GFR OF RENAL PHYSIOLOGY WITH DETAILED EXPLANATION with flowcharts
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Loading Image
Now I have comprehensive textbook content and key images. Let me compile the full, detailed explanation.
Glomerular Filtration Rate (GFR) - Detailed Explanation
1. Definition
GFR is the volume of plasma filtered across all glomeruli per unit time. It is the sum of the Single Nephron GFRs (SNGFRs) of all functioning nephrons:
- Normal GFR: 120 mL/min per 1.73 m² body surface area (~180 L/day)
- Daily tubular reabsorption: ~178.5 L/day → urine output: ~1.5 L/day
"The total glomerular filtration rate (GFR) is the sum of the SNGFRs of functioning nephrons and the normal range is wide, typically cited at 120 mL/min per 1.73 m² surface area." - Comprehensive Clinical Nephrology, 7th Edition
2. The Starling Forces - The Driving Equation
SNGFR = Kf × Net Ultrafiltration Pressure
The full equation:
SNGFR = Kf × [(Pgc - Pbs) - (πgc - πbs)]
| Variable | Meaning | Normal Value |
|---|---|---|
| Kf | Ultrafiltration coefficient (surface area × hydraulic conductivity) | Very high vs. other capillary beds |
| Pgc | Glomerular capillary hydrostatic pressure | ~45 mm Hg |
| Pbs | Bowman's space hydrostatic pressure | ~10 mm Hg |
| πgc | Glomerular capillary oncotic pressure | ~25 mm Hg |
| πbs | Bowman's space oncotic pressure | ~0 mm Hg |
Net Ultrafiltration Pressure = (45 - 10) - (25 - 0) = 35 - 25 = ~10 mm Hg
Pressure Diagram Along Glomerular Capillary
The textbook diagram below shows how pressures change along the length of the capillary:
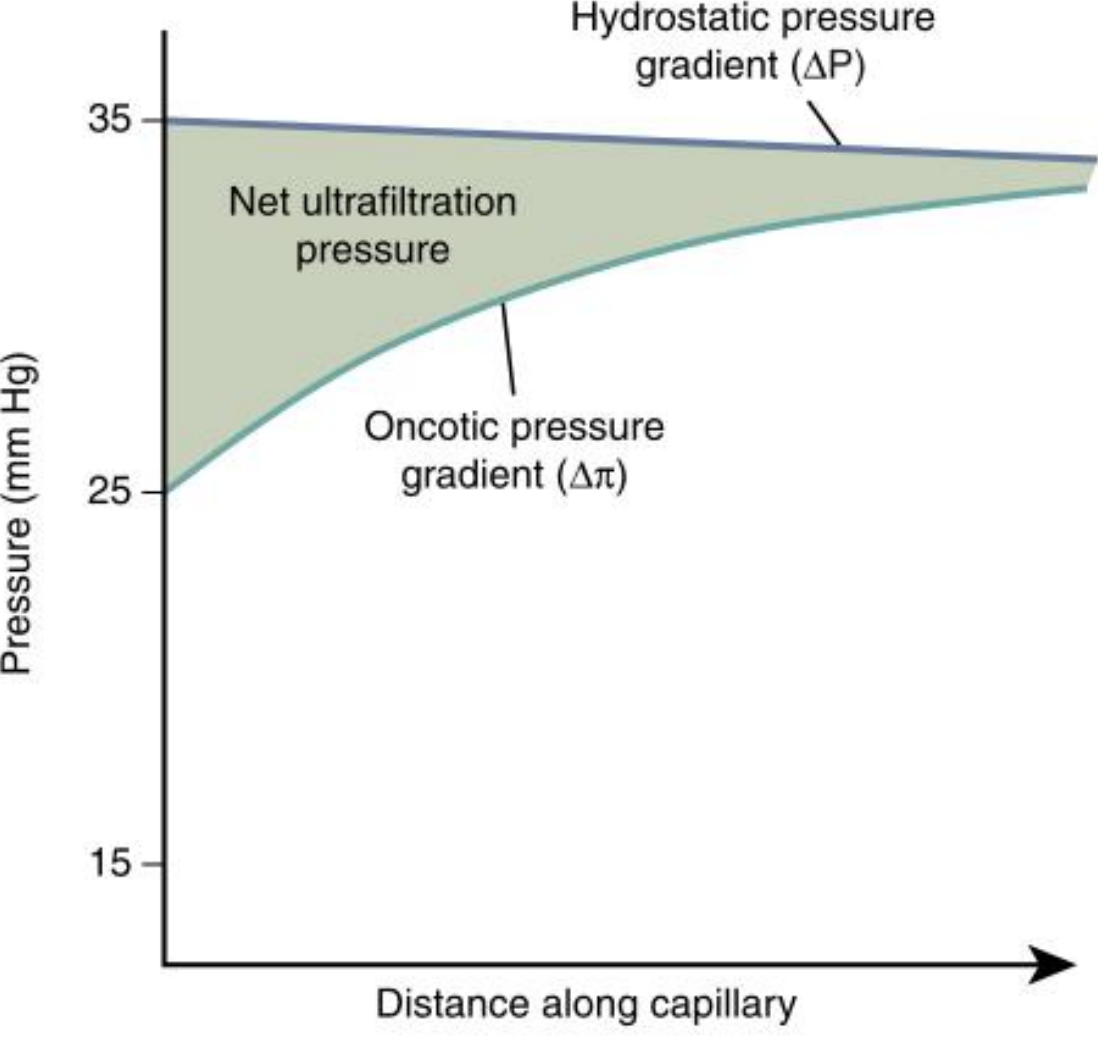
