Mucoepidermoid cancer
Reading File
Finding Sources
Searching PubMed
mucoepidermoid carcinoma
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information to provide a thorough answer. Let me compile the full response.
Mucoepidermoid Carcinoma (MEC)
Overview
Mucoepidermoid carcinoma is the most common primary malignant tumor of the salivary glands, representing approximately 15% of all salivary gland tumors. It is also the most common salivary gland malignancy in children and the most common pediatric salivary gland carcinoma overall.
- Sex: Slightly more common in women
- Mean age at onset: ~45 years (but can occur in children; peak pediatric incidence in the second decade)
- Risk factor: Prior radiation or chemotherapy in childhood increases risk
- Typical presentation: Painless, slow-growing mass
Sites of Origin
| Site | Notes |
|---|---|
| Parotid gland | Most common site; 60-70% of cases |
| Submandibular gland | Higher recurrence/metastasis rate even for low-grade tumors |
| Minor salivary glands | Hard palate most common intraoral site; also buccal mucosa, lip, retromolar trigone |
| Intraosseous (mandible/maxilla) | Rare; considered odontogenic in origin; less aggressive |
| Lung (tracheobronchial) | Also a recognized primary site |
Molecular Pathogenesis
More than 50% of MECs carry a balanced t(11;19)(q21;p13) chromosomal translocation, creating the CRTC1::MAML2 fusion gene. The fused MAML2 portion cannot interact normally with Notch signaling components, and the fusion protein is believed to perturb both Notch and cAMP-dependent signaling pathways. This translocation:
- Helps confirm the diagnosis (especially in low- and intermediate-grade tumors)
- Is associated with a better prognosis
- Is typically absent in high-grade MEC
Gross Pathology
- Can grow up to 8 cm in diameter
- Appear circumscribed but lack a true capsule - often infiltrative
- Cut surface: pale, gray-white with small mucin-containing cysts
- May appear bluish (mimicking a mucocele) in the oral cavity due to mucinous cyst content
Histology - The Three Cell Types
The hallmark of MEC is the presence of three cell types in variable proportions:
| Cell Type | Features |
|---|---|
| Mucous cells | Abundant light blue mucin in cytoplasm; nuclei displaced to periphery; line cystic spaces |
| Squamoid (epidermoid) cells | Large with abundant pink cytoplasm; resemble squamous cells but are NOT truly squamous; keratinization is rare |
| Intermediate cells | Modest amounts of pink or clear cytoplasm; usually the predominant cell type |
Architecture is a mixture of cystic and solid elements (cords, sheets, nests, or duct-like structures).
Special stains: PAS, mucicarmine, or Alcian blue can highlight mucin when it is scant.
IHC: Of limited utility in diagnosis.
FNA findings: Mucous cells (vacuolated cytoplasm), intermediate cells (round, small, open chromatin), squamoid cells (dense, homogeneous cytoplasm - orange on Papanicolaou stain). Both glandular and squamoid components must be present for diagnosis.
