarrhoea, alternating constipation
- Hyperinfection syndrome (immunocompromised patients - steroids, HTLV-1, immunosuppression): Massive larval dissemination throughout body; gram-negative bacteraemia (larvae carry gut bacteria through intestinal wall); meningitis; hepatitis; can be fatal
- Eosinophilia characteristic; may be absent in hyperinfection
F. TAPEWORMS (Cestodes)
| Species | Clinical Features |
|---|---|
| Taenia solium | Usually asymptomatic; passage of proglottids per rectum; cysticercosis (if eggs ingested) - neurocysticercosis = epilepsy, headache |
| Taenia saginata | Similar to T. solium but no cysticercosis risk; proglottids actively migrate out of anus |
| Diphyllobothrium latum | Usually asymptomatic; can cause Vitamin B12 deficiency (worm competes for ileal B12 absorption); megaloblastic anaemia; rarely neurological features |
| Hymenolepis nana | Commonest tapeworm worldwide; usually asymptomatic; diarrhoea, abdominal pain in heavy infections |
G. INTESTINAL FLUKES (Trematodes)
| Species | Transmission | Clinical Features |
|---|---|---|
| Fasciolopsis buski | Raw aquatic plants (water chestnuts) | Diarrhoea, abdominal pain, malabsorption |
| Heterophyes heterophyes | Raw fish | Mild diarrhoea, eosinophilia |
| Schistosoma mansoni | Cercariae penetrate skin in freshwater | Bloody diarrhoea, portal hypertension, hepatosplenomegaly (chronic) |
5. CLINICAL FEATURES SUMMARY
| Worm | Cardinal Signs | Characteristic Finding |
|---|---|---|
| Ascaris | Often asymptomatic / Loeffler's / intestinal obstruction | Worm in vomitus or stool; biliary colic |
| Trichuris | Dysentery + rectal prolapse (heavy load) | Bloody diarrhoea, tenesmus |
| Enterobius | Perianal nocturnal pruritus | Scotch tape test positive |
| Hookworm | Iron-deficiency anaemia, ground itch, Loeffler's | Hypochromic microcytic anaemia + eosinophilia |
| Strongyloides | Larva currens, midepigastric pain | Autoinfection; hyperinfection in immunocompromised |
| Taenia solium | Usually asymptomatic; proglottids in stool | Cysticercosis = epilepsy/seizures |
| D. latum | B12 deficiency | Megaloblastic anaemia |
6. DIAGNOSTIC APPROACH
Step 1: History
- Geographic origin / travel history (tropical, endemic areas)
- Barefoot outdoor exposure (hookworm, Strongyloides)
- Dietary habits (raw fish, pork, beef, vegetables)
- Contact with soil / playing in dirt
- Household contacts with similar symptoms
- Perianal itch (Enterobius)
- Immunosuppression status (critical for Strongyloides hyperinfection)
Step 2: Clinical Examination
- Growth assessment in children (stunting, weight)
- Pallor (iron deficiency / B12 deficiency anaemia)
- Oedema (hypoalbuminaemia in hookworm)
- Abdominal tenderness
- Rectal prolapse (heavy Trichuris)
- Skin: perianal excoriation (Enterobius), ground itch, larva currens
Step 3: Stool Examination (Primary Diagnostic Tool)
| Test | Method | Purpose |
|---|---|---|
| Stool microscopy - direct wet mount | Fresh stool + saline/iodine preparation | Identify eggs, larvae, proglottids |
| Formal-ether concentration technique | Formalin-ethyl acetate sedimentation | Increases sensitivity for light infections |
| Kato-Katz thick smear | Quantitative egg count | Estimates worm burden (eggs per gram of faeces); standard for STH (soil-transmitted helminth) surveys |
| Multiple stool samples | 3 samples on alternate days | Increases sensitivity (eggs not passed every day) |
| Species | Egg Characteristics |
|---|---|
| Ascaris | Elliptical, 35×55 µm; thick mammillated (bumpy) outer coat; golden-brown; fertilized = round inner content; unfertilized = irregular |
| Trichuris | Barrel/football-shaped; distinctive bipolar plugs (translucent knobs at both ends); thick brown shell; 50×22 µm |
| Hookworm | Oval, 40×60 µm; thin hyaline shell; contains 2-8-cell embryo in fresh stool; if stool old, may have hatched larvae |
| Enterobius | NOT found in stool routinely; asymmetrically flattened (planoconvex) shape; 55×25 µm; perianal swab needed |
| Strongyloides | Rhabditiform larvae in fresh stool (not eggs); distinguished from hookworm larvae by shorter buccal capsule and prominent genital primordium |
| Taenia | Proglottids visible in stool; eggs in proglottids: round, 30-40 µm, radially striated embryophore, contain oncosphere |
| D. latum | Operculated (lid-like cap); oval, 58-75 µm; yellowish-brown |
Step 4: Special Tests by Organism
| Test | Organism | Detail |
|---|---|---|
| Scotch tape (sellotape) test | Enterobius | Apply tape to perianal skin in morning before bathing → examine under microscope; high sensitivity for pinworm eggs |
| String test (Enterotest) | Ascaris larvae, Strongyloides | Swallowed gelatin capsule with string; examines duodenal fluid for larvae |
| Strongyloides serology (ELISA) | Strongyloides | Sensitivity ~95%; useful in endemic regions; cross-reactivity with other helminths |
| Modified Baermann technique / agar plate culture | Strongyloides | Culture of stool for larvae; more sensitive than direct microscopy |
| Serology (ELISA, Western blot) | Taenia solium cysticercosis, Echinococcus, Trichinella | Tissue phase/extraintestinal infections |
| PCR/NAAT | Hookworm species differentiation; Strongyloides | Research/reference labs; improving sensitivity and specificity |
| Peripheral eosinophilia | All tissue-migrating helminths | Significant eosinophilia (>500/µL, up to 50-60% in some) during larval migration; absent or mild when adults confined to intestinal lumen |
Step 5: Additional Investigations
| Investigation | Purpose |
|---|---|
| FBC | Anaemia (iron-deficiency, megaloblastic), eosinophilia |
| Serum iron, ferritin, TIBC | Iron-deficiency from hookworm |
| Serum B12, folate | D. latum infestation |
