Can stomach carcinoma present with ulcers mainly lintis plastica
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Here is a comprehensive answer based on authoritative pathology and gastroenterology textbooks.
Stomach Carcinoma: Ulcers vs. Linitis Plastica
The short answer is: ulcers and linitis plastica are distinct morphological presentations of gastric carcinoma, not the same thing. However, they can co-exist in some forms. Here is the full picture:
Macroscopic (Gross) Presentations — Borrmann Classification
Advanced gastric cancers are classified by the Borrmann system into four types:
| Type | Description |
|---|---|
| I | Polypoid / fungating mass |
| II | Ulcerative with elevated, distinct borders |
| III | Ulcerative with indistinct borders (infiltrative) |
| IV | Diffuse infiltrative — also called linitis plastica |
Types I & II are localized; Types III & IV are infiltrative. — Yamada's Textbook of Gastroenterology, 7th ed.
Linitis Plastica (Borrmann Type IV)
- Linitis plastica is the diffuse infiltrative form of gastric cancer, predominantly caused by signet ring cell (poorly cohesive) adenocarcinoma.
- Tumor cells permeate the entire gastric wall as small clusters and individual discohesive cells, driven by loss of E-cadherin (CDH1 mutations).
- The infiltrating cells evoke a desmoplastic (fibrotic) reaction, stiffening the gastric wall.
- When large areas are involved, this produces diffuse rugal flattening and a rigid, thickened wall — the classic "leather bottle" (linitis plastica) appearance.
- There is no discrete ulcer or mass in pure linitis plastica — the stomach is diffusely contracted and non-distensible.
"A mass may be difficult to appreciate in diffuse gastric cancer, but the infiltrative tumors often evoke a desmoplastic reaction that stiffens the gastric wall. When there are large areas of infiltration, diffuse rugal flattening and a rigid, thickened wall may impart a leather bottle appearance termed linitis plastica." — Robbins & Cotran Pathologic Basis of Disease
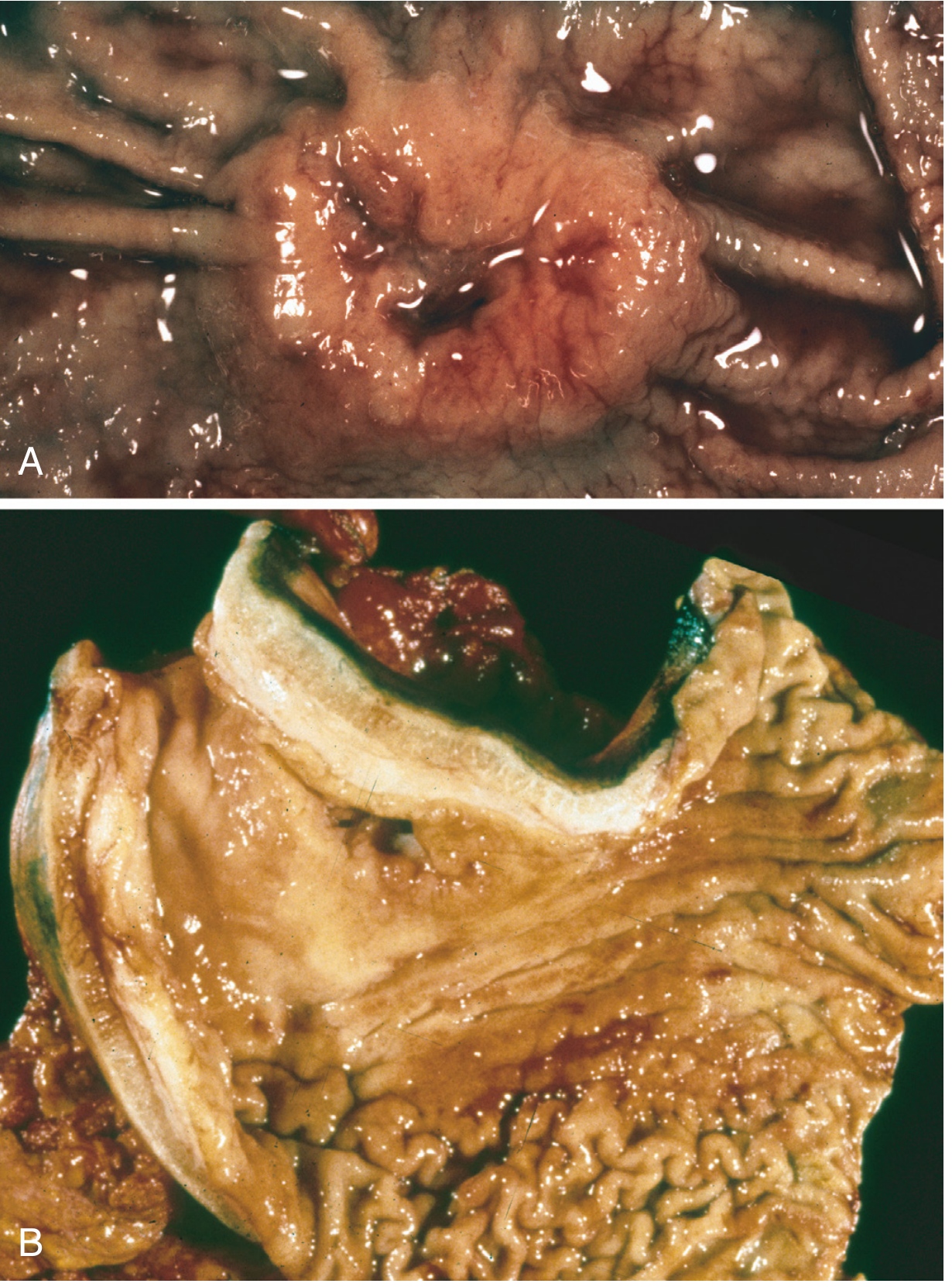