Histology Images
(Cummings Otolaryngology, Fig. 85.3)
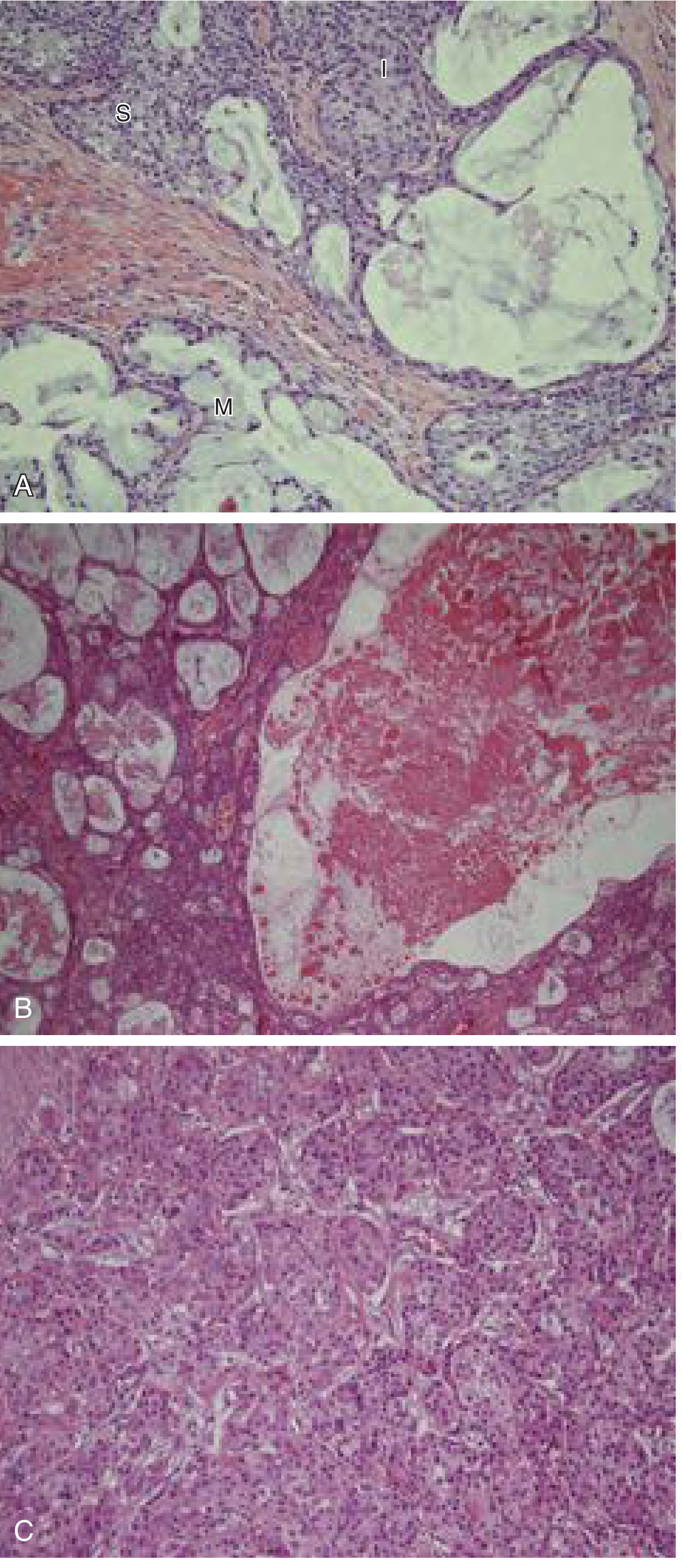
(A) Intermediate cells (I), mucous cells (M), and squamoid cells (S) - x200. (B) Tumor with extensive cystic change - x100. (C) High-grade MEC: solid sheets of intermediate cells, minimal mucous differentiation, no cystic change - x200.
(Robbins Pathology, Fig. 16.22)
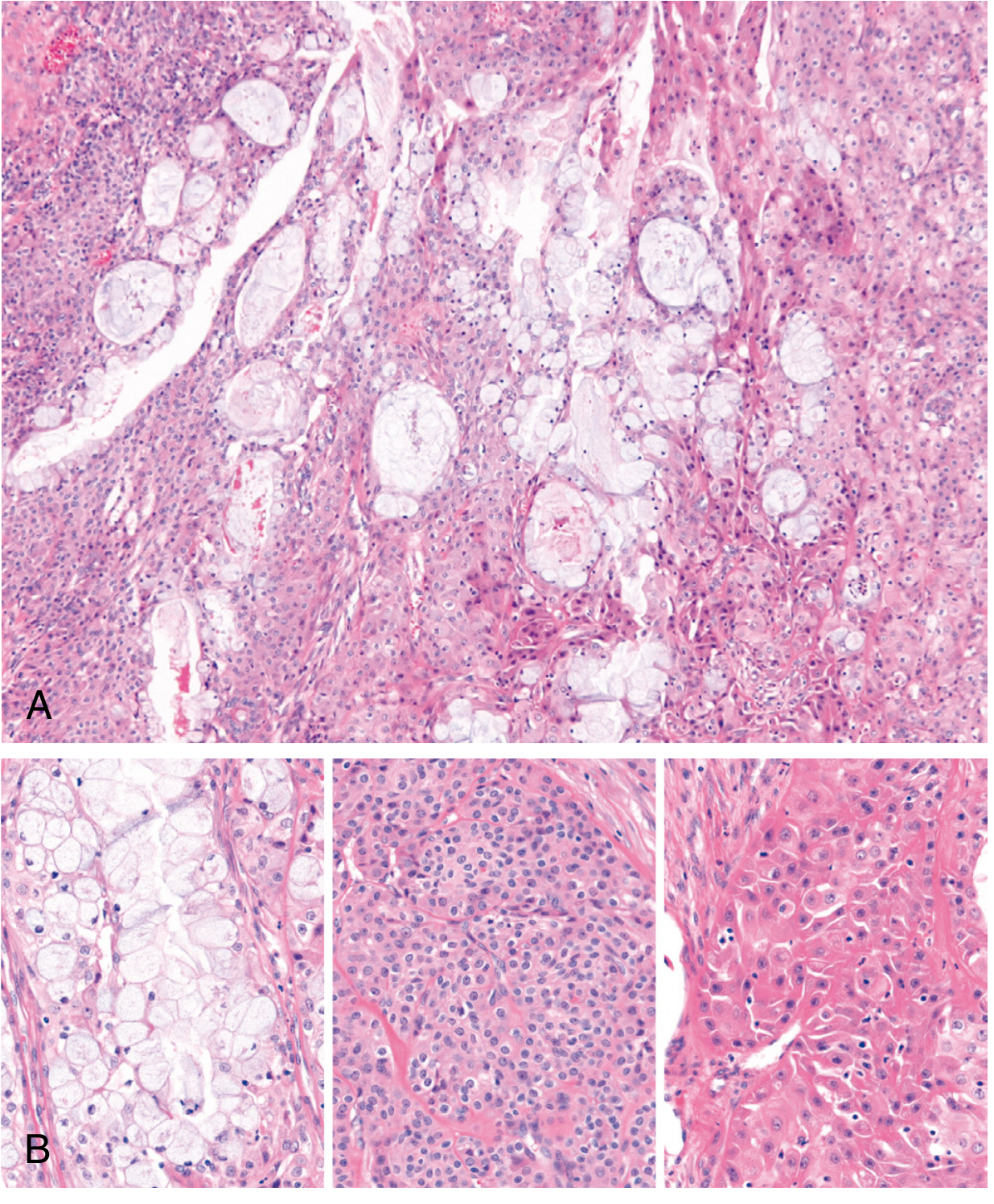
(A) Low-power: sheets and microcysts. (B) Cells vary from mucinous (left) to intermediate (center) to squamous (right).
Grading
Grading strongly correlates with clinical behavior. Two major systems are in use:
Auclair Grading System
| Parameter | Points |
|---|---|
| Cystic component <20% | +2 |
| Neural invasion | +2 |
| ≥4 mitoses/10 hpf | +3 |
| Necrosis | +3 |
| Anaplasia | +4 |
| Grade | Score |
|---|---|
| Low (Grade 1) | 0-4 |
| Intermediate (Grade 2) | 5-6 |
| High (Grade 3) | ≥7 |
Brandwein Grading System (modification - more stringent)
| Parameter | Points |
|---|---|
| Cystic component <25% | +2 |
| Tumor front invades in small nests/islands | +2 |
| Pronounced nuclear atypia | +2 |
| Lymphatic/vascular invasion | +3 |
| Neural invasion | +3 |
| Necrosis | +3 |
| ≥4 mitoses/10 hpf | +3 |
| Bony invasion | +3 |
| Grade | Score |
|---|---|
| Low (Grade 1) | 0 |
| Intermediate (Grade 2) | 2-3 |
| High (Grade 3) | ≥4 |
The Brandwein system is more stringent - tumors classified as low-grade by this system rarely ever metastasize or cause death. Intermediate-grade MEC has the most inter-observer variability and the most unpredictable clinical behavior.