| Serum albumin | Protein-losing enteropathy (hookworm, severe Trichuris) |
| Abdominal X-ray/USS | Ascaris obstruction (worm shadows), biliary involvement |
| CT/MRI brain | Neurocysticercosis (Taenia solium) |
| Chest X-ray | Loeffler's syndrome (Ascaris/hookworm migration) - transient infiltrates |
| Endoscopy | Hookworm (duodenal punctate erosions, pooled blood); Anisakiasis (direct visualization, extraction); Ascaris in bile duct on ERCP |
7. MANAGEMENT
General Principles
- Anthelmintic therapy - mainstay
- Nutritional rehabilitation - iron, protein, vitamins
- Treat household contacts (Enterobius - all members simultaneously)
- Sanitation and hygiene measures - prevent reinfection
- Mass Drug Administration (MDA) programs in endemic areas - albendazole/mebendazole annually for school-aged children (WHO-recommended deworming)
8. PHARMACOLOGY OF ANTHELMINTICS
A. BENZIMIDAZOLES
Albendazole (Albenza, Zentel) - Broad-spectrum, Drug of Choice
-
Mechanism of Action:
- Binds to β-tubulin of helminth → inhibits tubulin polymerization → disrupts microtubule assembly → impairs glucose uptake and transport → depletes glycogen stores → immobilization and death of worm
- Also inhibits fumarate reductase (helminth mitochondrial enzyme) → impairs energy production
- Absorbed systemically → reaches worm's head buried in gut wall (superior to mebendazole for Trichuris)
- Active metabolite: Albendazole sulphoxide - pharmacologically active; penetrates blood-brain barrier (useful for cysticercosis)
-
Spectrum and Doses (Goldman-Cecil Table 327-1):
| Parasite | Dose |
|---|---|
| Ascaris lumbricoides | 400 mg single dose |
| Hookworm | 400 mg OD × 3 days |
| Trichuris trichiura | 400 mg OD × 3 days |
| Enterobius vermicularis | 400 mg single dose, repeated in 2 weeks |
| Strongyloides stercoralis | 400 mg BD × 7 days (alternative to ivermectin) |
| Taenia (tapeworms) | 400 mg BD × 28 days (cysticercosis) |
| Capillaria philippinensis | 400 mg BD × 10 days |
| Trichostrongylus | 400 mg OD × 10 days |
| Cutaneous larva migrans | 400 mg OD × 3 days |
- ADME: Well absorbed with fatty meals; extensive first-pass hepatic metabolism to albendazole sulphoxide (active); t½ 8-12 hours; biliary excretion
- Adverse Effects: Generally well tolerated; nausea, abdominal pain; elevated liver enzymes (monitor in prolonged courses); bone marrow suppression (rare, with prolonged use); teratogenic - contraindicated in pregnancy (Category D); alopecia
Mebendazole (Vermox)
- Mechanism: Same as albendazole - binds β-tubulin → inhibits microtubule polymerization → blocks glucose uptake
- Poorly absorbed from GI tract (acts locally in intestinal lumen) - therefore less effective when the worm's head is embedded in mucosa (e.g., Trichuris)
- Doses:
- Ascaris: 500 mg single dose or 100 mg BD × 3 days
- Hookworm: 500 mg OD or 100 mg BD × 3 days
- Trichuris: 100 mg BD × 3 days (albendazole preferred)
- Enterobius: 100 mg single dose, repeat in 2 weeks
- Adverse Effects: Generally well tolerated; mild GI upset; teratogenic (avoid in first trimester)
B. MACROCYCLIC LACTONES
Ivermectin (Stromectol) - Drug of Choice for Strongyloides
- Mechanism of Action:
- Binds to glutamate-gated chloride ion channels (invertebrate-specific) in nerve and muscle cells of helminths
- Also potentiates GABA-gated chloride channels → hyperpolarization → paralysis → death of parasite
- Does NOT cross the human blood-brain barrier at therapeutic doses (BBB excludes ivermectin via P-glycoprotein)
- Spectrum and Doses:
| Parasite | Dose |
|---|---|
| Strongyloides stercoralis (uncomplicated) | 200 µg/kg OD × 2 days (drug of choice) |
| Strongyloides hyperinfection | 200 µg/kg OD × 2 days (repeat courses; until negative stool) |
| Ascaris | 150-200 µg/kg single dose (alternative) |
| Onchocerciasis | 150 µg/kg single dose annually |
| Trichuris (addition to albendazole) | 200 µg/kg OD × 3 days (improves efficacy) |
| Cutaneous larva migrans | 200 µg/kg OD × 1-2 days |
- ADME: Oral; peak concentration 4 hours; t½ ~18 hours; hepatic metabolism; fecal excretion
- Adverse Effects: Generally very well tolerated; Mazzotti reaction (fever, pruritus, rash, hypotension) in microfilaraemic patients with onchocerciasis; CNS toxicity if BBB compromised (avoid in meningitis, concurrent CNS disease, Loa loa co-infection with high microfilaraemia)
- Note: Contraindicated in pregnancy; caution in children <15 kg
Moxidectin
- Newer macrocyclic lactone; similar mechanism to ivermectin
- Ascaris: 8 mg single dose
- Trichuris: 8 mg OD × 3 days (in combination with albendazole)
C. PYRANTEL PAMOATE (Combantrin)
- Mechanism: Depolarising neuromuscular blocking agent - acts as nicotinic acetylcholine receptor agonist → persistent activation → spastic paralysis of worm → expelled by normal intestinal peristalsis
- Poorly absorbed from GI tract - acts locally
- Doses:
- Ascaris, Enterobius: 11 mg/kg single dose (max 1 g)
- Hookworm (heavy burden): 11 mg/kg × 3 days
- Trichostrongylus: 11 mg/kg single dose
- Enterobius: Repeat after 2 weeks
- Adverse Effects: Mild nausea, vomiting, diarrhoea, headache; generally very safe
- Contraindication: Do NOT combine with piperazine (antagonistic - piperazine causes flaccid paralysis vs. pyrantel's spastic paralysis)
D. PIPERAZINE
- Mechanism: GABA agonist → opens Cl⁻ channels → flaccid paralysis of worm musculature → worm expelled alive by peristalsis
- Used for Ascaris and Enterobius when other agents unavailable
- Largely replaced by safer agents
E. PRAZIQUANTEL (Biltricide) - Drug of Choice for Cestodes and Trematodes
- Mechanism:
- Increases Ca²⁺ permeability of parasite cell membrane → influx of calcium → tetanic spasm/paralysis of worm musculature
- Also damages worm tegument → exposes worm surface to immune attack
