give an essay answer on optical coherence tomography in ent especially larynx , its principle, mechanism, uses, indications contraindications advantages and disadvantages
optical coherence tomography larynx ENT clinical applications indications 2024
"optical coherence tomography" AND larynx
https://pmc.ncbi.nlm.nih.gov/articles/PMC3337210
"optical coherence tomography" AND ("vocal fold" OR "glottis" OR "laryngeal cancer")
OCT optical coherence tomography principle mechanism low coherence interferometry vocal cord basement membrane imaging
Optical Coherence Tomography in ENT - With Special Reference to the Larynx
1. Introduction
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 584
- Cummings Otolaryngology Head and Neck Surgery, p. 2287
2. Physical Principle
- Wavelength: 800-1300 nm NIR light (shorter wavelengths give better resolution; longer wavelengths penetrate deeper into scattering tissue)
- Axial resolution: Determined by the coherence length of the light source - typically 1-15 µm in tissue
- Lateral resolution: Determined by the focal spot size of the beam optics
- Depth of penetration: 1-3 mm, limited by optical scattering within biological tissue (most turbid tissues allow only ~1-2 mm in practice)
3. Mechanism of Image Formation
3.1 The Michelson Interferometer Setup
- Sample arm: Light is directed into the tissue via a probe or endoscopic catheter. At each depth within the tissue, small amounts of light are backscattered due to variation in optical refractive index between tissue components (cell membranes, organelles, collagen fibres, basement membrane, vessels).
- Reference arm: Light travels to a mirror at a precisely known distance and returns to the beam-splitter.
3.2 From A-Scan to 2D Image
- A-scan: One axial reflectivity profile at a single lateral point
- B-scan: Multiple A-scans acquired as the beam is swept laterally, producing a 2D cross-sectional image (equivalent to a vertical histological section)
- C-scan / en face: Lateral scanning at a fixed depth, producing a face-on image like a confocal microscopy view
3.3 Time-Domain vs Fourier-Domain OCT
| Feature | Time-Domain OCT (TD-OCT) | Fourier-Domain OCT (FD-OCT) |
|---|---|---|
| Reference mirror | Mechanically scanned | Fixed |
| Detection | Single photodetector | Spectrometer or swept-source laser |
| Speed | Slower (~1-2 kHz A-scan rate) | Faster (20-200 kHz A-scan rate) |
| Sensitivity | Lower | ~20-30 dB higher |
| Laryngeal use | Early systems | Current standard; reduces motion artifact |
4. OCT in the Larynx - Specific Applications
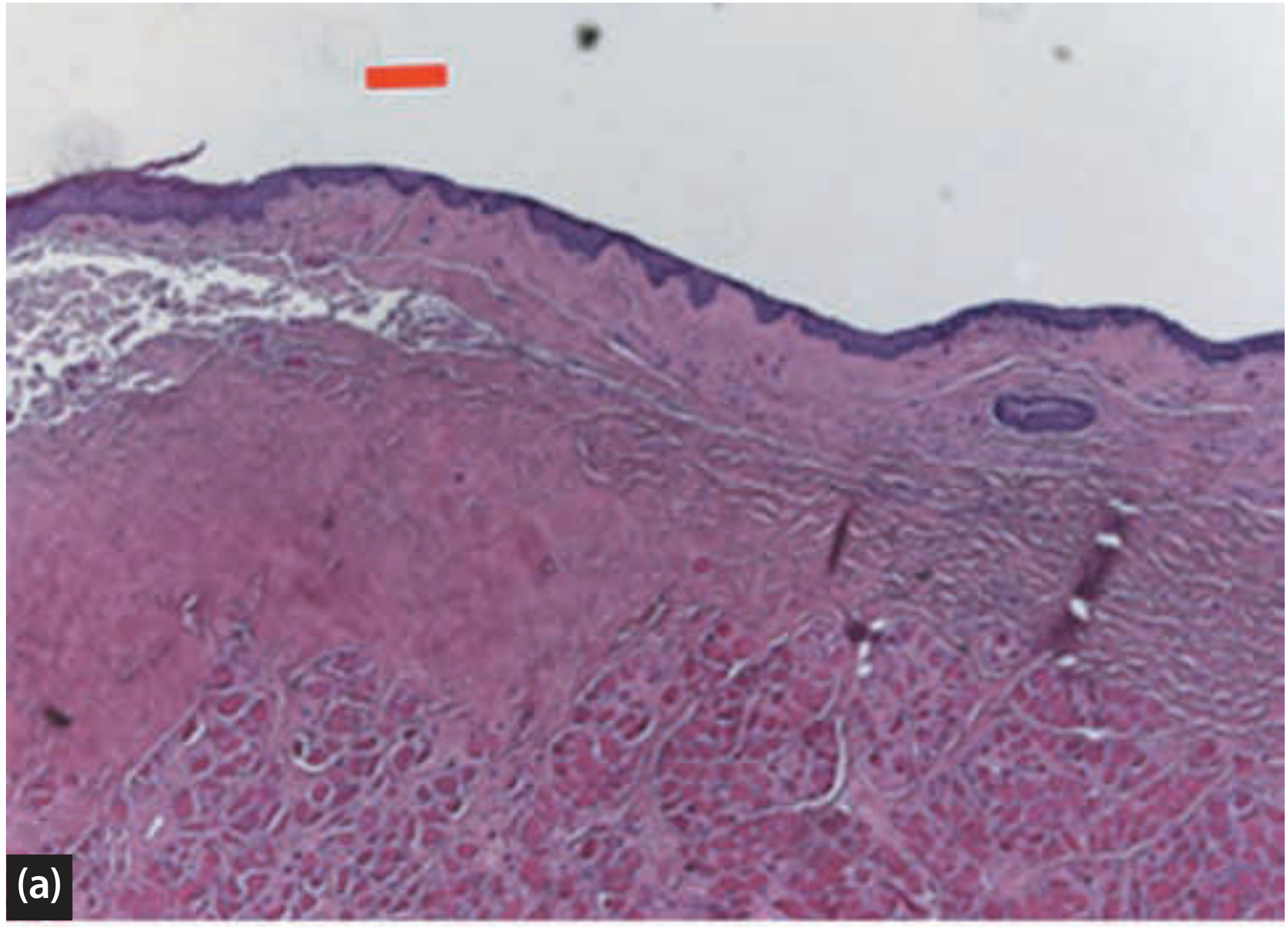
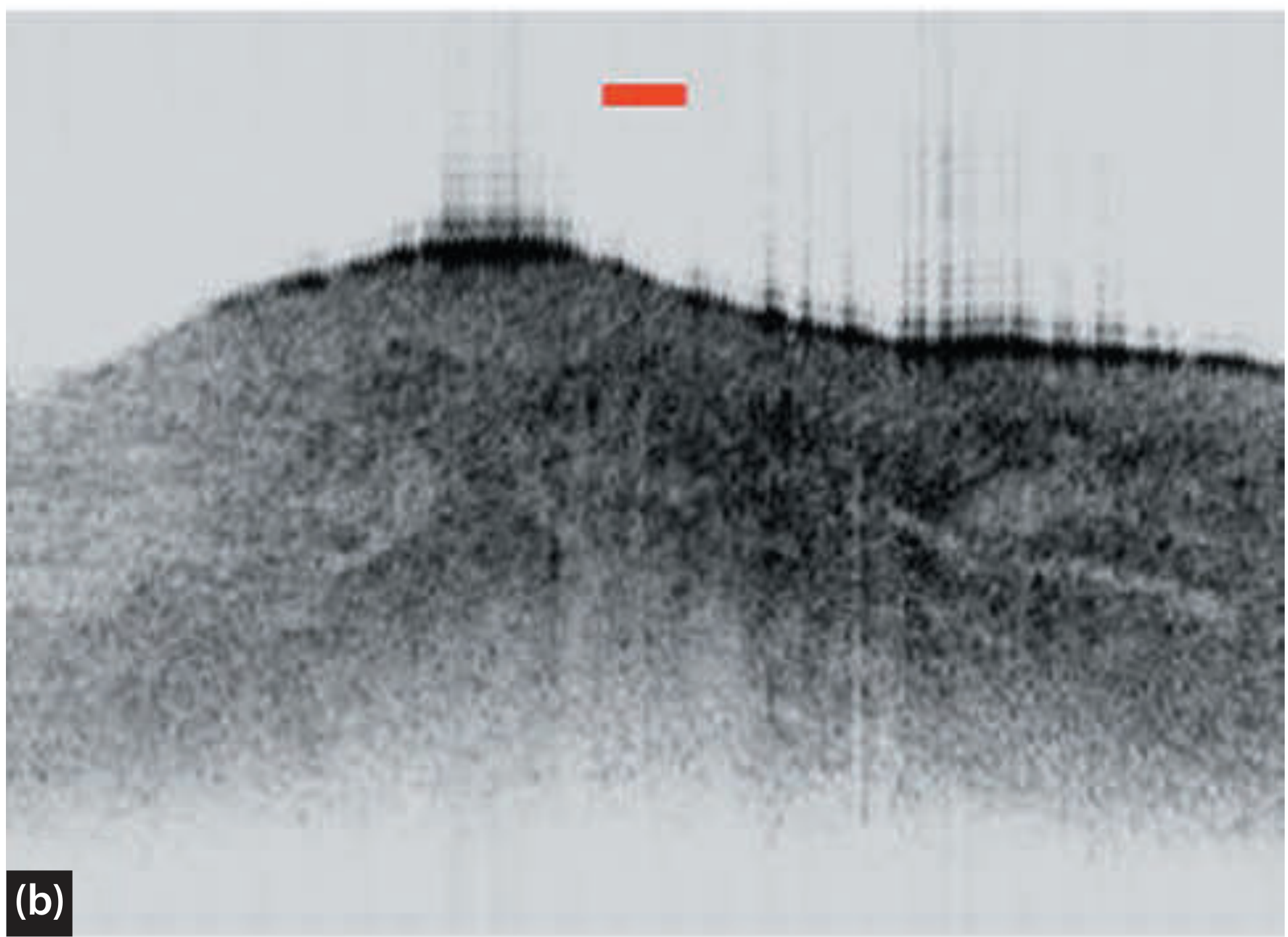
4.1 Normal Laryngeal Anatomy on OCT
- Stratified squamous epithelium (SS): Relatively uniform, moderately backscattering layer at the surface
- Basement membrane (BM): A thin, highly reflective bright band separating epithelium from lamina propria
- Lamina propria (LP): Deeper, heterogeneous zone of connective tissue
"Conventional OCT studies of healthy laryngeal tissues have demonstrated that OCT can detect spatial changes in the thickness and transparency of the epithelium, the content of the connective tissues including the presence of glands and vessels, as well as pronounced transitions in connective tissue type and the architecture of the basement membrane."
4.2 Detection of Basement Membrane Integrity
- In benign lesions (polyps, cysts, Reinke's oedema, papilloma), the BM remains intact and identifiable as a bright reflective band
- In carcinoma in situ (CIS), the BM is intact but the epithelial architecture is disordered
