Teratogenic effects of heparin in imges
Reading File
Finding Sources
Searching Images
heparin teratogenic effects fetus pregnancy
Searching the Web
heparin teratogenic effects pregnancy fetus images
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Searching Images
warfarin embryopathy nasal hypoplasia skeletal fetus comparison heparin safe pregnancy
Searching Images
heparin large molecule does not cross placenta anticoagulant pregnancy diagram
Loading Image
Loading Image
I now have all the material needed. Here is a comprehensive, image-rich answer:
Teratogenic Effects of Heparin in Pregnancy
Key Conclusion: Heparin Is NOT Teratogenic
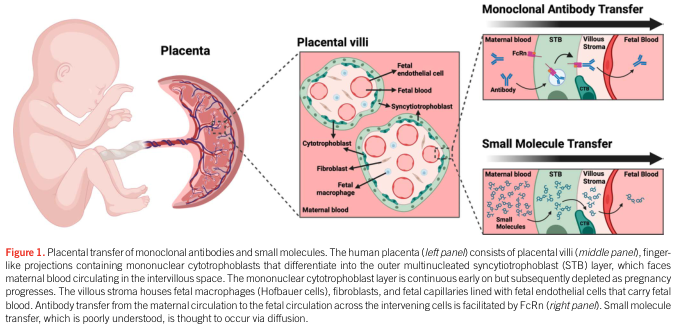
This is the central clinical point. Heparin does not cross the placenta — and therefore poses no direct teratogenic risk to the fetus. This makes it the anticoagulant of choice in pregnancy, in stark contrast to warfarin.
"The anticoagulant heparin does not appear to be teratogenic." — Langman's Medical Embryology
"Neither unfractionated heparin (UFH) nor low-molecular-weight heparin (LMWH) crosses the placenta and are not teratogenic." — Rosen's Emergency Medicine
Why Heparin Cannot Cross the Placenta
The mechanism is pharmacokinetic — heparin's molecular characteristics prevent placental transfer:
| Property | Heparin | Warfarin |
|---|---|---|
| Molecular weight | Very large (>20,000 Da) | Small (~308 Da) |
| Polarity | Highly polar (anionic) | Lipophilic |
| Placental crossing | No | Yes |
| Teratogenicity | None | Yes (1st trimester) |
| FDA Pregnancy Category | B (LMWH) / C (UFH) | X (contraindicated) |
From Katzung's Basic and Clinical Pharmacology:
"Because it is a very large (and polar) molecule, heparin is unable to cross the placenta — and this is true also for low molecular weight but polar heparins."
What IS Teratogenic: Warfarin Embryopathy (for Comparison)
Warfarin — the alternative oral anticoagulant — does cross the placenta and causes well-documented fetal harm. Understanding warfarin embryopathy highlights why heparin is the preferred substitute.
Warfarin Embryopathy: Clinical Features
1st trimester exposure (organogenesis):
- Nasal hypoplasia (flattened nasal bridge, perialar flatness)
- Skeletal abnormalities: stippled epiphyses, limb hypoplasia
- Chondrodysplasia punctata
Any trimester exposure (CNS):
- Microcephaly, optic atrophy
- Dorsal midline dysplasia, Dandy-Walker malformation
- Fetal and neonatal hemorrhage
Clinical photograph — warfarin embryopathy at ~18 weeks showing characteristic nasal hypoplasia and flattened midface:

Frontal view of warfarin-exposed fetus showing the characteristic flattened nasal bridge and overall facial dysmorphia:

Heparin in Pregnancy: Indications and Safety Profile
Although heparin is not teratogenic, it is not without maternal risks:
| Complication | Details |
|---|---|
| Maternal hemorrhage | Main concern; affects mother, not fetus |
| Heparin-induced thrombocytopenia (HIT) | Can occur; especially with UFH |
| Osteoporosis | Prolonged UFH use (>1 month); LMWH lower risk |
| Spontaneous abortion | Slightly increased, likely related to underlying thrombophilia |
| Fetal teratogenicity | None — does not cross placenta |
Common indications for heparin in pregnancy:
- Deep vein thrombosis (DVT) / Pulmonary embolism (PE)
- Mechanical heart valves (anticoagulation required throughout pregnancy)
- Antiphospholipid syndrome (with prior pregnancy morbidity)
- Prevention of thrombosis in thrombophilias
Summary
| Drug | Teratogenic? | Crosses Placenta? | Use in Pregnancy |
|---|---|---|---|
| UFH (Unfractionated Heparin) | No | No | Yes (Category C) |
| LMWH (e.g., Enoxaparin) | No | No | Yes (Category B) — preferred |
| Warfarin | Yes | Yes | Avoid (esp. 1st trimester) |
| DOACs (rivaroxaban, etc.) | Unknown | Yes | Contraindicated |
LMWH is the anticoagulant of choice in pregnancy — it is non-teratogenic, predictable in dosing, and carries lower risk of HIT and osteoporosis compared to UFH.
Sources: Langman's Medical Embryology; Katzung's Basic and Clinical Pharmacology, 16e; Creasy & Resnik's Maternal-Fetal Medicine; Rosen's Emergency Medicine; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22e
Warfarin Toxicity Features image
Reading File
Finding Sources
Searching Images
warfarin toxicity bleeding complications skin necrosis features
Searching the Web
warfarin toxicity clinical features skin necrosis purple toe syndrome hemorrhage images
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Loading Image
Loading Image
Searching Images
warfarin intracranial hemorrhage brain CT scan anticoagulant toxicity
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have everything needed. Here is the complete, image-rich answer:
Warfarin Toxicity — Features with Images
Mechanism of Warfarin Action (Context)
Warfarin inhibits vitamin K epoxide reductase (VKORC1), preventing recycling of vitamin K and blocking carboxylation of clotting factors II, VII, IX, X (and anticoagulant proteins C and S). Toxicity arises primarily from excessive anticoagulation (elevated INR) but also from paradoxical thrombotic/embolic events.
1. BLEEDING — The Major Toxicity
The most common and clinically significant adverse effect.
"The risk of intracranial hemorrhage increases dramatically with an INR greater than 4, although up to two-thirds of intracranial bleeds on warfarin occur when the INR is therapeutic." — Goodman & Gilman's Pharmacological Basis of Therapeutics
Sites of Bleeding
| Site | Features |
|---|---|
| Intracranial | Most feared; ICH, subdural hematoma, blood-fluid levels on CT |
| GI tract | Haematemesis, melaena, rectal bleeding |
| Urinary | Haematuria |
| Soft tissue | Large haematomas, ecchymoses |
| Retroperitoneal | Flank/back pain, drop in Hb |
| Surgical wounds | Excessive intraoperative/postoperative bleeding |
CT Brain — Warfarin-Related Intracranial Hemorrhage
Left parietal lobar ICH with blood-fluid level — the characteristic "hematocrit effect" seen in coagulopathy (dense cellular elements settle dependently; hypodense plasma above):