Key insight: ΔP (hydrostatic gradient) remains relatively constant because the efferent arteriole gates flow. Δπ (oncotic gradient) rises progressively as protein-free filtrate is removed, concentrating plasma proteins. Net ultrafiltration pressure falls but NEVER reaches zero under normal conditions (no filtration equilibrium in healthy glomeruli).
3. Filtration Flowchart
BLOOD enters via AFFERENT ARTERIOLE
|
▼
GLOMERULAR CAPILLARIES
|
Forces acting:
┌─────────────────────────────────────────┐
│ PRO-FILTRATION forces (push OUT): │
│ Pgc (capillary hydrostatic) = 45 mmHg │
│ πbs (Bowman's oncotic) = 0 mmHg │
│─────────────────────────────────────────│
│ ANTI-FILTRATION forces (push IN): │
│ πgc (plasma oncotic) = 25 mmHg │
│ Pbs (Bowman's hydrostatic) = 10 mmHg │
└─────────────────────────────────────────┘
|
▼
Net Ultrafiltration Pressure = ~10 mmHg
|
▼
FILTRATE enters BOWMAN'S CAPSULE
(protein-free, cell-free ultrafiltrate)
|
▼
Passes through TUBULES for reabsorption
|
▼
URINE
4. The Filtration Barrier: Size and Charge Selectivity
Three structural layers form the barrier:
| Layer | Structure | Function |
|---|---|---|
| Fenestrated endothelium | 70-100 nm pores, no diaphragm | Allows water, solutes; blocks RBCs/platelets |
| Glomerular Basement Membrane (GBM) | Type IV collagen + heparan sulfate (negative charge) | Size + charge barrier |
| Podocyte slit diaphragm | Nephrin-based filtration slits | Critical final size barrier |
Size & Charge Filterability Graph
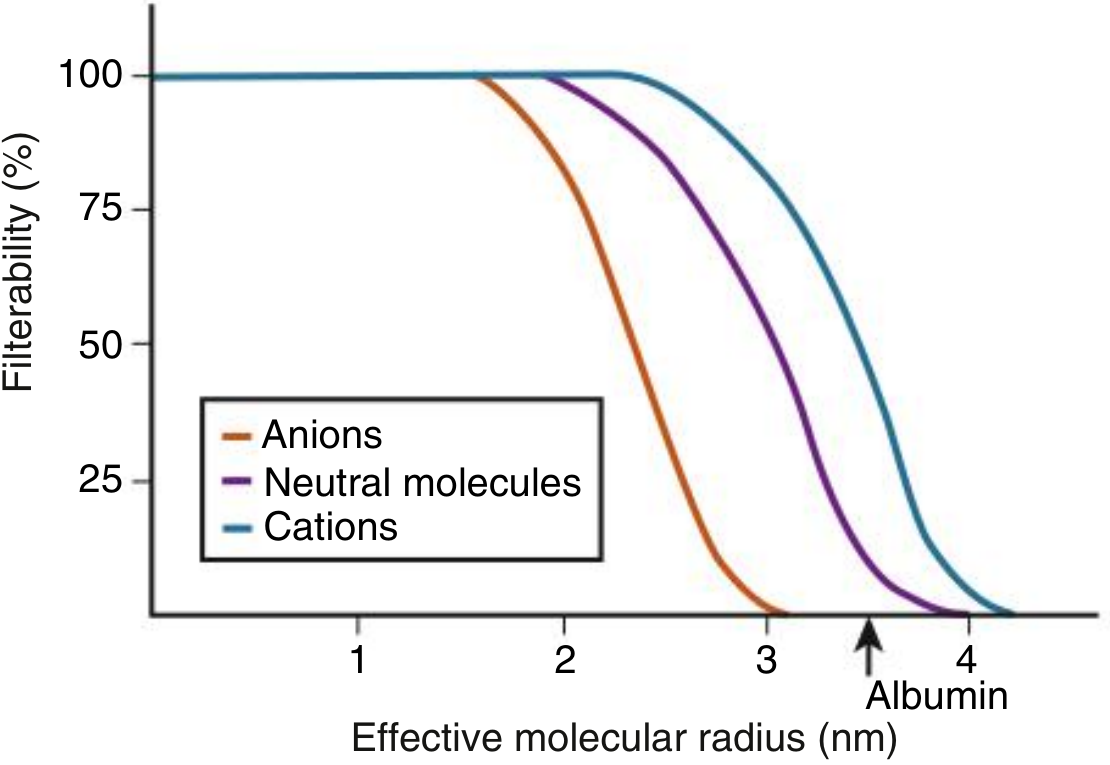
Key points:
- Molecules with radius < 1.6 nm are freely filtered regardless of charge
- Anions are filtered LESS than neutral molecules of the same size (GBM's negative charge repels them)
- Albumin (anionic, radius 3.6 nm) - almost no filtration normally
- In minimal change nephropathy, loss of GBM negative charge causes proteinuria despite preserved pore size
5. The Kf (Ultrafiltration Coefficient)