- In microinvasive SCC, the BM is disrupted - irregular, discontinuous, or completely absent - with tumour nests penetrating into the submucosa

4.3 Vocal Fold Vibration and Dynamic OCT
4.4 Pediatric Laryngology
- Develop computerized airway models for predicting neonatal subglottic stenosis following prolonged intubation
- Localize the site of upper airway obstruction in children with sleep-disordered breathing
- Image pediatric vocal fold paralysis intraoperatively to assess mucosal integrity and extracellular matrix changes
4.5 Subglottic / Tracheal Applications
4.6 Other ENT Applications
| Site | Application |
|---|---|
| Middle ear / tympanic membrane | Identification of myringitis, biofilm, stapes footplate in revision stapes surgery, tympanic membrane microanatomy |
| Cochlear implantation | Robotic electrode placement guidance, cochleostomy planning |
| Nasal/sinonasal | Feasibility studies for mucosal imaging |
| Oral cavity | Mucosal dysplasia screening |
| Thyroid & parathyroid | Intraoperative tissue identification using OFDI and µOCT to distinguish parathyroid from surrounding tissue without frozen section |
5. Clinical Indications in Laryngology
- Evaluation of superficial and subtle laryngeal lesions - lesions suspicious for early cancer in which standard imaging and white-light endoscopy are indeterminate
- Differentiation of benign from microinvasive or early malignant lesions - particularly T1 glottic tumours, leukoplakia, and erythroplakia
- Assessment of basement membrane integrity in lesions suspicious for CIS or microinvasive SCC
- Grading of precancerous lesions (dysplasia) in conjunction with microlaryngoscopy
- Guiding targeted biopsy - identifying the most representative site for tissue sampling, reducing sampling error
- Surgical margin assessment following transoral laser microsurgery or endoscopic resection of laryngeal tumours
- Monitoring disease progression or response to treatment (radiotherapy, photodynamic therapy) without tissue removal
- Intraoperative real-time guidance during phonomicrosurgery under surgical microscopy
- Assessment of vocal fold scar - PS-OCT for collagen architecture and lamina propria layering
- Pediatric subglottis - post-intubation stenosis assessment and airway modelling
6. Contraindications
- Bulky or exophytic laryngeal lesions - the BM cannot be consistently identified because thick hypercellular tissue increases backscattering and limits light penetration; biopsy on clinical criteria alone is more appropriate in this situation
- Heavily keratinized surfaces - keratin scatters light intensely and may obscure deeper structures
- Active haemorrhage at the imaging site - blood absorbs and scatters NIR light, degrading image quality
- Severely obstructed airway - delivering a probe to the larynx in acute airway compromise is contraindicated; airway security takes priority
- Uncooperative or paediatric patient (for office-based awake OCT) - patient motion causes significant imaging artifact; general anaesthesia or microlaryngoscopy setting may be required
- Limitation to superficial imaging - OCT cannot evaluate deep cervical lymph nodes, cartilage invasion, or subglottic extension beyond 1-3 mm; CT/MRI remain essential for advanced staging
7. Delivery Methods
- Microlaryngoscopy-integrated OCT: Probe passed through the operating laryngoscope under general anaesthesia with the surgical microscope; allows hands-free OCT simultaneously with microscopic visualization. Good probe stability, minimal motion artifact.