- Doses:
- Taenia (tapeworms): 5-10 mg/kg single dose
- Intestinal flukes (Fasciolopsis, Heterophyes): 25 mg/kg TDS × 1 day
- Schistosoma: 40 mg/kg in 2 divided doses (S. mansoni/haematobium); 60 mg/kg in 3 doses (S. japonicum)
- Clonorchis/Opisthorchis: 25 mg/kg TDS × 1 day
- ADME: Well absorbed orally; extensive first-pass hepatic metabolism; t½ ~1.5 hours
- Adverse Effects: Nausea, headache, dizziness, abdominal pain (Mazzotti-like reactions); generally transient; caution in neurocysticercosis (may trigger inflammatory reaction around dying cysts - use corticosteroids)
F. TRICLABENDAZOLE (Egaten)
- Mechanism: Benzimidazole that uniquely inhibits tubulin in Fasciola (not nematodes)
- Treats fascioliasis: 10 mg/kg × 2 doses on consecutive days
- Also used for paragonimiasis
G. NICLOSAMIDE
- Mechanism: Inhibits mitochondrial ATP synthesis in tapeworms by uncoupling oxidative phosphorylation → kills worm scolex (head) → worm detaches
- Used for tapeworms (Taenia, D. latum, H. nana): 2 g single dose (chewed)
- Now largely replaced by praziquantel
H. DILOXANIDE FUROATE (Luminal Amoebiocide - also used for some protozoa)
- Not for helminths; cross-referenced as it may appear in parasite tables
I. TREATMENT SUMMARY TABLE (Goldman-Cecil, Table 327-1)
| Nematode | First-Line | Alternative |
|---|---|---|
| Ascaris lumbricoides | Albendazole 400 mg once | Mebendazole 500 mg once; ivermectin 150-200 µg/kg once; moxidectin 8 mg once; pyrantel pamoate 11 mg/kg once (max 1 g) |
| Hookworm | Albendazole 400 mg OD × 3 days | Tribendimidine 400 mg once; mebendazole 500 mg OD or 100 mg BD × 3 days; pyrantel pamoate 11 mg/kg × 3 days |
| Trichuris trichiura | Albendazole 400 mg OD × 3 days | Mebendazole 100 mg BD × 3 days; add ivermectin 200 µg/kg or moxidectin 8 mg × 3 days to improve efficacy |
| Enterobius vermicularis | Pyrantel pamoate 11 mg/kg once, repeat in 2 weeks | Mebendazole 100 mg once or albendazole 400 mg once, both repeated in 2 weeks |
| Strongyloides stercoralis | Ivermectin 200 µg/kg OD × 2 days (drug of choice) | Albendazole 400 mg BD × 7 days (less effective) |
| Capillaria philippinensis | Albendazole 400 mg BD × 10 days | Mebendazole 500 mg OD × 20 days |
| Trichostrongylus | Pyrantel pamoate 11 mg/kg once | Albendazole 400 mg OD × 10 days; mebendazole 500 mg OD × 10 days |
| Taenia (tapeworm) | Praziquantel 5-10 mg/kg once | Niclosamide 2 g once |
| Intestinal flukes | Praziquantel 25 mg/kg TDS × 1 day | |
| Schistosoma | Praziquantel 40-60 mg/kg |
J. Adjunct Pharmacological Treatments
| Drug | Purpose |
|---|---|
| Ferrous sulphate / Iron supplementation | Hookworm-induced iron-deficiency anaemia; 200 mg TDS until stores replenished |
| Cyanocobalamin (Vitamin B12) | Diphyllobothrium-induced B12 deficiency |
| Nutritional supplements | Protein, zinc, vitamins in malnourished children with heavy worm burdens |
| Corticosteroids | Inflammatory complications of cysticercosis, Trichinella (myocarditis, encephalitis), severe Loeffler's syndrome |
| Antiepileptics | Neurocysticercosis with seizures |
9. PREVENTION AND PUBLIC HEALTH
| Measure | Target |
|---|---|
| Mass Drug Administration (WHO) | Albendazole 400 mg or mebendazole 500 mg annually for school-age children in endemic areas |
| Sanitation (safe disposal of faeces) | Breaks fecal-oral cycle; prevents all soil-transmitted helminths |
| Wearing footwear | Prevents hookworm and Strongyloides skin penetration |
| Hand hygiene | Prevents Enterobius, Ascaris, Trichuris fecal-oral transmission |
| Proper cooking of meat (≥65°C internal) | Prevents Taenia, Trichinella |
| Treat household contacts simultaneously | Enterobius - all members treated; bedding washed in hot water |
| Wash vegetables/fruits | Removes Ascaris/Trichuris eggs from soil-contaminated produce |
| Safe drinking water | Prevents Diphyllobothrium, Ascaris, amoebiasis |
- Harrison's Principles of Internal Medicine 22E - Chapters 236-240 (all intestinal helminths); Table 327-1 (treatment doses)
- Goldman-Cecil Medicine - Table 327-1 Oral Treatment of Intestinal Nematodes
- Sherris & Ryan Medical Microbiology 8th Ed - Chapter 54 (Ascaris, Trichuris, Enterobius, Hookworm, Strongyloides life cycles and pathogenesis)
- Yamada's Textbook of Gastroenterology 7th Ed - Chapter 147 (hookworm clinical manifestations, diagnosis, treatment)
- Goodman & Gilman's - Anthelmintic pharmacology (benzimidazoles, ivermectin, praziquantel, pyrantel pamoate)
provide defenition, types, causes, pathology, diagnostic approach , management along with pharmacology for UTI
Urinary Tract Infection (UTI): Complete Clinical Guide
1. DEFINITION
| Term | Definition |
|---|---|
| Bacteriuria | Detection of bacteria in urine; clinically significant at ≥10⁵ organisms/mL (may be as low as 10² CFU/mL if symptoms + pyuria present) |
| Asymptomatic bacteriuria (ASB) | ≥10⁵ organisms/mL WITHOUT symptoms |
| Pyuria | ≥10 WBCs/mm³ in uncentrifuged urine; accompanies infection |
| Significant bacteriuria | ≥10⁵ CFU/mL → 95% likelihood of infection; 10⁴ CFU/mL → 50% likelihood |
| Cystitis | Infection confined to the bladder (lower UTI) |
| Pyelonephritis | Infection of the renal parenchyma and collecting system (upper UTI) |
| Urosepsis | Systemic sepsis arising from urinary tract source |
2. TYPES / CLASSIFICATION
A. By Anatomical Location
| Type | Location | Symptoms |
|---|---|---|
| Lower UTI | Urethra, bladder, prostate | Dysuria, frequency, urgency, suprapubic pain, haematuria; NO fever |
| Urethritis | Urethra | Dysuria, urethral discharge; often STI-related |
| Cystitis | Bladder mucosa | Frequency, urgency, dysuria, suprapubic pain/pressure |
| Prostatitis | Prostate | Perineal pain, voiding symptoms, fever (acute) |