Kf = hydraulic conductivity × filtration surface area
- The mesangium (mesangial cells have contractile ability) can REDUCE filtration surface area
- Angiotensin II, vasopressin → mesangial contraction → ↓ Kf → ↓ GFR
- The glomerular capillary Kf is much higher than other capillary beds, explaining why 20% of plasma is filtered vs. <1% in systemic capillaries
6. GFR Measurement (Clearance Concept)
Renal clearance formula:
Cy = (Uy × V) / Py
Where:
- Cy = clearance of substance y (mL/min)
- Uy = urine concentration
- Py = plasma concentration
- V = urine flow rate
A substance equals GFR when it is:
- Freely filtered at the glomerulus
- NOT reabsorbed by tubules
- NOT secreted by tubules
- NOT metabolized by the kidney
| Method | Substance | Notes |
|---|---|---|
| Gold standard | Inulin (polyfructose) | Exogenous; cumbersome infusion required |
| Clinical standard | Creatinine clearance | Slightly overestimates (some tubular secretion) |
| Estimated GFR (eGFR) | CKD-EPI, MDRD equations | Uses serum creatinine, age, sex, race |
| Alternative | Cystatin C clearance | Better in low muscle mass, obesity |
7. Renal Blood Flow and Filtration Fraction
- Renal blood flow (RBF): ~1200 mL/min (~20% cardiac output)
- Renal plasma flow (RPF): ~650 mL/min
- GFR: ~120 mL/min
Filtration Fraction (FF) = GFR / RPF = 120/650 = ~20%
The 80% of plasma NOT filtered exits via the efferent arteriole into:
- Peritubular capillaries (cortical nephrons) → reabsorption of tubular fluid
- Vasa recta (juxtamedullary nephrons) → medullary blood supply
8. Autoregulation of GFR
The kidney maintains GFR nearly constant over a MAP range of 80-180 mm Hg. This is an intrinsic (autonomous) mechanism - even a denervated/transplanted kidney autoregulates normally.