- Office-based awake transnasal OCT: A flexible fiberoptic probe is introduced through the nasal passage to the larynx in an awake patient. Burns et al. described the largest published series of this technique, demonstrating feasibility for non-anaesthetic outpatient evaluation. Challenges include patient gag reflex, motion artifact, and short focal length requiring careful probe positioning.
- Handheld probe: Investigational; being explored for intraoperative use similar to a nerve stimulator.
- Surgical microscope-coupled OCT: Allows real-time imaging during phonomicrosurgery.
8. Advantages
| Advantage | Details |
|---|---|
| Near-histological resolution | 1-15 µm axial; resolves epithelium, BM, lamina propria - unmatched by any other real-time in vivo modality |
| No tissue removal required | "Optical biopsy" - avoids the risks of conventional biopsy (airway compromise, scar formation, haemorrhage) |
| No ionizing radiation | Safe for repeated use and monitoring; suitable for paediatric patients |
| Real-time imaging | Immediate feedback during surgery or office assessment |
| No general anaesthesia (office-based) | OCT of the awake larynx is feasible; reduces procedural burden for surveillance |
| 3D volumetric capability | Modern SS-OCT can produce 3D datasets for anatomical modelling |
| Functional/dynamic imaging | High-speed OCT can image vibrating vocal folds; PS-OCT maps collagen organization |
| Adjunct to endoscopy | Complements white-light, NBI, and autofluorescence endoscopy to increase diagnostic accuracy |
| Intraoperative guidance | Assists in defining surgical margins during transoral laser microsurgery |
| Surgical monitoring | Allows objective surveillance of disease post-treatment without repeated biopsies |
| No contrast agents or radiotracers | Completely label-free; no nephrotoxicity or allergic risk |
9. Disadvantages and Limitations
| Disadvantage | Details |
|---|---|
| Limited depth penetration | Only 1-3 mm; cannot assess deep invasion, cartilage, or lymph nodes - CT/MRI still essential for staging |
| Unreliable BM assessment in bulky lesions | Thick hypercellular tumours scatter light intensely; the BM cannot be consistently identified in large exophytic lesions |
| Motion artifact | Patient movement (swallowing, phonation, respiration) causes image degradation, especially in awake studies; higher frame-rate FD-OCT partially mitigates this |
| Short focal length probes | Requires steady, close contact or near-contact positioning of the probe on target tissue - technically demanding |
| Steep learning curve | Interpreting OCT images requires specific training to correlate grey-scale patterns with tissue architecture; not yet standardized in ENT training |
| Limited lateral resolution | Commercial clinical probes sacrifice lateral resolution (50-100 µm) for portability and probe diameter |
| Cannot definitively replace histopathology | Current evidence is predominantly from non-randomized pilot and proof-of-concept studies; large-scale trials to justify replacement of excisional biopsy are lacking |
| Cost and infrastructure | OCT systems remain expensive; not universally available in ENT departments |
| Interference from secretions | Mucus on the vocal cord surface can degrade the image; surface cleaning or jet irrigation may be needed |
| Limited field of view | Single OCT image covers a small area (typically 2-4 mm wide); multiple acquisitions needed to survey the larynx |
| Not suitable for deep or large lesions | Clinically apparent large tumours proceed directly to biopsy - OCT adds no value over visual inspection in this context |
10. OCT Variants Relevant to ENT
- Polarization-sensitive OCT (PS-OCT): Exploits birefringence of organized collagen. Relevant for vocal fold scar, cartilage assessment, and distinguishing fibrotic from normal lamina propria.
- Fourier-domain OCT (FD-OCT) / Swept-source OCT (SS-OCT): Faster acquisition, less motion artifact, greater depth; preferred for in-office and intraoperative laryngeal work.
- Long-range OCT (LR-OCT): Extended depth of field; used for airway cross-sectional modelling in subglottic stenosis and paediatric airway.
- Optical frequency domain imaging (OFDI): High-speed variant; demonstrated for parathyroid identification in thyroid/parathyroid surgery.
- Micro-OCT (µOCT): Ultra-high resolution system offering ~1 µm axial resolution; still largely experimental but has been demonstrated for parathyroid tissue identification.
- Dynamic/4D OCT and optical Doppler tomography (ODT): Allows imaging of vocal fold vibration mechanics and mucosal wave motion in real time.
- Spectroscopic OCT: Encodes spectral information within the OCT signal to provide molecular contrast beyond pure structural imaging.