Grade Correlates with Histology
| Feature | Low-Grade | High-Grade |
|---|---|---|
| Architecture | Predominantly cystic | Predominantly solid |
| Cell type | Abundant, well-differentiated mucous cells | Squamoid and intermediate cells predominate |
| Cytologic atypia | Minimal | Prominent |
| Mitoses | Low | High |
| Other | Well circumscribed | Necrosis, perineural invasion, LVI, bony invasion |
Differential Diagnosis
- Necrotizing sialometaplasia - nonneoplastic lesion of the hard palate; reactive changes in minor salivary glands
- Adenosquamous carcinoma - most important distinction, especially at mucosal sites
- High-grade, with definitive squamous differentiation and keratinization (rare in MEC)
- Often has surface mucosal squamous dysplasia (absent in MEC)
- Mucocele (clinically, due to bluish appearance in oral cavity)
Prognosis by Grade
| Grade | Local Recurrence | Distant Metastasis | 5-Year Survival |
|---|---|---|---|
| Low | ~15% | Rare | >90% |
| Intermediate | Variable | Variable | Intermediate |
| High | Up to 30% | ~30% (lungs most common) | ~50% |
Additional prognostic factors:
- Submandibular gland primaries recur and metastasize more often than parotid or minor salivary gland tumors, even when low-grade
- Presence of CRTC1::MAML2 fusion = better prognosis (but not independent of grade)
- Clinical stage is as important as histologic grade
Treatment
- Complete surgical excision with wide margins - cornerstone of treatment for all grades
- Adjuvant radiotherapy - standard of care for intermediate- and high-grade MEC
- Low-grade MEC: surgery alone generally sufficient
- High-grade MEC: aggressive local extension with bone/skin involvement and nodal metastases; thorough resection mandatory; adjuvant RT indicated
Key Summary Points
- Most common salivary gland malignancy; most common pediatric salivary gland cancer
- Parotid is the most common site
- Three cell types: mucous, squamoid (epidermoid), intermediate
- Graded as low, intermediate, or high - this drives prognosis and management
- CRTC1::MAML2 fusion from t(11;19) translocation - diagnostic and prognostic marker
- True keratinization is rare; if present, consider adenosquamous carcinoma
- High-grade: solid, aggressive, 50% 5-year survival; Low-grade: cystic, indolent, >90% survival
Sources: Cummings Otolaryngology Head & Neck Surgery, p. 1531; Bailey and Love's Short Practice of Surgery 28th ed., p. 862; Robbins & Kumar Basic Pathology / Robbins Cotran Pathologic Basis of Disease, p. 698
Recent evidence (2024-2025): Systematic reviews confirm ongoing interest in Warthin-like MEC variants (PMID 40338433) and laryngeal MEC recurrence patterns (PMID 38591104) - no major paradigm shifts from the above guidelines.
What surgery
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Excellent - comprehensive surgical information gathered. Here is the complete answer:
Surgery for Mucoepidermoid Carcinoma
The surgical approach depends on tumor location and histologic grade. Wide excision with clear margins is the cardinal principle for all sites.
1. Parotid Gland (Most Common Site)
Superficial Parotidectomy
- Adequate for small, low-grade tumors confined to the superficial lobe
- The facial nerve is dissected and preserved
- Less Frey syndrome and facial nerve morbidity compared to total parotidectomy
- Landmarks for facial nerve identification: tympanomastoid suture line, posterior belly of digastric muscle, tragal pointer, stylomastoid artery
Total Parotidectomy
- Required for larger tumors, deep lobe involvement, high-grade MEC, or any malignancy with significant extent
- Diagnosis of malignancy may not be confirmed until final pathology - en bloc resection with good margins is adequate in most small cancers
- Facial nerve management is the key surgical decision:
| Scenario | Action |
|---|---|
| Nerve not invaded, functional | Preserve nerve - always |
| Low-grade MEC near nerve | Total parotidectomy with facial nerve preservation |
| High-grade MEC, nerve grossly invaded (pathology confirmed) | Sacrifice nerve + immediate nerve graft reconstruction |
| Tumor near skull base / stylomastoid foramen | Open mastoid, identify descending facial nerve proximally, then follow toward tumor |
The facial nerve should never be sacrificed unless there is pathology-confirmed invasion. Even in malignancy, if the nerve is functional and not directly invaded, it is preserved.
Facial Nerve Reconstruction
If sacrificed, immediate reconstruction with a nerve graft (e.g., greater auricular nerve or sural nerve) is performed at the same sitting.