Autoregulation Graph
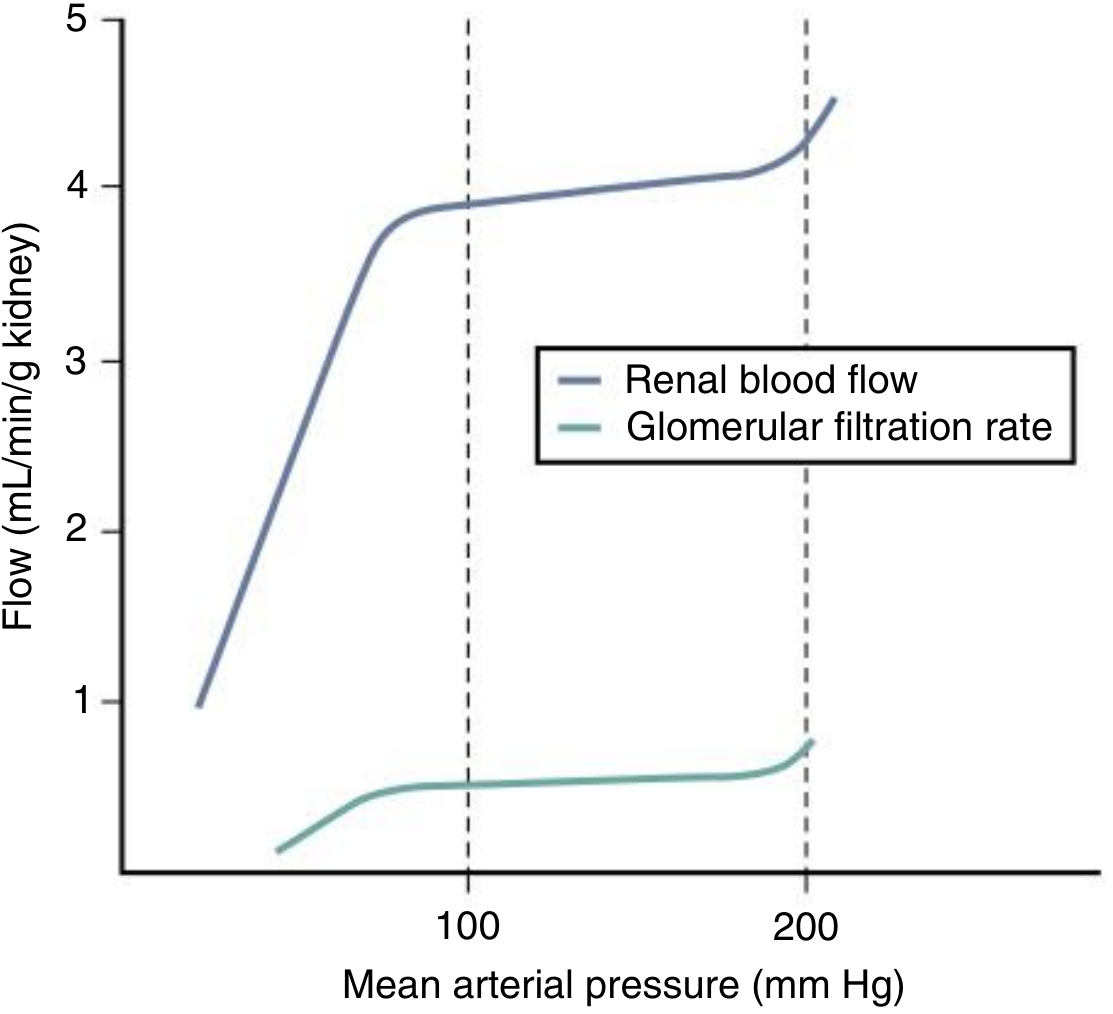
Between 80-180 mmHg MAP: RBF and GFR remain flat (autoregulated). Outside this range, they fall or rise with pressure.