11. Current Evidence and Status
- Good histological correlation for normal and pathological laryngeal tissue has been demonstrated across multiple groups (Armstrong et al., 2006 [PMID 16826043]; Burns et al., 2012 [PMID 22913932])
- OCT in conjunction with microlaryngoscopy significantly increases sensitivity for distinguishing benign from malignant lesions and grading precancerous lesions compared to microlaryngoscopy alone
- Office-based awake transnasal OCT of the larynx has been demonstrated as feasible, with the potential to diagnose laryngeal lesions, guide targeted biopsy, and monitor disease noninvasively
- OCT is most useful for subtle superficial lesions - particularly potential T1 tumours, CIS, and early dysplastic disease
- Large-scale randomized studies to justify replacement of histological biopsy are lacking, and OCT currently serves as an adjunct rather than a replacement for tissue diagnosis
"Whilst these studies are predominantly non-randomized pilot or proof of concept studies they illustrate potential clinical applications for widespread clinical practice... we currently lack large-scale studies to justify replacement of histological confirmation." (p. 584)
12. Summary Table
| Parameter | Detail |
|---|---|
| Physical basis | Low-coherence interferometry; Michelson interferometer |
| Light source | Broadband NIR 800-1300 nm (SLD, swept-source laser) |
| Axial resolution | 1-15 µm (tissue) |
| Lateral resolution | 20-100 µm |
| Depth penetration | 1-3 mm |
| Primary laryngeal application | BM integrity assessment; benign vs early malignant distinction |
| Best suited lesions | Superficial, subtle; T1 glottic SCC, dysplasia, CIS, leukoplakia |
| Not suitable | Bulky exophytic tumours, deep invasion assessment |
| Key advantage | Real-time optical biopsy without tissue removal |
| Key limitation | Cannot replace histopathology; limited depth; motion artifact |
| Evidence level | Predominantly observational / non-randomized pilot studies |
13. Conclusion
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1, pp. 584-586; Vol 2, p. 962
- Cummings Otolaryngology Head and Neck Surgery, pp. 2287-2292
- Armstrong WB et al. Optical coherence tomography of laryngeal cancer. Laryngoscope 2006. [PMID 16826043]
- Burns JA. Optical coherence tomography: imaging the larynx. Curr Opin Otolaryngol Head Neck Surg 2012. [PMID 22913932]
- Tibbetts KM, Tan M. Role of Advanced Laryngeal Imaging in Glottic Cancer. Otolaryngol Clin North Am 2015. [PMID 26096138]
- Benboujja F, Hartnick C. Quantitative evaluation of the human vocal fold ECM using OCT. Sci Rep 2021. [PMID 33510352]
can you make the whole information into a pdf
ls -la /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace
mkdir -p /home/daytona/workspace/oct-larynx-pdf
~/oct-larynx-pdf/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.lib import colors
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import ListFlowable, ListItem
OUTPUT = "/home/daytona/workspace/oct-larynx-pdf/OCT_in_ENT_Larynx.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
rightMargin=2.2*cm,
leftMargin=2.2*cm,
topMargin=2.5*cm,
bottomMargin=2.5*cm,
title="Optical Coherence Tomography in ENT – Special Reference to the Larynx",
author="Orris Medical AI"
)
styles = getSampleStyleSheet()
# ── Custom styles ──────────────────────────────────────────────────────────────
NAVY = colors.HexColor("#1a3557")
TEAL = colors.HexColor("#1e6e8c")
LGRAY = colors.HexColor("#f4f6f9")
DGRAY = colors.HexColor("#555555")
BLACK = colors.black
title_style = ParagraphStyle(
"MainTitle",
parent=styles["Title"],
fontSize=20,
leading=26,
textColor=NAVY,
spaceAfter=6,
alignment=TA_CENTER,
fontName="Helvetica-Bold",
)
subtitle_style = ParagraphStyle(
"SubTitle",
parent=styles["Normal"],
fontSize=11,
leading=15,
textColor=TEAL,
spaceAfter=4,
alignment=TA_CENTER,
fontName="Helvetica-Oblique",
)
h1_style = ParagraphStyle(
"H1",
parent=styles["Heading1"],
fontSize=14,
leading=18,
textColor=colors.white,
spaceAfter=6,
spaceBefore=14,
fontName="Helvetica-Bold",
backColor=NAVY,
leftIndent=-0.3*cm,
rightIndent=-0.3*cm,
borderPad=5,
)
h2_style = ParagraphStyle(
"H2",
parent=styles["Heading2"],
fontSize=12,
leading=16,
textColor=NAVY,
spaceAfter=4,
spaceBefore=10,
fontName="Helvetica-Bold",
borderPad=2,
)
h3_style = ParagraphStyle(
"H3",
parent=styles["Heading3"],
fontSize=11,
leading=15,
textColor=TEAL,
spaceAfter=3,
spaceBefore=8,
fontName="Helvetica-BoldOblique",
)
body_style = ParagraphStyle(
"Body",
parent=styles["Normal"],
fontSize=10,
leading=15,
textColor=BLACK,
spaceAfter=6,
alignment=TA_JUSTIFY,
fontName="Helvetica",
)
bullet_style = ParagraphStyle(
"Bullet",
parent=body_style,
leftIndent=15,
spaceAfter=3,
bulletIndent=5,
)
quote_style = ParagraphStyle(
"Quote",
parent=body_style,
leftIndent=20,
rightIndent=20,
textColor=DGRAY,
fontName="Helvetica-Oblique",
borderPad=8,
backColor=LGRAY,
spaceAfter=8,
spaceBefore=4,
)
ref_style = ParagraphStyle(
"Ref",
parent=styles["Normal"],
fontSize=8.5,
leading=12,
textColor=DGRAY,
spaceAfter=3,
fontName="Helvetica",
)
caption_style = ParagraphStyle(
"Caption",
parent=styles["Normal"],
fontSize=8.5,
leading=12,
textColor=DGRAY,
fontName="Helvetica-Oblique",
alignment=TA_CENTER,
spaceAfter=6,
)
def h1(text):
return Paragraph(f" {text}", h1_style)
def h2(text):
return Paragraph(text, h2_style)
def h3(text):
return Paragraph(text, h3_style)
def body(text):
return Paragraph(text, body_style)
def bullet(items):
elems = []
for item in items:
elems.append(Paragraph(f"• {item}", bullet_style))
return elems
def quote(text):
return Paragraph(f'"{text}"', quote_style)
def spacer(h=0.3):
return Spacer(1, h*cm)
def hr():
return HRFlowable(width="100%", thickness=0.5, color=TEAL, spaceAfter=6, spaceBefore=4)
def make_table(headers, rows, col_widths=None):
data = [headers] + rows
if col_widths is None:
n = len(headers)