| Upper UTI | Ureters, renal pelvis, parenchyma | Fever, rigors, flank/loin pain, CVA tenderness |
| Pyelonephritis | Renal parenchyma + collecting system | Fever >38°C, flank pain, nausea/vomiting, CVA tenderness |
B. By Complexity
| Type | Definition | Key Features |
|---|---|---|
| Uncomplicated UTI | In a non-pregnant individual with structurally and functionally normal urinary tract | Short course antibiotics sufficient |
| Complicated UTI | Associated with structural/functional abnormality, instrumentation, transplantation, or systemic disease (DM, renal insufficiency, immunodeficiency) | Longer antibiotic course; full investigation needed |
C. By Course
| Type | Definition |
|---|---|
| Acute/isolated UTI | Single episode |
| Recurrent UTI | ≥2 episodes in 6 months OR ≥3 episodes in 12 months |
| Relapse | Same organism re-infects within 2 weeks of completing treatment (incomplete eradication) |
| Reinfection | New infection with different organism or same organism >2 weeks after treatment |
| Bacterial persistence | Organism persists despite appropriate antibiotic therapy; suggests structural abnormality |
3. CAUSES AND RISK FACTORS
Causative Organisms
| Organism | Frequency | Notes |
|---|---|---|
| Escherichia coli | 75-90% of acute cystitis in young women; >70% of all UTIs | Most virulent strains have Type 1 and P (Pap) fimbriae for uroepithelial adhesion |
| Staphylococcus saprophyticus | 10-20% of acute cystitis in young women | Skin commensal; second most common in young sexually active women; does NOT convert nitrate to nitrite |
| Klebsiella pneumoniae | 5-10% | Common in complicated/hospital UTI |
| Proteus mirabilis | 5% | Urea-splitter → alkaline urine → struvite stones; common in diabetic women/obstruction |
| Enterococcus spp. | 5% | |
| Pseudomonas aeruginosa | Hospital/catheter UTI | |
| Staphylococcus aureus | Haematogenous seeding | |
| Candida spp. | Catheterised patients |
Risk Factors
- Short urethra (anatomical - opens near vulva and perirectal area)
- Sexual activity, new sexual partner
- Spermicide use (disrupts vaginal flora, promotes E. coli colonisation)
- Prior UTI; family history of UTI (possible inherited urethral anatomy)
- Postmenopausal status (oestrogen deficiency → loss of Lactobacillus protection)
- Pregnancy (physiological urinary stasis; dilated ureters; progesterone smooth muscle relaxation)
- Diabetes mellitus
- High postvoid residual (incomplete emptying)
- Urological abnormalities (BPH, urethral stricture)
- Unretracted foreskin
- Male homosexuality (rectal E. coli)
- Lack of circumcision
- Urinary tract obstruction (calculi, stricture, tumour, BPH)
- Urinary instrumentation (catheterisation, cystoscopy)
- Vesicoureteral reflux
- Neurogenic bladder
- Immunosuppression (HIV, steroids, transplant)
- Hospital/nursing home setting
- Diabetes mellitus
4. PATHOPHYSIOLOGY AND PATHOLOGY
Route of Infection
- Colonisation of periurethral/perirectal area by enteric/vaginal flora (predominantly E. coli)
- Colonisation of urethra → bladder ascent (facilitated by short female urethra; sexual intercourse; instrumentation)
- Bladder infection (cystitis) → may ascend ureters to renal pelvis → pyelonephritis
- The most common mechanism in pregnancy is ascending infection from perineal bacteria with fimbriated E. coli attaching to uroepithelial cells
Virulence Factors of Uropathogens (E. coli)
| Factor | Role |
|---|---|
| Type 1 fimbriae (mannose-sensitive) | Attachment to uroepithelial mannose receptors |
| P fimbriae (Pap fili; mannose-resistant) | Bind to globosides on uroepithelium and red blood cells; major virulence factor in pyelonephritis |
| Haemolysin | Cytotoxin that lyses red blood cells and provides iron |
| Aerobactin | Siderophore; scavenges iron |
| K antigen (capsular polysaccharide) | Resists phagocytosis and complement |
| LPS (O antigen) | Triggers inflammatory response |
Host Defence Mechanisms (and their Failure)
- Urine flow (mechanical flushing) - impaired by obstruction, incomplete voiding
- Urinary pH, osmolality, organic acids
- Tamm-Horsfall protein (uromodulin) - binds bacteria; first-line defence
- Urothelial tight junctions - barrier
- Secretory IgA in urine
- Vaginal Lactobacillus flora in women - maintains acidic pH, produces H₂O₂
Pathology
- Mucosal erythema, oedema, petechiae
- Superficial infection of bladder mucosa - hence no systemic fever
- Microscopy: epithelial cell vacuolation, submucosa oedema, neutrophilic infiltrate
- Gross: kidney swollen, focal yellow-white abscesses on cortex (wedge-shaped)
- Micro: suppurative (neutrophilic) infiltrate in interstitium, tubules, collecting ducts; tubular necrosis; glomeruli relatively spared; pus-filled tubules
- Cortical abscesses when severe → renal carbuncle
- Complications: perinephric abscess, emphysematous pyelonephritis (gas-forming organisms in diabetics - life-threatening)
- Gross: coarse irregular corticomedullary scars; deformed calyces
- Micro: interstitial fibrosis, tubular atrophy, mononuclear infiltrate; "thyroidisation" (colloid casts in atrophic tubules resembling thyroid tissue)
- Occurs with vesicoureteric reflux (reflux nephropathy) or obstruction
- Xanthogranulomatous pyelonephritis: Lipid-laden macrophages (foam cells) replace renal parenchyma; associated with Proteus or E. coli + obstructing calculus; can mimic renal carcinoma
- Malacoplakia: Soft yellowish plaques of macrophages containing Michaelis-Gutmann bodies (calcified bacterial remnants); rare
- Emphysematous cystitis/pyelonephritis: Gas in bladder wall or renal parenchyma by glucose-fermenting organisms (E. coli, Klebsiella); mainly diabetics
5. CLINICAL FEATURES
Uncomplicated Cystitis (Lower UTI)
- Dysuria (burning/stinging on micturition) - single most reliable symptom