Fig. 17.20 — (A) Intestinal-type adenocarcinoma with central ulceration. (B) Linitis plastica with markedly thickened, rigid gastric wall and flattened rugae. — Robbins & Cotran
Ulcerative Presentations (Borrmann Types II & III)
- Ulcers occur mainly in intestinal-type adenocarcinoma (Laurén classification), which grows along broad cohesive fronts to form exophytic masses or ulcerated infiltrative tumors.
- The ulcers have heaped-up, irregular borders (unlike benign peptic ulcers with smooth, punched-out edges).
- Borrmann Type II = ulcerated with clear, elevated margins.
- Borrmann Type III = ulcerated with indistinct, infiltrating margins — this is the overlap zone where ulceration and infiltration co-exist.
Key Distinction
| Feature | Ulcerative (Type II/III) | Linitis Plastica (Type IV) |
|---|---|---|
| Histology | Intestinal-type adenocarcinoma | Diffuse (signet ring) type |
| Gross appearance | Ulcer with raised borders | Rigid, thickened wall, no distinct ulcer |
| Wall behavior | Focal infiltration | Diffuse wall involvement |
| E-cadherin | Usually intact | Lost (CDH1 mutation) |
| Distensibility | Preserved regionally | Severely impaired globally |
| Prognosis | Slightly better | Very poor |
Can They Co-exist?
Borrmann Type III represents a partial overlap — it has both ulceration and indistinct infiltrating borders. However, true linitis plastica (Type IV) does not primarily present as an ulcer — it presents as a diffusely contracted, non-distensible stomach. The primary presentation of linitis plastica is early satiety, weight loss, and a non-distensible stomach on endoscopy or imaging, not ulcer-type pain.
Summary: Ulcerative and linitis plastica forms are distinct morphological subtypes of gastric carcinoma. Ulcers are the hallmark of intestinal-type (Borrmann II/III), whereas linitis plastica is the hallmark of diffuse-type signet ring cell carcinoma (Borrmann IV). The main presentations of stomach carcinoma are polypoid/fungating, ulcerative, and diffusely infiltrative (linitis plastica) — not "ulcers mainly" with linitis plastica being secondary.
This is a shared conversation. Sign in to Orris to start your own chat.