col_widths = [(doc.width / n)] * n
tbl = Table(data, colWidths=col_widths, repeatRows=1)
tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), NAVY),
("TEXTCOLOR", (0,0), (-1,0), colors.white),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 9),
("ALIGN", (0,0), (-1,0), "CENTER"),
("ROWBACKGROUNDS",(0,1),(-1,-1), [colors.white, LGRAY]),
("FONTNAME", (0,1), (-1,-1), "Helvetica"),
("FONTSIZE", (0,1), (-1,-1), 9),
("ALIGN", (0,1), (-1,-1), "LEFT"),
("VALIGN", (0,0), (-1,-1), "TOP"),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#cccccc")),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING",(0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING", (0,0), (-1,-1), 6),
]))
return tbl
# ── Document content ───────────────────────────────────────────────────────────
story = []
# ── COVER ──────────────────────────────────────────────────────────────────────
story.append(spacer(3))
story.append(Paragraph("Optical Coherence Tomography in ENT", title_style))
story.append(Paragraph("With Special Reference to the Larynx", subtitle_style))
story.append(spacer(0.5))
story.append(HRFlowable(width="60%", thickness=2, color=TEAL, spaceBefore=2, spaceAfter=8))
story.append(Paragraph(
"Principle · Mechanism · Uses · Indications · Contraindications · Advantages · Disadvantages",
subtitle_style
))
story.append(spacer(0.5))
story.append(Paragraph("Sources: Scott-Brown's ORL HNS · Cummings ORL HNS · Peer-reviewed literature", caption_style))
story.append(spacer(0.3))
story.append(Paragraph("Compiled by Orris Medical AI | June 2026", caption_style))
story.append(PageBreak())
# ── 1. INTRODUCTION ────────────────────────────────────────────────────────────
story.append(h1("1. Introduction"))
story.append(spacer(0.2))
story.append(body(
"Optical Coherence Tomography (OCT) is a non-contact, non-invasive, high-resolution optical "
"imaging modality that generates real-time cross-sectional images of biological tissue microstructure "
"at near-histological resolution (1–15 µm). First described for ophthalmic imaging in the early 1990s, "
"OCT has expanded into multiple specialties including cardiology, gastroenterology, pulmonology, and "
"otolaryngology. In ENT, the larynx has attracted the most clinical attention because OCT can image "
"the epithelium, basement membrane (BM), and lamina propria in vivo – without tissue removal – directly "
"addressing one of laryngology's most pressing diagnostic challenges: distinguishing benign mucosal "
"disease from early invasive malignancy."
))
story.append(body(
"Conventional cross-sectional imaging (CT, MRI, ultrasound) offers a spatial resolution of approximately "
"1 mm at best, which is of limited use for very superficial laryngeal lesions. OCT fills this gap with "
"10–20 µm axial resolution and tissue penetration of 1–3 mm, effectively enabling an <i>optical biopsy</i> "
"of the mucosal layers."
))
story.append(body(
"<i>Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 584; "
"Cummings Otolaryngology Head and Neck Surgery, p. 2287</i>"
))
story.append(spacer(0.3))
# ── 2. PHYSICAL PRINCIPLE ──────────────────────────────────────────────────────
story.append(h1("2. Physical Principle"))
story.append(spacer(0.2))
story.append(body(
"OCT operates on the principle of <b>low-coherence interferometry (LCI)</b> – the optical analogue "
"of pulse-echo ultrasound. While ultrasound measures the time delay of returning acoustic echoes, OCT "
"measures the time delay and intensity of backscattered near-infrared (NIR) light."
))
story.append(h2("Why Interferometry is Required"))
story.append(body(
"The speed of light (~3 × 10⁸ m/s) is so fast that the ~10 femtosecond echo delays from tissue "
"reflectors at micrometer depths cannot be measured with conventional electronics. Interferometry solves "
"this by comparing backscattered sample light with a reference beam of known optical path length, "
"generating an interference signal only when the two beam paths are matched to within the light source's "
"coherence length."
))
story.append(h2("Key Optical Parameters"))
story.append(make_table(
["Parameter", "Value / Detail"],
[
["Wavelength", "800–1300 nm near-infrared (NIR)"],
["Axial resolution", "1–15 µm in tissue (determined by coherence length of light source)"],
["Lateral resolution","20–100 µm (determined by beam optics / focal spot size)"],
["Depth penetration", "1–3 mm (limited by optical scattering; ~1–2 mm in most turbid tissues)"],
["Light source", "Superluminescent diode (SLD) or swept-source laser (broadband)"],
],
col_widths=[5.5*cm, 11.5*cm]
))
story.append(spacer(0.3))
# ── 3. MECHANISM OF IMAGE FORMATION ───────────────────────────────────────────
story.append(h1("3. Mechanism of Image Formation"))
story.append(spacer(0.2))
story.append(h2("3.1 The Michelson Interferometer"))
story.append(body(
"The core of every OCT system is a <b>Michelson interferometer</b> with a broadband (low-coherence) "
"light source. Light from the source is split by a beam-splitter into two arms:"
))
story += bullet([
"<b>Sample arm:</b> Light is directed into tissue via a probe or endoscopic catheter. At each depth, "
"small amounts of light are backscattered due to variation in optical refractive index between tissue "
"components (cell membranes, organelles, collagen fibres, basement membrane, vessels).",
"<b>Reference arm:</b> Light travels to a mirror at a precisely known distance and returns to the "
"beam-splitter.",
])
story.append(spacer(0.2))
story.append(body(
"The two beams recombine at a photodetector. Constructive interference – and therefore a detectable "
"signal – occurs <b>only</b> when the optical path lengths of both arms match to within the coherence "
"length (~1–15 µm). By scanning the reference path length or using Fourier-domain detection, OCT "
"reconstructs a depth-resolved reflectivity profile – the <b>A-scan</b>."