- Urinary frequency (voiding small amounts frequently)
- Urgency (sudden, compelling desire to void)
- Suprapubic pain or pressure
- Haematuria (visible or microscopic)
- Nocturia
- Foul-smelling or cloudy urine (non-specific)
- NO fever, chills, or systemic symptoms
- Combination of dysuria + frequency predicts UTI in >90% of cases (in absence of vaginal discharge)
Acute Pyelonephritis (Upper UTI)
- Fever (≥38°C) - often high-spiking with rigors
- Flank/loin pain (unilateral or bilateral)
- Costovertebral angle tenderness (CVAT) on examination
- Nausea, vomiting
- Lower urinary tract symptoms (dysuria, frequency) - may precede or accompany
- Systemic toxaemia: malaise, myalgia, headache
- In pregnancy: right-sided predominance (right ureter more dilated)
- May progress to urosepsis → septic shock (10-20% mortality)
Prostatitis
- Acute bacterial prostatitis: Fever, chills, perineal/pelvic pain, dysuria, urinary retention, tender boggy prostate on PR (do NOT massage - bacteraemia risk)
- Chronic bacterial prostatitis: Voiding symptoms, low back and perineal pain, myalgias; recurrent UTIs in men
Asymptomatic Bacteriuria (ASB)
- No symptoms; detected on routine screening
- Treat in: Pregnant women, immunosuppressed, prior to urological procedures
- Do NOT treat in: Elderly, catheterised patients, diabetics (unless symptomatic) - treatment increases resistant organisms without clinical benefit
6. DIAGNOSTIC APPROACH
Step 1: History
- Symptoms (onset, duration, character)
- Previous UTIs, recurrence pattern
- Sexual activity, spermicide use
- Pregnancy status
- Prior urological procedures, catheterisation
- Antibiotic use history (resistance risk)
- Comorbidities: DM, immunosuppression, renal disease
Step 2: Physical Examination
- Temperature (fever → upper UTI)
- Abdominal palpation - suprapubic tenderness
- CVA tenderness (CVAT) - hallmark of pyelonephritis
- PR examination in men (prostate tenderness/size)
- Pelvic examination in women (to exclude vaginitis, cervicitis)
Step 3: Urinalysis (Primary Diagnostic Test)
| Test | Significance |
|---|---|
| Nitrite | Converted from nitrate by gram-negative bacteria (E. coli, Klebsiella, Proteus); high specificity (~95%); NOT produced by S. saprophyticus or Enterococcus |
| Leukocyte esterase (LE) | Enzyme released by neutrophils; indicates pyuria; marker of inflammation |
| Both LE + nitrite positive | Specificity nearly 100% for UTI |
| Both LE + nitrite negative | When pretest probability low → reliably excludes UTI; when strongly suspected clinically → send urine culture regardless |
| Blood (haematuria) | Supportive of UTI |
| Protein | Renal involvement in pyelonephritis |
- Pyuria: ≥10 WBCs/mm³ (haemocytometer) - present in nearly all UTIs from coliforms
- Bacteria on microscopy: Most reliable test; Gram stain may identify organism class
- WBC casts: Highly specific for pyelonephritis (casts formed in renal tubules)
- RBC casts: Glomerulonephritis (distinguish from UTI)
- Positive culture: ≥10⁵ CFU/mL (conventional); ≥10³ CFU/mL acceptable with classic symptoms
- Identifies organism and antibiotic sensitivities (C&S)
- When to send culture:
- Pyelonephritis
- Complicated UTI
- Recurrent or relapsing UTI
- Pregnant women
- Suspected multidrug-resistant organism
- Men with UTI
- No improvement after 48-72 hours of treatment
- NOT required for uncomplicated cystitis in young women with typical symptoms
- Mid-stream clean catch (MSCC) urine - most common
- Catheter specimen (for inpatients/catheterised patients)
- Suprapubic aspiration (gold standard for infants and equivocal cases - any growth significant)
Step 4: Blood Tests (for Pyelonephritis/Complicated UTI)
| Test | Purpose |
|---|---|
| FBC (CBC) | Leukocytosis with neutrophilia (bacterial infection) |
| CRP / PCT (Procalcitonin) | Raised in pyelonephritis and urosepsis; PCT useful to guide antibiotic duration |
| Serum urea, creatinine, eGFR | Assess renal function (AKI in severe pyelonephritis) |
| Blood cultures | Pyelonephritis with fever/rigors (positive in ~10-20%); acute bacterial prostatitis; urosepsis |
| Serum electrolytes | Na⁺, K⁺ in sepsis/AKI |
| LFTs | Hepatic involvement in sepsis |
| Blood glucose / HbA1c | Diabetes screen |
Step 5: Imaging
| Investigation | Indication | Findings |
|---|---|---|
| Ultrasound (renal + bladder) | First-line imaging; pyelonephritis with no improvement after 48-72h; obstructive symptoms; recurrent UTI | Hydronephrosis, hydroureter, abscesses, calculi, postvoid residual, congenital anomalies |
| CT abdomen/pelvis (non-contrast) | Suspected calculi, abscess, obstruction, emphysematous pyelonephritis; failure to respond | Shows renal/perinephric abscess; gas in emphysematous pyelonephritis; calculi; hydronephrosis |
| CT with contrast (CT-IVU) | Complex/complicated UTI; mass lesion query | Renal enhancement patterns in pyelonephritis; abscesses |
| MCUG (voiding cystourethrogram) | Children with recurrent UTI | Vesicoureteric reflux |
| DMSA scan | Renal scarring in children | Cortical scarring, relative function assessment |
| Cystoscopy | Recurrent/complicated UTI with risk factors (Table 55.9) | Bladder lesion, tumour, fistula, calculi |
- Previous urinary trauma/surgery
- Previous bladder/renal calculi
- Gross haematuria after resolution of infection
- Obstructive symptoms; high PVR
- Urea-splitting organisms on culture
- Immunocompromise/DM
- Repeated pyelonephritis
- Bacterial persistence despite sensitivity-based therapy
7. MANAGEMENT
General Measures (All UTIs)
- Increased fluid intake (2-3 L/day) - dilutes urine, flushes bacteria
- Urinary analgesic: Phenazopyridine (bladder-specific local anaesthetic) for dysuria symptom relief (colours urine orange; max 2 days)
- Complete the full antibiotic course