2. Neck Dissection
| Scenario | Recommendation |
|---|---|
| High-grade MEC | Ipsilateral elective neck dissection even with N0 neck |
| Clinically node-positive (any grade) | Therapeutic neck dissection |
| Low-grade MEC | Neck dissection generally not needed unless clinically positive |
| Oral cavity/oropharyngeal MEC, high-grade or T3-T4 | Occult nodal rate ~14-17% - neck dissection indicated |
3. Submandibular Gland
- Resection via an upper neck crease incision
- Marginal mandibular branch of the facial nerve must be carefully preserved (runs superficial to the gland)
- The hypoglossal nerve is identified medially (deep to the digastric)
- Even low-grade MEC of the submandibular gland should be resected aggressively, as it has a higher recurrence and metastasis rate than parotid-site disease
4. Minor Salivary Gland (Palate, Oral Cavity, Oropharynx)
- Wide surgical excision with clear margins
- For hard palate primaries: resection may include periosteum or bone if involved
- Neck dissection for suspected/clinically obvious nodal disease; in National Cancer Database data (3005 patients), occult nodal rate was <6% overall but rose to ~14-17% with high-grade or T3-T4 tumors
5. Laryngeal MEC
- Partial or total laryngectomy depending on tumor size and extent
- Neck dissection for node-positive disease
- Some advocate elective neck dissection for high-grade only; others for all given high regional metastasis rates
6. Parapharyngeal Space
- Transcervical approach (most cases)
- Mandibulotomy for access when mandible is involved or better exposure is needed
- Infratemporal fossa approach or mastoidectomy for skull base extension
- Transoral approach is avoided due to risk of tumor rupture
Adjuvant Radiotherapy (Post-op)
| Indication | Recommendation |
|---|---|
| Stage III/IV disease | Yes |
| High-grade MEC (any site) | Yes |
| Perineural invasion | Yes |
| Close or positive surgical margins | Yes |
| Pathologically confirmed cervical metastases | Yes |
| Low-grade, clear margins | Surgery alone generally sufficient |
Summary by Grade
| Grade | Surgery | Neck | Adjuvant RT |
|---|---|---|---|
| Low | Complete excision with margins | Only if N+ | Usually not needed |
| Intermediate | Complete excision, often total parotidectomy | Selective / N+ | Consider |
| High | Total parotidectomy / radical resection | Elective neck dissection | Yes |
Sources: Mulholland & Greenfield's Surgery 7e, p. 1985-1986; Scott-Brown's Otorhinolaryngology Vol. 1, p. 497; K.J. Lee's Essential Otolaryngology, p. 657; Cummings Otolaryngology, p. 1785, 2008
Maxillectomy surgery
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive information to compose a full, well-structured answer.
Maxillectomy Surgery
Maxillectomy is the surgical resection of part or all of the maxilla (upper jaw), performed primarily for malignant tumors of the maxillary sinus, nasal cavity, palate, and adjacent structures. The extent of resection is dictated by tumor location, size, and involvement of surrounding structures.