))
story.append(h2("3.2 From A-Scan to 2D Image"))
story += bullet([
"<b>A-scan:</b> One axial reflectivity profile at a single lateral point.",
"<b>B-scan:</b> Multiple A-scans acquired as the beam sweeps laterally – produces a 2D cross-sectional "
"image equivalent to a vertical histological section.",
"<b>C-scan / en face:</b> Lateral scanning at fixed depth, producing a face-on confocal-like view.",
])
story.append(spacer(0.2))
story.append(h2("3.3 Time-Domain vs Fourier-Domain OCT"))
story.append(make_table(
["Feature", "Time-Domain OCT (TD-OCT)", "Fourier-Domain OCT (FD-OCT)"],
[
["Reference mirror", "Mechanically scanned", "Fixed"],
["Detection", "Single photodetector", "Spectrometer or swept-source laser"],
["Acquisition speed", "Slower (~1–2 kHz A-scan)", "Faster (20–200 kHz A-scan)"],
["Sensitivity", "Lower", "~20–30 dB higher"],
["Motion artifact", "More susceptible", "Less; preferred for laryngeal work"],
],
col_widths=[4*cm, 7*cm, 6*cm]
))
story.append(spacer(0.3))
story.append(h2("3.4 OCT Variants Relevant to ENT"))
story.append(make_table(
["Variant", "Key Feature", "ENT Application"],
[
["PS-OCT (Polarization-sensitive)", "Maps birefringence of organized collagen", "Vocal fold scar, lamina propria layers, cartilage"],
["SS-OCT / OFDI (Swept-source)", "Very high speed; deeper imaging", "Intraoperative larynx, parathyroid ID"],
["LR-OCT (Long-range)", "Extended depth of field", "Subglottic stenosis, paediatric airway modelling"],
["µOCT (Micro-OCT)", "Ultra-high ~1 µm axial resolution", "Parathyroid identification; experimental"],
["Dynamic / 4D OCT + ODT", "Images tissue mechanics in real time", "Vocal fold vibration, mucosal wave analysis"],
["Spectroscopic OCT", "Molecular spectral contrast added", "Experimental tissue characterization"],
],
col_widths=[4.5*cm, 6*cm, 6.5*cm]
))
story.append(spacer(0.3))
# ── 4. OCT IN THE LARYNX ──────────────────────────────────────────────────────
story.append(h1("4. OCT in the Larynx – Specific Applications"))
story.append(spacer(0.2))
story.append(h2("4.1 Normal Laryngeal Anatomy on OCT"))
story.append(body(
"On a normal true vocal fold OCT image, three distinct layers are typically resolved:"
))
story += bullet([
"<b>Stratified squamous epithelium (SS):</b> Relatively uniform, moderately backscattering surface layer.",
"<b>Basement membrane (BM):</b> A thin, highly reflective bright band separating epithelium from lamina propria.",
"<b>Lamina propria (LP):</b> Deeper, heterogeneous zone of connective tissue with glands and vessels.",
])
story.append(spacer(0.2))
story.append(quote(
"Conventional OCT studies of healthy laryngeal tissues have demonstrated that OCT can detect spatial changes "
"in the thickness and transparency of the epithelium, the content of the connective tissues including the "
"presence of glands and vessels, as well as pronounced transitions in connective tissue type and the "
"architecture of the basement membrane."
))
story.append(Paragraph("– Scott-Brown's ORL HNS, p. 584", caption_style))
story.append(spacer(0.2))
story.append(h2("4.2 Detection of Basement Membrane Integrity (Most Critical Application)"))
story.append(body(
"The single most clinically significant laryngeal application of OCT is <b>assessing basement membrane "
"(BM) integrity</b> to distinguish benign/dysplastic mucosal disease from microinvasive or invasive "
"squamous cell carcinoma (SCC)."
))
story.append(make_table(
["Pathology", "BM on OCT", "Epithelial Architecture"],
[
["Normal", "Intact bright band", "Regular, stratified"],
["Benign lesions (polyp, cyst, Reinke's oedema, papilloma)", "Intact", "Variable thickening/oedema"],
["Dysplasia / CIS", "Intact but may be irregular", "Disordered; thickened rete pegs"],
["Microinvasive SCC", "Disrupted, discontinuous, or absent", "Irregular nests penetrating submucosa"],
["Invasive SCC", "Not identifiable", "Tumour bulk obscures deep layers"],
],
col_widths=[5*cm, 5.5*cm, 6.5*cm]
))
story.append(spacer(0.2))
story.append(body(
"OCT in conjunction with microlaryngoscopy has been shown to <b>significantly increase the sensitivity</b> "
"for determining benign versus malignant lesions and the grade of precancerous lesions compared to "
"microlaryngoscopy alone. (Scott-Brown's Vol 2, p. 962)"
))
story.append(spacer(0.2))
story.append(h2("4.3 Vocal Fold Vibration and Dynamic OCT"))
story.append(body(
"High-speed OCT systems operating at 1050 nm with swept-source detection can image vibrating vocal folds "
"in real time. Dynamic/4D-OCT and optical Doppler tomography (ODT) allow visualization of the mucosa wave "
"and tissue mechanics during phonation, relevant for assessing scar stiffness and post-surgical changes."
))
story.append(h2("4.4 Paediatric Laryngology"))
story += bullet([
"Long-range OCT (LR-OCT) and FD-OCT are used to develop computerised airway models for predicting "
"<b>neonatal subglottic stenosis</b> following prolonged intubation.",
"Localisation of upper airway obstruction in children with <b>sleep-disordered breathing</b>.",
"Intraoperative imaging of <b>paediatric vocal fold paralysis</b> to assess mucosal integrity and "
"extracellular matrix changes.",
])
story.append(spacer(0.2))
story.append(h2("4.5 Subglottic / Tracheal Applications"))
story.append(body(
"OCT combined with endobronchial ultrasound (EBUS) has been used intraoperatively for patients with "
"<b>post-intubation laryngotracheal stenosis</b> undergoing laser dilatation – to identify residual "
"hypertrophic or inflammatory tissue (contributors to stricture recurrence) that may not be visible "
"endoscopically."