- Treat underlying risk factors (calculi, obstruction, DM control)
- Remove/change urinary catheters where possible
- Follow-up culture (test of cure) for pregnant women, recurrent UTI, pyelonephritis
8. PHARMACOLOGY
A. Treatment of Uncomplicated Cystitis (Lower UTI)
1. Nitrofurantoin (Macrobid, Macrodantin)
- Mechanism: Complex mechanism not fully understood; rapidly reduced intracellularly by bacterial nitroreductases to highly reactive intermediates → damage bacterial DNA, ribosomes, and multiple enzyme systems; both bacteriostatic and bactericidal (concentration-dependent)
- Spectrum: Gram-negatives (E. coli, Klebsiella, Enterobacteriaceae), Enterococci; NOT effective against Proteus, Pseudomonas, or Serratia
- Dose: Nitrofurantoin macrocrystals (Macrobid): 100 mg BD × 5 days (uncomplicated cystitis)
- ADME: Rapidly absorbed; concentrates only in urine (not in serum or tissues) → NOT suitable for upper UTI, pyelonephritis, bacteraemia, or systemic infections
- Advantages: Minimal effects on bowel or vaginal flora; exceedingly low acquired resistance in E. coli; inexpensive
- Adverse Effects: GI upset (take with food); pulmonary reactions (acute hypersensitivity pneumonitis or chronic pulmonary fibrosis - with prolonged use); peripheral neuropathy (long-term); hepatotoxicity (rare); haemolytic anaemia in G6PD deficiency
- Contraindications: eGFR <30 mL/min (inadequate urinary concentrations; accumulation of toxic metabolites); pregnancy at term (≥38 weeks) and first trimester when alternatives available; G6PD deficiency
- Avoid in: Pyelonephritis (does NOT achieve adequate tissue levels)
2. Trimethoprim-Sulfamethoxazole (TMP-SMX / Co-trimoxazole)
- Mechanism:
- Sulfamethoxazole: Structural analogue of PABA → competitively inhibits dihydropteroate synthase → blocks dihydrofolic acid synthesis
- Trimethoprim: Inhibits dihydrofolate reductase → blocks conversion of dihydrofolate to tetrahydrofolate (active form)
- Sequential blockade of the same folate pathway = synergistic bactericidal effect (50:1 ratio in SMX:TMP in co-trimoxazole)
- Human cells unaffected because they use dietary preformed folate
- Dose: 160/800 mg (one DS tablet) BD × 3 days (uncomplicated cystitis)
- Spectrum: E. coli, Klebsiella, Enterobacteriaceae; Staphylococci; Listeria; Pneumocystis
- Adverse Effects: GI upset; Stevens-Johnson syndrome (severe - rare); bone marrow suppression; hyperkalaemia (trimethoprim blocks renal K⁺ secretion); crystalluria; megaloblastic anaemia (folate deficiency with prolonged use)
- Contraindications: Pregnancy (first trimester - sulfonamides may cause foetal haemolysis and hyperbilirubinaemia; third trimester - risk of kernicterus); G6PD deficiency; severe renal failure
- Note: Rising resistance (up to 20-30% in some regions); check local antibiogram before empirical use
3. Fosfomycin Trometamol (Monurol)
- Mechanism: Inhibits MurA (UDP-N-acetylglucosamine enolpyruvyl transferase) → blocks the first step in peptidoglycan cell wall synthesis; bactericidal
- Dose: 3 g sachet as a SINGLE ORAL DOSE (uncomplicated cystitis); single dose is highly effective and improves compliance
- Spectrum: E. coli, Enterococcus faecalis; active against some ESBL-producers and VRE
- ADME: Well absorbed; concentrates in urine; urinary concentrations maintained for 24-48 hours after single dose
- Advantages: Single-dose therapy; active against multidrug-resistant organisms; safe in pregnancy
- Adverse Effects: Diarrhoea, nausea; headache
- Not effective for: Pyelonephritis (inadequate tissue levels)
B. Treatment of Uncomplicated Pyelonephritis (Upper UTI - Outpatient)
4. Fluoroquinolones (First-Line for Outpatient Pyelonephritis)
Ciprofloxacin
- Mechanism: Inhibits bacterial DNA gyrase (topoisomerase II) and topoisomerase IV → prevents DNA supercoiling, replication, and repair → stabilises DNA-enzyme complex → lethal double-strand DNA breaks; bactericidal
- Dose: Ciprofloxacin XR 500-1000 mg OD × 7 days (pyelonephritis); or Ciprofloxacin 500 mg BD × 7 days
- Spectrum: Excellent against gram-negatives (E. coli, Klebsiella, Proteus, Pseudomonas); Staphylococci
- Advantages: Excellent tissue penetration including prostate (first-line for prostatitis); excellent urinary concentrations
- Adverse Effects: GI disturbances; CNS effects (dizziness, headache, seizures - rare); tendinopathy/tendon rupture (especially Achilles; risk with age >60, steroids); peripheral neuropathy; prolonged QT interval; photosensitivity; cartilage damage (avoid in children and pregnancy); Clostridioides difficile
- Resistance: Chromosomal mutations in DNA gyrase/topoisomerase IV; plasmid-mediated PMQR genes; up to 20-30% resistance in some regions; 80% resistance in transplant units using prophylactic fluoroquinolones
- Contraindications: Pregnancy, children, myasthenia gravis; caution with QT-prolonging drugs
Levofloxacin
- Third-generation fluoroquinolone; enhanced gram-positive activity vs. ciprofloxacin
- Dose: 250-500 mg OD × 7-10 days (uncomplicated pyelonephritis); 750 mg OD × 5 days (complicated)
C. Treatment of Complicated UTI / Severe Pyelonephritis (Inpatient IV Therapy)
5. Third/Fourth-Generation Cephalosporins
Ceftriaxone
- Mechanism: Beta-lactam; binds Penicillin-Binding Proteins (PBPs) → inhibits transpeptidation step in peptidoglycan cross-linking → cell wall synthesis blocked → osmotic lysis
- Dose: 1-2 g IV once daily (pyelonephritis, urosepsis); first IV dose for severe pyelonephritis requiring admission
- Spectrum: Excellent gram-negative coverage (E. coli, Klebsiella, Proteus); limited Pseudomonas; Staphylococci (not MRSA)
- Adverse Effects: Hypersensitivity; GI disturbance; biliary sludge; cholecystitis (with high doses or prolonged use)
Cefepime (4th gen)