Two Mechanisms of Autoregulation
A. Myogenic Mechanism (Bayliss Effect)
↑ Arterial Pressure
|
▼
Stretches afferent arteriole wall
|
▼
Opens stretch-activated Ca²⁺ channels
|
▼
↑ intracellular Ca²⁺ in smooth muscle
|
▼
Smooth muscle CONTRACTION
|
▼
↑ Afferent arteriolar resistance
|
▼
RBF and GFR restored to normal
B. Tubuloglomerular Feedback (TGF)
The most important regulatory loop, mediated by the juxtaglomerular apparatus (JGA):
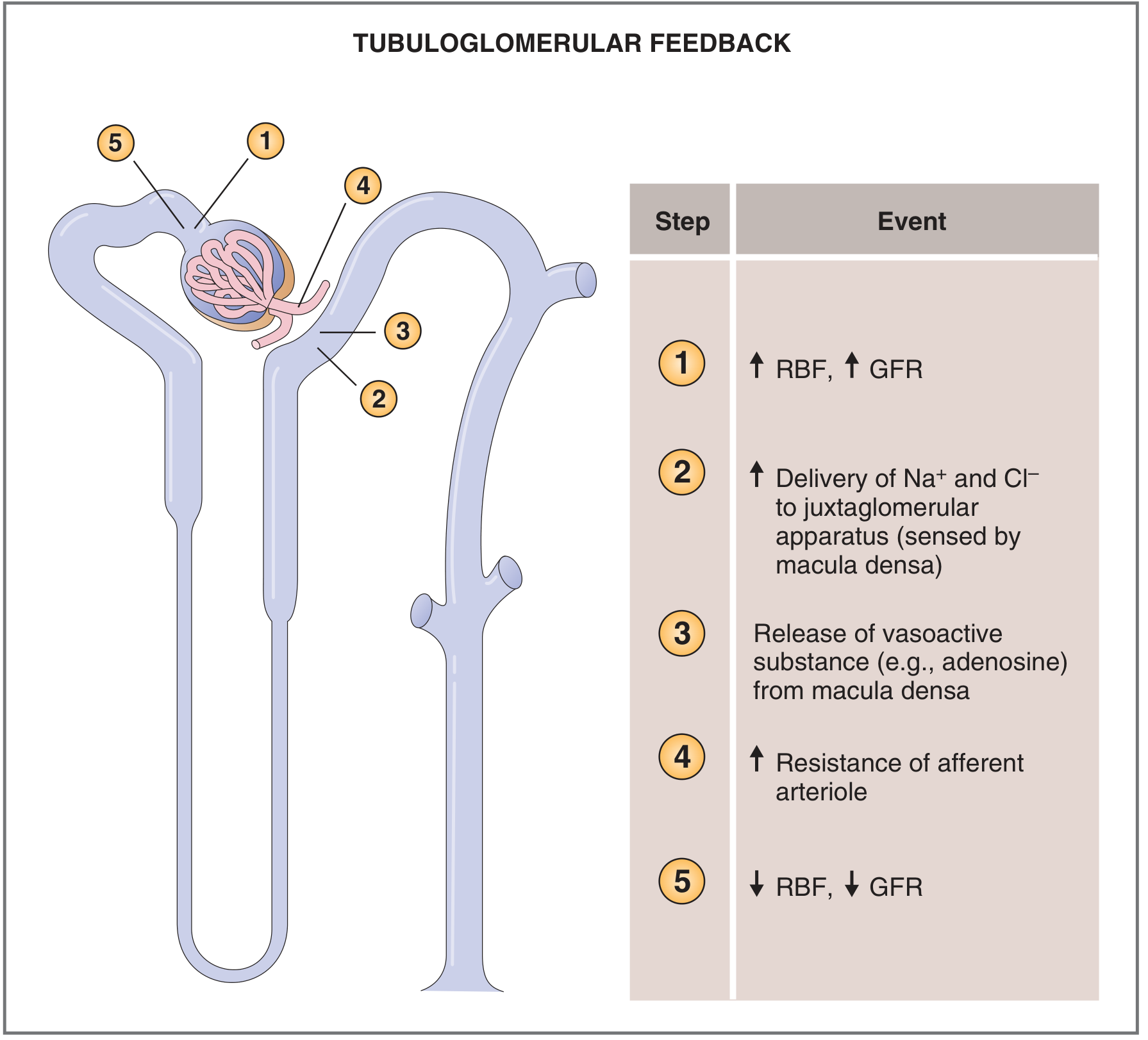
Step-by-step TGF flowchart:
Step 1: ↑ Renal arterial pressure → ↑ RBF → ↑ GFR
|
Step 2: ↑ Delivery of Na⁺ and Cl⁻ to macula densa
(specialized cells at thick ascending limb / early distal tubule)
|
Step 3: Macula densa senses ↑ NaCl via Na⁺-K⁺-2Cl⁻ cotransporter
→ triggers ATP release
→ ATP → adenosine (via ecto-5'-nucleotidase)
|
Step 4: Adenosine acts on A1 receptors on afferent arteriole
→ VASOCONSTRICTION of afferent arteriole
→ ↑ Resistance
|
Step 5: ↓ RBF → ↓ GFR → restores back to normal
Modulators of TGF sensitivity:
- Angiotensin II → sensitizes TGF (amplifies vasoconstriction)
- Nitric oxide → blunts TGF
- Adenosine → primary mediator of TGF
9. Why Autoregulation Matters (Clinical Importance)
Without autoregulation, a simple rise in MAP from 100 → 125 mmHg would increase GFR by 25%:
- GFR: 180 → 225 L/day
- Tubular reabsorption stays ~178.5 L/day
- Urine output: 1.5 → 46.5 L/day (>30× increase!)