))
story.append(h2("4.6 Other ENT Applications"))
story.append(make_table(
["ENT Site", "Application"],
[
["Middle ear / tympanic membrane", "Myringitis, biofilm detection, stapes footplate localisation in revision surgery, tympanic membrane microanatomy"],
["Cochlear implantation (Otology)", "Robotic electrode placement guidance; cochleostomy planning in dry-fixed temporal bones"],
["Nasal / sinonasal", "Feasibility studies for mucosal imaging; rhinosinusitis monitoring"],
["Oral cavity", "Mucosal dysplasia screening; guidance of biopsies"],
["Thyroid & parathyroid", "Intraoperative tissue identification (OFDI + µOCT) – histology-like certainty without frozen section"],
],
col_widths=[5*cm, 12*cm]
))
story.append(spacer(0.3))
# ── 5. DELIVERY METHODS ───────────────────────────────────────────────────────
story.append(h1("5. Delivery Methods"))
story.append(spacer(0.2))
story.append(make_table(
["Method", "Description", "Key Advantage"],
[
["Microlaryngoscopy-integrated OCT",
"Probe passed through the operating laryngoscope under general anaesthesia with surgical microscope",
"Stable positioning; hands-free; minimal motion artifact"],
["Office-based awake transnasal OCT",
"Flexible fiberoptic probe introduced transnasally in the awake patient",
"No anaesthesia; suitable for surveillance and monitoring"],
["Surgical microscope-coupled OCT",
"OCT system optically coupled to operating microscope",
"Real-time imaging during phonomicrosurgery"],
["Handheld probe OCT",
"Portable handheld device; investigational",
"Flexible intraoperative use; analogous to nerve stimulator"],
],
col_widths=[4.5*cm, 7.5*cm, 5*cm]
))
story.append(spacer(0.3))
# ── 6. INDICATIONS ────────────────────────────────────────────────────────────
story.append(h1("6. Clinical Indications in Laryngology"))
story.append(spacer(0.2))
indications = [
"Evaluation of <b>superficial and subtle laryngeal lesions</b> – lesions suspicious for early cancer "
"in which standard imaging and white-light endoscopy are indeterminate.",
"Differentiation of <b>benign from microinvasive or early malignant lesions</b> – particularly T1 "
"glottic tumours, leukoplakia, and erythroplakia.",
"<b>Assessment of basement membrane integrity</b> in lesions suspicious for CIS or microinvasive SCC.",
"<b>Grading of precancerous lesions</b> (dysplasia) in conjunction with microlaryngoscopy.",
"<b>Guiding targeted biopsy</b> – identifying the most representative site for tissue sampling and "
"reducing sampling error.",
"<b>Surgical margin assessment</b> following transoral laser microsurgery or endoscopic resection.",
"<b>Monitoring disease progression or treatment response</b> (radiotherapy, photodynamic therapy) "
"without tissue removal.",
"<b>Intraoperative real-time guidance</b> during phonomicrosurgery under surgical microscopy.",
"<b>Assessment of vocal fold scar</b> – PS-OCT maps collagen architecture and lamina propria layering.",
"<b>Paediatric subglottis</b> – post-intubation stenosis assessment and airway anatomical modelling.",
]
story += bullet(indications)
story.append(spacer(0.3))
# ── 7. CONTRAINDICATIONS ─────────────────────────────────────────────────────
story.append(h1("7. Contraindications"))
story.append(spacer(0.2))
story.append(body(
"OCT has <b>no absolute contraindications</b> as an imaging modality itself – it emits no ionising "
"radiation and uses eye-safe NIR light at low power. Contraindications relate to delivery method and "
"patient context:"
))
story.append(spacer(0.1))
story.append(make_table(
["Contraindication / Limitation", "Reason"],
[
["Bulky / exophytic laryngeal lesions",
"BM cannot be consistently identified; thick hypercellular tissue increases backscattering and limits "
"light penetration. Biopsy on clinical criteria alone is more appropriate."],
["Heavily keratinised surfaces",
"Keratin scatters light intensely, obscuring deeper structures and degrading image quality."],
["Active haemorrhage at imaging site",
"Blood absorbs and scatters NIR light, rendering images uninterpretable."],
["Severely obstructed airway",
"In acute airway compromise, probe delivery to the larynx is dangerous; airway security takes priority."],
["Uncooperative / paediatric patient (office-based)",
"Patient motion causes significant image artifact; microlaryngoscopy under GA is preferred."],
["Need for deep invasion staging",
"OCT penetrates only 1–3 mm; CT/MRI remain essential for subglottic extension, cartilage invasion, "
"and lymph node assessment."],
],
col_widths=[6*cm, 11*cm]
))
story.append(spacer(0.3))
# ── 8. ADVANTAGES ─────────────────────────────────────────────────────────────
story.append(h1("8. Advantages"))
story.append(spacer(0.2))
story.append(make_table(
["Advantage", "Detail"],
[
["Near-histological resolution",
"1–15 µm axial resolution resolves epithelium, BM, lamina propria – unmatched by any other real-time in vivo modality."],
["No tissue removal required",
"'Optical biopsy' – avoids risks of conventional biopsy (airway compromise, scar formation, haemorrhage)."],
["No ionising radiation",
"Safe for repeated use and monitoring; suitable for pregnant patients and children."],
["Real-time imaging",
"Immediate feedback during surgery or outpatient assessment."],
["No general anaesthesia (office-based)",
"OCT of the awake larynx is feasible; reduces procedural burden for surveillance."],
["3D volumetric capability",
"Modern SS-OCT produces 3D datasets for anatomical modelling (e.g., subglottic stenosis)."],
["Functional / dynamic imaging",
"High-speed OCT images vibrating vocal folds; PS-OCT maps collagen organisation and scar."],
["Adjunct to endoscopy",
"Complements white-light, NBI, and autofluorescence endoscopy to increase diagnostic accuracy."],
["Intraoperative surgical guidance",
"Assists in defining surgical margins during transoral laser microsurgery."],
["Post-treatment monitoring",
"Objective surveillance of disease response without repeated biopsies or radiation."],
["No contrast agents / radiotracers",
"Completely label-free; no nephrotoxicity, anaphylaxis risk, or radiotracer dose."],
],
col_widths=[5.5*cm, 11.5*cm]
))
story.append(spacer(0.3))
# ── 9. DISADVANTAGES ─────────────────────────────────────────────────────────
story.append(h1("9. Disadvantages and Limitations"))
story.append(spacer(0.2))
story.append(make_table(
["Disadvantage", "Detail"],
[
["Limited depth penetration",
"Only 1–3 mm; cannot assess deep invasion, cartilage involvement, or cervical lymph nodes. CT/MRI "
"remain essential for advanced staging."],
["Unreliable BM assessment in bulky lesions",
"Thick hypercellular tumours scatter light intensely; BM cannot be consistently identified in large "
"exophytic lesions."],
["Motion artifact",
"Patient movement (swallowing, breathing, phonation) degrades image quality, especially in awake "
"studies. Higher frame-rate FD-OCT partially mitigates this."],
["Short focal length probes",
"Requires steady, close or near-contact probe positioning on target tissue – technically demanding "
"in mobile laryngeal structures."],
["Steep learning curve",
"Interpreting grey-scale OCT patterns requires specific training; not yet standardised in ENT training."],
["Limited lateral resolution",
"Commercial clinical probes sacrifice lateral resolution (50–100 µm) for portability and small probe diameter."],
["Cannot replace histopathology",
"Evidence is predominantly non-randomised pilot studies; large-scale RCTs to justify replacing "
"excisional biopsy are lacking."],
["Cost and infrastructure",
"OCT systems remain expensive and not universally available in ENT departments."],
["Interference from secretions",
"Mucus on the vocal cord surface degrades the image; surface cleaning or jet irrigation may be needed."],
["Limited field of view",
"Single OCT image typically covers only 2–4 mm laterally; multiple acquisitions needed for laryngeal survey."],
["Not useful for large lesions",
"Clinically apparent bulky tumours proceed directly to biopsy – OCT adds no value over visual inspection."],
],
col_widths=[5.5*cm, 11.5*cm]
))
story.append(spacer(0.3))
# ── 10. CURRENT EVIDENCE ─────────────────────────────────────────────────────
story.append(h1("10. Current Evidence and Clinical Status"))
story.append(spacer(0.2))
story.append(body(
"The clinical evidence base for laryngeal OCT consists predominantly of non-randomised pilot and "
"proof-of-concept studies. Key findings from published literature include:"
))
story += bullet([
"Good histological correlation for normal and pathological laryngeal tissue has been demonstrated across "
"multiple groups (Armstrong et al., 2006; Burns et al., 2012).",
"OCT in conjunction with microlaryngoscopy <b>significantly increases sensitivity</b> for distinguishing "
"benign from malignant lesions and grading precancerous lesions compared to microlaryngoscopy alone.",
"Office-based awake transnasal OCT of the larynx has been demonstrated as feasible for diagnosing "
"laryngeal lesions, guiding targeted biopsy, and monitoring disease non-invasively.",
"OCT is <b>most useful for subtle superficial lesions</b> – particularly potential T1 tumours, CIS, "
"and early dysplastic disease.",
"<b>Large-scale prospective RCTs</b> to justify replacement of histological biopsy are lacking; OCT "
"currently serves as an adjunct rather than a replacement for tissue diagnosis.",
])
story.append(spacer(0.2))
story.append(quote(
"Whilst these studies are predominantly non-randomized pilot or proof of concept studies they illustrate "
"potential clinical applications for widespread clinical practice... we currently lack large-scale studies "
"to justify replacement of histological confirmation."