- Extended gram-negative coverage including Pseudomonas
- Dose: 1-2 g IV every 8-12 hours
- Used for complicated UTI/pyelonephritis
6. Aminoglycosides
Gentamicin / Amikacin
- Mechanism: Binds irreversibly to 30S ribosomal subunit → inhibits protein synthesis → causes mRNA misreading → insertion of wrong amino acids → dysfunctional proteins; also disrupts cell membrane
- Dose: Gentamicin 3-5 mg/kg/day IV (once-daily dosing preferred; monitor trough levels); Amikacin 15 mg/kg/day
- Advantages: Excellent urinary concentrations; bactericidal; active against Pseudomonas
- Adverse Effects: Nephrotoxicity (tubular necrosis; monitor creatinine); ototoxicity (vestibular > cochlear); avoid in pre-existing renal failure
- Use: Second-line; complicated UTI; hospital-acquired UTI
7. Piperacillin-Tazobactam
- Mechanism: Piperacillin (anti-pseudomonal penicillin) + tazobactam (beta-lactamase inhibitor) → protects from enzymatic inactivation
- Dose: 4.5 g IV every 6-8 hours
- Spectrum: Broad gram-negative including Pseudomonas; gram-positive; anaerobes
- Use: Complicated/hospital UTI; Pseudomonas UTI; ESBL-producing organisms (some strains)
8. Carbapenems
Meropenem / Imipenem-Cilastatin / Ertapenem
- Mechanism: Beta-lactam with broadest spectrum; stable to most beta-lactamases including ESBLs; binds PBPs → cell wall synthesis inhibition
- Use: Multidrug-resistant UTI (ESBL producers, carbapenem-sensitive Klebsiella); last resort for complicated UTI
- Dose: Meropenem 500 mg-1 g IV every 8 hours; Ertapenem 1 g IV once daily
D. Treatment of Specific UTI Types
Trimethoprim (alone - used in UK)
- Mechanism: Inhibits dihydrofolate reductase alone
- Dose: 200 mg BD × 3 days (uncomplicated cystitis); or 100 mg ON for prophylaxis
- Commonly used in the UK as first-line for uncomplicated UTI
Nitrofurantoin vs Trimethoprim for Uncomplicated Cystitis (Efficacy)
- Both have ~85-90% clinical cure rates for uncomplicated cystitis
- Nitrofurantoin preferred when TMP-SMX resistance is >20% locally
E. Antibiotic Selection by UTI Type - Treatment Summary
| UTI Type | First-Line | Duration | Alternative |
|---|---|---|---|
| Uncomplicated cystitis (women) | Nitrofurantoin 100 mg BD, OR TMP-SMX 160/800 mg BD, OR Fosfomycin 3 g single dose | 5 days; 3 days; 1 dose | Trimethoprim 200 mg BD × 3 days |
| Uncomplicated pyelonephritis (outpatient) | Ciprofloxacin 500 mg BD, OR Levofloxacin 500 mg OD | 7 days | TMP-SMX 160/800 mg BD × 14 days (if susceptible) |
| Pyelonephritis (inpatient IV → oral) | Ceftriaxone 1-2 g IV OD → step down to oral once afebrile | 7-14 days total | Piperacillin-tazobactam; aminoglycosides |
| Complicated UTI | Based on C&S; Ciprofloxacin IV or ceftriaxone IV | 7-14 days (up to 4-6 weeks if abscess) | Meropenem (MDR organisms) |
| Urosepsis | IV ceftriaxone ± aminoglycoside, OR piperacillin-tazobactam | 14 days minimum | Meropenem; imipenem |
| Prostatitis (acute bacterial) | Ciprofloxacin 500 mg BD or Levofloxacin 500 mg OD | 4-6 weeks | Ceftriaxone IV until afebrile, then oral fluoroquinolone |
| Chronic bacterial prostatitis | Fluoroquinolone (ciprofloxacin or levofloxacin) | 4-6 weeks | TMP-SMX 160/800 BD × 4-6 weeks |
| ASB in pregnancy | Cephalexin 500 mg BD, OR Nitrofurantoin 100 mg BD, OR Fosfomycin 3 g single dose | 7 days (or as indicated) | Amoxicillin (if susceptible) |
| Pyelonephritis in pregnancy | Ceftriaxone IV → oral when afebrile | 14 days | Cefepime IV; aztreonam; piperacillin-tazobactam (avoid fluoroquinolones) |
| Catheter-associated UTI (CAUTI) | Based on C&S; fluoroquinolone or cephalosporin | 7 days (if prompt response) | Remove/replace catheter first |
F. Drugs for Recurrent UTI Prophylaxis
| Drug | Dose | Notes |
|---|---|---|
| Nitrofurantoin | 50-100 mg ON | Continuous prophylaxis for recurrent UTI; most commonly used |
| Trimethoprim | 100 mg ON | Effective prophylaxis; resistance may emerge |
| TMP-SMX | 40/200 mg ON | Effective but resistance concern |
| Fosfomycin | 3 g every 10 days | Alternative prophylaxis |
| Post-coital prophylaxis | Single dose of nitrofurantoin or TMP after intercourse | For women with coitally-triggered recurrent UTI |
G. Non-Antibiotic Approaches for Recurrent UTI Prevention
| Approach | Evidence | Mechanism |
|---|---|---|
| Cranberry products | Moderate evidence | Proanthocyanidins block Type 1 fimbriae - prevent bacterial adhesion |
| Vaginal oestrogen (postmenopausal) | Good evidence | Restores Lactobacillus-dominant vaginal flora; lowers vaginal pH |
| D-Mannose | Emerging evidence | Competes with uroepithelial mannose receptors for Type 1 fimbriae binding |
| Lactobacillus probiotics | Emerging | Restore protective vaginal flora |
| Methenamine hippurate | UK-used; low resistance risk | Converted to formaldehyde in acidic urine → bactericidal |
9. SPECIAL POPULATIONS
| Population | Key Consideration |
|---|---|
| Pregnant women | Screen all at 12-16 weeks; treat ASB; avoid fluoroquinolones; avoid nitrofurantoin at term (≥38 wks); treat pyelonephritis with IV cephalosporin |
| Elderly | ASB common and does NOT require treatment; UTI can present atypically (confusion, falls); avoid nitrofurantoin if CrCl <30 mL/min |
| Men | All UTIs are complicated; full investigation needed; exclude prostatitis; minimum 7-day course; consider urological referral |
| Diabetics | Higher risk and more severe infections; emphysematous pyelonephritis risk; strict glycaemic control |
| Catheterised patients (CAUTI) | Most common hospital-acquired infection; change/remove catheter; treat only when symptomatic |
| Immunocompromised | Treat ASB; longer courses; broader-spectrum agents; atypical organisms |
| Children | Investigate after first febrile UTI (USS, MCUG, DMSA); reflux nephropathy risk; renal scarring |