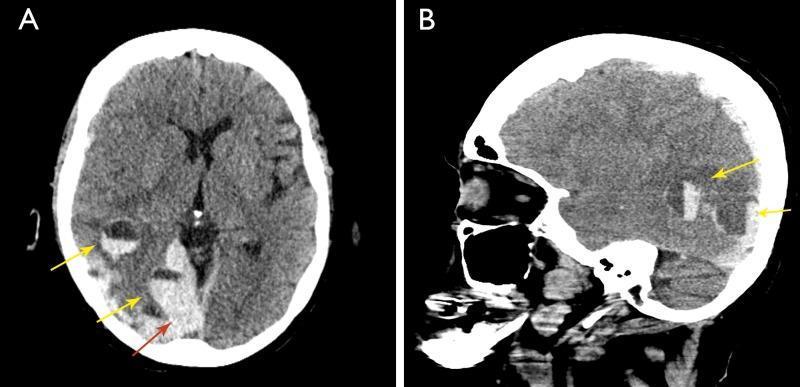
Acute subdural hematoma + intraparenchymal hematomas with blood-fluid levels — axial (A) and sagittal (B) CT showing warfarin-associated intracranial hemorrhage with midline shift:
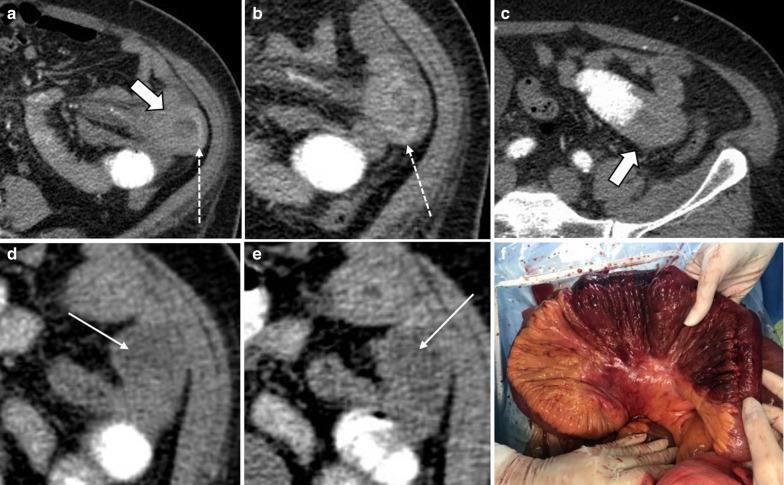
CT Abdomen — Warfarin-Related Bowel Hemorrhage
Small bowel intramural hemorrhage with circumferential mural thickening (CT a–e) and intraoperative hemorrhagic infarction of jejunum (f) in warfarin toxicity:
2. WARFARIN-INDUCED SKIN NECROSIS
A rare but serious complication occurring 3–10 days after initiation of warfarin.
Pathophysiology: Warfarin initially suppresses protein C (a natural anticoagulant) faster than the procoagulant factors, creating a transient hypercoagulable state → microvascular thrombosis → dermal ischemia and necrosis.
Risk factors: Protein C or S deficiency, HIT, large loading doses without heparin bridging.
Sites: Extremities, buttocks, breasts, thighs, abdomen, penis.
Early stage — erythematous, violaceous/dusky plaques with surrounding edema:

Established necrosis — full-thickness skin necrosis with hemorrhagic bullae and crusting:

Advanced necrosis with eschar — central grey-black eschar with surrounding violaceous edema and ulceration:

3. PURPLE TOE SYNDROME
Occurs 3–8 weeks after starting warfarin. A non-hemorrhagic complication caused by cholesterol microemboli released from atheromatous plaques. Warfarin is thought to dislodge cholesterol crystals from plaques.
Features:
- Painful, blue/purple discoloration of plantar surfaces and sides of toes
- Blanches with pressure
- Fades with leg elevation
- Bilateral involvement

4. TERATOGENICITY (Fetal Toxicity)
Covered in detail in the previous session. Key points:
- 1st trimester: Nasal hypoplasia, stippled epiphyses, limb hypoplasia (warfarin embryopathy)
- 2nd/3rd trimester: CNS defects, optic atrophy, fetal/neonatal hemorrhage, intrauterine death
- Management: Replace with heparin/LMWH throughout pregnancy
5. OTHER LESS COMMON TOXICITIES
| Toxicity | Features |
|---|---|
| Calciphylaxis | Calcium deposition in small vessels → painful skin necrosis; potentially fatal |
| Alopecia | Hair thinning/loss, usually reversible |
| Urticaria / Dermatitis | Hypersensitivity skin reactions |
| GI symptoms | Nausea, diarrhea, abdominal cramps, anorexia |
| Fever | Rare drug hypersensitivity |
| Drug interactions | Numerous — NSAIDs, antibiotics, antifungals, amiodarone all potentiate warfarin |
Management of Warfarin Toxicity / Overdose
| INR / Clinical Status | Management |
|---|---|
| INR above range, no bleeding | Hold warfarin; restart at lower dose when INR therapeutic |
| INR ≥ 10, no bleeding | Oral vitamin K₁ 2.5–5 mg; INR falls in 24–48 h |
| Serious bleeding / profound overdose | 4-factor prothrombin complex concentrate (4F-PCC) + IV vitamin K₁ 10 mg (slow infusion) |
| Post-reversal if anticoagulation still needed | Switch to heparin / LMWH |
Note: IV vitamin K₁ carries a risk of anaphylactoid reactions. High doses render patients resistant to further warfarin for several days.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics, 13e; Harrison's Principles of Internal Medicine 22e; Rosen's Emergency Medicine; DermNet NZ (warfarin-induced skin necrosis); ClotConnect (purple toe syndrome)
This is a shared conversation. Sign in to Orris to start your own chat.