Classification of Maxillectomy
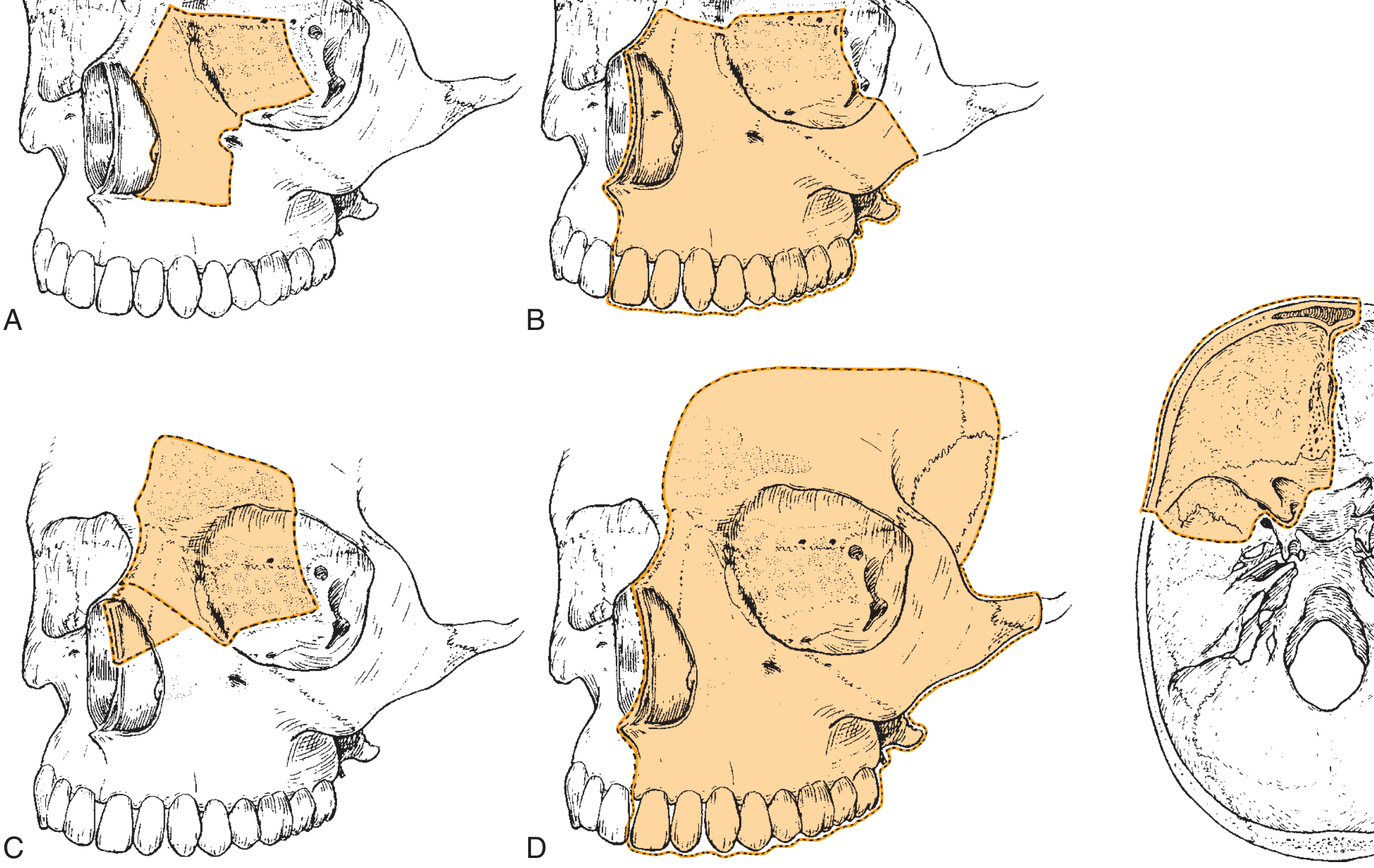
(Fig. A = Medial maxillectomy; B = Total maxillectomy; C & D = Craniofacial resection with varying extent)
1. Partial (Infrastructure) Maxillectomy
Partial removal of the upper jaw skeleton. Two common variants:
- Medial maxillectomy - clearance of the lateral nasal wall including the ethmoid sinuses
- Palatal/alveolar resection - hard palate with adjacent alveolus; used for oral cavity tumors
Infrastructural maxillectomy builds on the medial maxillectomy by also removing the dentition, alveolar ridge, and hard palate.
2. Subtotal Maxillectomy
Removes the entire maxilla but preserves the orbital floor.
3. Total Maxillectomy
Removes the entire maxilla including the orbital floor (but preserves the orbital contents if the periorbita is not breached).
4. Extended Maxillectomy
Required when tumor extends beyond the maxilla - to skin, infratemporal fossa, pterygoid plates, or skull base. When the skull base is involved, this becomes a craniofacial resection.
5. Total Maxillectomy with Orbital Exenteration
When tumor invades through the orbital periosteum into the periorbita - orbital exenteration is added. Only performed with curative intent.