))
story.append(Paragraph("– Scott-Brown's ORL HNS, p. 584", caption_style))
story.append(spacer(0.3))
# ── 11. SUMMARY TABLE ─────────────────────────────────────────────────────────
story.append(h1("11. Summary Reference Table"))
story.append(spacer(0.2))
story.append(make_table(
["Parameter", "Detail"],
[
["Physical basis", "Low-coherence interferometry (LCI); Michelson interferometer"],
["Light source", "Broadband NIR 800–1300 nm (SLD, swept-source laser)"],
["Axial resolution", "1–15 µm in tissue"],
["Lateral resolution", "20–100 µm (probe-dependent)"],
["Depth penetration", "1–3 mm (1–2 mm practical in turbid tissues)"],
["Image output", "2D cross-sectional B-scan; 3D volumetric with SS-OCT"],
["Primary laryngeal application", "Basement membrane integrity; benign vs early malignant distinction"],
["Best suited lesions", "Superficial, subtle; T1 glottic SCC, dysplasia, CIS, leukoplakia"],
["Not suitable for", "Bulky exophytic tumours; deep invasion; staging of advanced disease"],
["Key advantage", "Real-time optical biopsy without tissue removal or ionising radiation"],
["Key limitation", "Cannot replace histopathology; limited depth; motion artifact"],
["Evidence level", "Predominantly observational / non-randomised pilot studies"],
],
col_widths=[6*cm, 11*cm]
))
story.append(spacer(0.3))
# ── 12. CONCLUSION ────────────────────────────────────────────────────────────
story.append(h1("12. Conclusion"))
story.append(spacer(0.2))
story.append(body(
"OCT represents a genuinely promising addition to the laryngologist's diagnostic armamentarium. Its "
"capacity to image tissue microstructure in real time, at near-histological resolution, without tissue "
"removal or radiation makes it uniquely suited to the larynx – an organ where even a small biopsy carries "
"risk of scar, voice change, or airway compromise. The technology's greatest current value lies in "
"evaluating subtle mucosal abnormalities, assessing basement membrane integrity in early glottic lesions, "
"guiding targeted biopsy, and monitoring post-treatment response."
))
story.append(body(
"However, OCT remains a technology in development for ENT practice. The limiting factors are its restricted "
"depth of penetration, motion artifact in awake patients, limited lateral resolution in current clinical "
"probes, and the absence of large prospective trials comparing OCT-guided decision-making against standard "
"histopathology. Until such evidence exists, OCT functions best as a high-value adjunct to microlaryngoscopy "
"and endoscopy rather than as an independent diagnostic tool."
))
story.append(body(
"The next decade of research – driven by faster swept-source systems, AI-assisted OCT image interpretation, "
"and miniaturised handheld probes – holds considerable potential to move this technology from the research "
"laboratory into routine laryngological practice."
))
story.append(spacer(0.3))
# ── REFERENCES ────────────────────────────────────────────────────────────────
story.append(h1("References"))
story.append(spacer(0.2))
refs = [
"Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1, pp. 584–586; Vol 2, p. 962. "
"Eds. Gleeson M et al. CRC Press / Taylor & Francis, 8th ed.",
"Cummings Otolaryngology Head and Neck Surgery, pp. 2287–2292. Eds. Flint PW et al. Elsevier, 7th ed.",
"Armstrong WB, Ridgway JM, Vokes DE, et al. Optical coherence tomography of laryngeal cancer. "
"Laryngoscope. 2006;116(7):1107–13. [PMID 16826043]",
"Burns JA. Optical coherence tomography: imaging the larynx. "
"Curr Opin Otolaryngol Head Neck Surg. 2012;20(6):477–81. [PMID 22913932]",
"Tibbetts KM, Tan M. Role of Advanced Laryngeal Imaging in Glottic Cancer: Early Detection and "
"Evaluation of Glottic Neoplasms. Otolaryngol Clin North Am. 2015;48(4):625–40. [PMID 26096138]",
"Benboujja F, Hartnick C. Quantitative evaluation of the human vocal fold extracellular matrix "
"using multiphoton microscopy and optical coherence tomography. Sci Rep. 2021;11(1):2551. [PMID 33510352]",
"Nourmahnad A, Benboujja F, Hartnick CJ. Using intraoperative optical coherence tomography to image "
"pediatric unilateral vocal fold paralysis. Int J Pediatr Otorhinolaryngol. 2019;121:191–94. [PMID 30877978]",
"Shakhova M et al. Optical coherence tomography in otolaryngology: current opportunities and perspectives "
"for use. Almanac of Clinical Medicine. 2025.",
"Israelsen N, Larsen CF, Pedersen M. Quantitative examination of vocal cords with high-speed video and "
"optical coherence tomography. Ugeskr Laeger. 2022;184(6). [PMID 35179120]",
]
for i, r in enumerate(refs, 1):
story.append(Paragraph(f"{i}. {r}", ref_style))
story.append(spacer(0.1))
# ── BUILD ──────────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF created: {OUTPUT}")
I used it only once today , how can credits be over