- This would rapidly deplete plasma volume (total plasma = only 3L)
Autoregulation prevents this catastrophic fluid loss.
10. Factors That Alter GFR
Summary Flowchart
GFR = Kf × Net Ultrafiltration Pressure
INCREASES GFR: DECREASES GFR:
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
↑ Pgc ↓ Pgc
→ Afferent dilation (PGE2, NO) → Afferent constriction
→ Efferent constriction (Ang II) (catecholamines, high Ang II,
NSAIDs block PGE2)
↓ πgc ↑ πgc
→ Hypoalbuminemia, saline infusion → Hemoconcentration, ↑ protein
→ Volume depletion
↓ Pbs ↑ Pbs
→ Normal → Urinary obstruction, tubular
obstruction (casts, edema)
↑ Kf ↓ Kf
→ Relaxation of mesangium → Mesangial contraction
(ANP, cAMP-mediated) (Ang II, vasopressin, ET-1)
→ Loss of nephron mass (CKD)
Hormonal/Vasoactive Effects
| Agent | Effect on Afferent | Effect on Efferent | Net Effect on GFR |
|---|---|---|---|
| Angiotensin II (low dose) | Constricts | Constricts more | Maintained (preferential efferent) |
| Angiotensin II (high dose) | Constricts strongly | - | ↓ GFR |
| ACE inhibitors / ARBs | - | Dilates efferent | ↓ GFR (especially in renal artery stenosis) |
| Prostaglandins (PGE2, PGI2) | Dilates | - | ↑ GFR (important in low flow states) |
| NSAIDs | Block PGE2 → constrict afferent | - | ↓ GFR |
| ANP (atrial natriuretic peptide) | Dilates | Constricts | ↑ GFR |
| Sympathetic/catecholamines | Constricts | Constricts | ↓ GFR |
| Nitric oxide | Dilates | - | ↑ GFR |
| Endothelin (ET-1) | Constricts | Constricts | ↓ GFR |
11. CKD Staging by GFR
| Stage | Description | eGFR (mL/min/1.73 m²) |
|---|---|---|
| G1 | Normal or high | ≥ 90 |
| G2 | Mildly decreased | 60-89 |
| G3a | Mildly-moderately decreased | 45-59 |
| G3b | Moderately-severely decreased | 30-44 |
| G4 | Severely decreased | 15-29 |
| G5 | Kidney failure | < 15 |
12. Master Summary Flowchart
RENAL ARTERY BLOOD
|
▼
AFFERENT ARTERIOLE
(resistance controlled by myogenic reflex + TGF + neurohumoral factors)
|
▼
GLOMERULAR CAPILLARY (Pgc ~45 mmHg)
|
FILTRATION EQUATION:
GFR = Kf × [(Pgc - Pbs) - (πgc - πbs)]
↓ ↓
Net hydrostatic Net oncotic
gradient (~35 mmHg) pressure (~25 mmHg)
↓
Net Ultrafiltration = ~10 mmHg
|
▼
BOWMAN'S CAPSULE
(protein-free, cell-free filtrate)
|
▼
PROXIMAL TUBULE → LOOP OF HENLE → DISTAL TUBULE → COLLECTING DUCT
(reabsorb 178.5 L/day out of 180 L/day filtered)
|
▼
URINE (~1.5 L/day)
AUTOREGULATION LOOP:
↑ MAP → ↑ GFR → ↑ NaCl at macula densa → TGF → adenosine
→ ↑ Afferent resistance → ↓ RBF → GFR restored
(+ Myogenic: stretch → Ca²⁺ → smooth muscle contraction)
Sources
- Comprehensive Clinical Nephrology, 7th Edition, p. 35-36
- Costanzo Physiology, 7th Edition, p. 264
- Guyton and Hall Textbook of Medical Physiology, p. 343
- National Kidney Foundation Primer on Kidney Diseases, 8th Edition
This is a shared conversation. Sign in to Orris to start your own chat.