Surgical Approaches (Incisions)
Three classic soft tissue exposures are used:
A. Lateral Rhinotomy (Moure / originally Michaux, 1854)
- Incision along the lateral nasal crease
- Excellent exposure of nasal cavities and medial maxilla
- Cosmetically acceptable scar in nasal crease
- Can be extended into the lip if needed (usually unnecessary)
- Used for medial maxillectomy
B. Weber-Ferguson Incision (originally Gensoul, 1833)
- The standard approach for total maxillectomy
- Facial incision from medial canthus along the nasal side, splitting the upper lip at the philtrum
- A subciliary extension (under the lower eyelid) is added when the orbital floor must be accessed
- The incision should follow the lid crease closely to maintain cosmesis; any lateral extension runs inferolaterally into a "crow's foot"
- In the medial canthal region, curve the incision forward over the nasal bones for support
- A stepped incision on the lip (along the philtrum crest) is more acceptable than a midline cut
- Upper cheek flap raised in a submuscular (subperiosteal) plane
C. Midfacial Degloving (Casson / Howard)
- No external skin incision - completely hidden scars
- Sublabial incision from maxillary tuberosity to contralateral tuberosity + bilateral intercartilaginous incisions + transfixion incision
- Midface soft tissues elevated over the nasal dorsum (rhinoplasty technique)
- With infraorbital nerve division: exposes entire anterior maxilla to the inferior orbital rim
- Can be combined with Le Fort I osteotomy for access to the clivus
- Suitable for bilateral or centrally placed lesions; not ideal if anterior ethmoids, frontonasal duct, orbit, or zygoma are involved
Anaesthesia note: Hypotensive general anaesthesia + topical nasal decongestant. An oral tube or tracheostomy is required for midfacial degloving.
Step-by-Step: Total (Subtotal) Maxillectomy
Skin Incision and Flap
- Weber-Ferguson incision with subciliary extension
- Upper cheek flap raised; lower eyelid portion elevated off the orbicularis oculi
- Flap taken laterally to ~1 cm beyond the lateral canthus
- Orbicularis oculi and orbit dissected off the inferior orbital rim in subperiosteal fashion, carried back toward the orbital apex
- Masseter muscle attachment to the inferior zygoma is divided
Intraoral Mucosal Incision
- Mucosal incision between the lateral incisor and canine, carried posteriorly along the midline of the hard palate
- At the junction of soft palate, the incision turns laterally to the maxillary tubercle and along the gingivobuccal sulcus behind the last molar
- Medial pterygoid muscle attachments are cut to further free the maxilla
Osteotomies
The maxilla must be freed from all bony attachments:
| Osteotomy | Location |
|---|---|
| Premaxilla | Through premaxilla into nasal cavity |
| Superomedial | Through the nasal process and medial orbital rim (preserving orbital floor in subtotal) |
| Superolateral | Through the zygomatic arch - if zygoma included, osteotomy through lateral orbital wall below Whitnall's tubercle |
| Lateral maxillary wall | Divided after zygomatic arch |
| Pterygoid plates | Freed using a curved osteotome (not power saw) |
| Palatal | In the floor of the nasal cavity, using power tools; placed in the midline |
| Frontal process | Osteotomy through frontal process of maxilla, dividing the lacrimal sac |
- Power saws are used expeditiously to minimize blood loss
- An osteotome completes the fracture lines
- Remaining soft tissue attachments at the posterior maxilla are divided with heavy Mayo scissors
- Specimen is removed en bloc
Bleeding Control
- Internal maxillary artery - controlled by packing, Ligaclip, diathermy, or haemostatic matrices (often in combination)
Completion of Resection
After the maxilla is removed:
- Ethmoid cells are exenterated completely
- Sphenoid and frontal sinuses opened widely
- Assessment for orbital periosteum involvement
Orbital Management
| Situation | Management |
|---|---|
| Orbital floor invaded but periorbita intact | Remove orbital floor; preserve orbital contents |
| Medial/inferior orbital walls removed | Globe can survive without enophthalmos |
| Whitnall's tubercle removed (lateral orbital wall) | Loss of lateral globe support → correct by temporalis muscle transposition medially |
| Orbital periosteum (periorbita) breached | Orbital exenteration indicated |
Orbital Exenteration Technique (when added)
- Skin incisions from medial to lateral canthi; skin flaps raised off orbicularis oculi
- Superior orbital periosteum incised → subperiosteal dissection on orbital roof back to apex, done circumferentially (except the quadrant in continuity with the maxillectomy specimen)
- Extraocular muscles divided
- Optic nerve and vessels clamped and suture ligated
- Eyelids preserved; lid margins and tarsal plates sacrificed → smooth skin-lined cavity for an onlay prosthesis
Neck Dissection
- Occult metastasis rate in maxillary sinus SCC is < 10%
- Retrospective reviews do not clearly show survival benefit from elective selective neck dissection
- Neck dissection is performed for clinically node-positive disease
Endoscopic Partial/Medial Maxillectomy
A minimally invasive alternative for selected tumors:
Anatomic segments resected endoscopically:
- Medial maxillary wall with inferior turbinate attachment
- Uncinate process
- Orbital lamina (if involved)
- Posterior margins can extend to the nasopharynx
- Lateral limit: plane of the maxillary division of trigeminal nerve (V2) in the orbital floor
Denker's Extension - adds removal of the lateral nasal piriform aperture for anterior maxillary sinus access (periosteum of anterior face elevated to infraorbital nerve).