- Rosen's Emergency Medicine - Chapter 85 (UTI in adults and pregnancy; drug tables; diagnostic approach)
- Campbell-Walsh-Wein Urology 3-Volume Set - Chapter 55 (Nitrofurantoin, fluoroquinolone pharmacology; antimicrobial formulary; recurrent UTI management)
- Comprehensive Clinical Nephrology 7th Ed - Chapter definitions, pathogenesis, pregnancy UTI
- Harrison's Principles of Internal Medicine 22E - Antibiotic mechanisms (nitrofurantoin, quinolones)
- Goldman-Cecil Medicine - Complicated UTI, Pseudomonas UTI management
provide defenition, types, causes, pathoPHYSIOLOGY Along with flow chart, diagnostic approach , management along with pharmacology for LITHIASIS
What This Guide Covers
1. Definition
2. Types of Stones (with distribution pie chart)
- Calcium oxalate (~60-70%) - most common; radiopaque; monohydrate (dumbbell) and dihydrate (envelope) crystal forms
- Calcium phosphate (~10-20%) - includes brushite; alkaline urine; associated with RTA and hyperparathyroidism
- Struvite (~15-20%) - infection stones; magnesium ammonium phosphate; form staghorn calculi; need urease-producing bacteria
- Uric acid (~5-10%) - radiolucent; acidic urine; dissolvable with alkalinisation
- Cystine (~2%) - autosomal recessive; hexagonal crystals; COLA amino acids
- Drug-induced - indinavir, triamterene, topiramate, acyclovir, loop diuretics
3. Causes and Risk Factors
4. Pathophysiology + Flowcharts
- Master flowchart: Predisposing factors → Supersaturation → Nucleation (homogeneous/heterogeneous) → Crystal growth → Aggregation → Randall plaque anchoring → Stone growth → Ureteral migration → Colic
- Stone-specific pathways: CaOx (enteric hyperoxaluria), Struvite (urease cascade: urea → NH₃ → alkaline urine → MgNH₄PO₄), Uric acid (acidic urine + hyperuricosuria), Cystine (genetic transporter defect)
- Key inhibitors: citrate, magnesium, pyrophosphate, Tamm-Horsfall protein, glycosaminoglycans
5. Clinical Features
- Acute renal colic: abrupt onset severe colicky flank pain with location-dependent radiation (loin → groin → testis/labia); haematuria; nausea/vomiting; patient writhes
- Other presentations: asymptomatic, recurrent UTI, chronic loin pain, AKI, urosepsis
6. Diagnostic Approach (with flowchart)
- Urinalysis: pH, crystals (hexagonal = cystine pathognomonic; coffin-lid = struvite; envelope = CaOx)
- Blood: Ca, PTH, uric acid, eGFR, FBC/CRP
- NCCT (gold standard): 98%/97% sensitivity/specificity; all stone types; low-dose CT preferred
- Radiopacity table: uric acid is radiolucent; drug stones may be invisible even on CT
- 24-hour urine collection targets table for recurrent stone formers
7. Management (with flowchart)
- Emergency: Infected obstructed kidney → immediate decompression (DJ stent or PCN) + IV antibiotics
- Conservative: Stones ≤7 mm with controlled pain; hydration, analgesia, MET, strain urine
- Surgical: ESWL (≤2 cm, non-cystine); URS + laser lithotripsy (all ureteral stones, renal ≤2 cm); PCNL (>2 cm, staghorn); open surgery (last resort)
- Chemolysis: uric acid stones dissolve with urinary alkalinisation
8. Pharmacology
- Analgesia: NSAIDs first-line (diclofenac - COX inhibition → ↓PGE₂ → ↓ureteral spasm); opioids second-line
- MET: Tamsulosin 0.4 mg OD (α₁A-blocker → relax distal ureteral smooth muscle); Nifedipine (CCB) as alternative
- Prevention: Potassium citrate (↑citrate, alkalinise); Thiazides (↑distal tubular Ca reabsorption → ↓calciuria); Allopurinol (xanthine oxidase inhibitor → ↓uric acid); Penicillamine/Tiopronin (thiol chelators for cystine); Acetohydroxamic acid (urease inhibitor for struvite); Antibiotics for struvite eradication
provide defenition, types, causes, pathology, diagnostic approach , management along with pharmacology for WATER AND ELECTROLYTE IMBALANCE
Guide Summary
Section A: Foundations
- Body fluid compartments (ICF 67%, ECF 33% - plasma + interstitial)
- Normal electrolyte distribution with ranges
- AVP/ADH, RAAS, natriuretic peptides, Starling forces
- The key principle: ECF osmolality drives transcellular water movement
Section B: Water Imbalance (Sodium Disorders)
- 3-type classification: Hypovolaemic (GI losses, Addison's, diuretics) / Euvolaemic (SIADH - most common type, drugs, hypothyroidism) / Hypervolaemic (CHF, cirrhosis, nephrotic syndrome)
- Pathophysiology: Free water excess → ↓ osmolality → water INTO brain → cerebral oedema → symptoms
- SIADH criteria + full causes (CNS, pulmonary, malignancy, drugs - SSRIs, carbamazepine, cyclophosphamide)
- Osmotic Demyelination Syndrome (ODS/CPM): Over-rapid correction >8-10 mmol/L/24h → pontine demyelination → paraparesis, locked-in syndrome
- Diagnostic flowchart: Serum osm → volume status → urine Na⁺ → urine osm
- Management by type: NS (hypovolaemic) / Fluid restriction + tolvaptan (euvolaemic/hypervolaemic) / 3% NaCl bolus (severe acute)
- Causes: Diabetes Insipidus (central vs nephrogenic), dehydration, GI losses, inadequate intake
- Pathology: Water OUT of brain → cell shrinkage → vascular tearing → SDH
- DDAVP test to distinguish Central vs Nephrogenic DI
- Free water deficit formula + correction: Max 10 mmol/L/24h
- Treatment: D5W or 0.45% NS; DDAVP for central DI; thiazides paradoxically for nephrogenic DI
Section C: Potassium Disorders
- ECG: Flat T waves → U waves (characteristic) → ST depression
- Potentiates digoxin toxicity
- Urine K⁺ differentiates renal vs extra-renal loss
- Management: Oral KCl (40-100 mmol/day); IV for severe (never bolus); correct Mg²⁺ first
- ECG: Peaked T waves (first sign) → absent P waves → wide QRS → sine wave → VF
- Three-step treatment: (1) Calcium gluconate - cardiac membrane stabilisation; (2) Insulin/glucose + salbutamol + NaHCO₃ - shift K⁺ into cells; (3) SZC/Patiromer/Kayexalate/dialysis - remove K⁺ from body