Potential complications of endoscopic maxillectomy:
- Epiphora (nasolacrimal duct injury)
- Orbital complications (diplopia, orbital hematoma, vision loss)
- Bleeding
- V2 nerve damage
- CSF leak
- Olfactory loss
- Sinonasal/vestibular scarring
Reconstruction
Choice depends on defect size and whether the orbit is involved:
| Defect | Reconstruction |
|---|---|
| Low defects (no orbital involvement) | Dental obturator ± split-skin graft lining |
| Extensive maxillary defects | Free flap required |
| Bony orbital floor support needed | DCIA flap (iliac crest + internal oblique) or scapula tip flap (with latissimus dorsi) - enables implant-borne dental/orbital prosthesis |
| Soft tissue only | Free rectus abdominis flap |
| Nasomaxillary defect | Bone needed to augment nasal bone loss |
| Orbitomaxillary defect | Can use local or soft-tissue free flap |
| Total maxillectomy + orbital exenteration | Scapula flap or DCIA flap (composite bone + soft tissue for best cosmesis and function) |
Obturator Technique (when used)
- Split-skin graft applied to under surface of facial skin flap
- Temporary prosthesis fitted immediately after closure (secured with circumzygomatic wires or fixation screws into hard palate remnant)
- Prosthesis changed at ~14 days; adjusted repeatedly over weeks until cavity healed
- Definitive dental obturator created once healing is complete; must obliterate air space and can restore voice via bolus extension
Postoperative jaw exercises are essential for months to prevent trismus.
Craniofacial Resection (Extended Maxillectomy)
For tumors involving the cribriform plate or skull base, a combined intracranial and transfacial approach is used (Ketcham/Cheesman classification):
| Type | Description |
|---|---|
| Type 1 (transorbital) | Extended medial maxillectomy via lateral rhinotomy - controls cribriform plate via orbital approach |
| Type 2 | Full transcranial + transfacial; bifrontal craniotomy combined with facial approach |
| Type 3 | Most extensive; includes lateral skull base / infratemporal fossa |
5-year survival after craniofacial resection is significantly affected by: margin status, histology (adenocarcinoma > SCC), and intracranial invasion.
Summary Table
| Procedure | Extent | Approach | Reconstruction |
|---|---|---|---|
| Medial maxillectomy | Lateral nasal wall + ethmoids | Lateral rhinotomy or endoscopic | Healing by secondary intention / local flap |
| Partial/infrastructure maxillectomy | Palate + alveolus | Intraoral / lateral rhinotomy | Obturator or free flap |
| Subtotal maxillectomy | Entire maxilla, orbital floor spared | Weber-Ferguson + subciliary | Obturator or free flap |
| Total maxillectomy | Entire maxilla + orbital floor | Weber-Ferguson + subciliary | Free flap (DCIA / scapula / rectus) |
| Total maxillectomy + orbital exenteration | Above + orbital contents | Weber-Ferguson | Composite free flap (scapula/DCIA) |
| Craniofacial resection | Maxilla + skull base | Weber-Ferguson + bifrontal craniotomy | Composite flap ± dural repair |
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, pp. 127-130; Cummings Otolaryngology Head & Neck Surgery, pp. 1747-1757
This is a shared conversation. Sign in to Orris to start your own chat.