Ectopic pregnancy
Reading File
Finding Sources
Searching PubMed
"ectopic pregnancy"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to write a thorough, well-structured answer on ectopic pregnancy. Let me compile everything.
Ectopic Pregnancy
Definition
Ectopic pregnancy refers to implantation of the fertilized ovum outside the uterine corpus. Approximately 1-2% of pregnancies are ectopic, making it the most common obstetric cause of maternal death in the first trimester. - Robbins & Kumar Basic Pathology, Roberts & Hedges' Clinical Procedures in Emergency Medicine
Sites of Implantation
| Site | Frequency |
|---|---|
| Fallopian tube (ampulla most common) | ~90% |
| Ovary | Rare |
| Abdominal cavity (peritoneum) | Rare |
| Interstitial / cornual (intramural tube) | Rare but high rupture risk |
| Cervical | Very rare |
Ovarian pregnancies occur when the ovum is fertilized just as the follicle ruptures. Abdominal pregnancies result when a fertilized egg exits the fimbriated end and implants on the peritoneum. - Robbins & Kumar Basic Pathology, p. 909
Risk Factors
The single most important predisposing condition is intraluminal fallopian tube scarring secondary to chronic salpingitis (pelvic inflammatory disease). Other significant risk factors include:
- Previous ectopic pregnancy
- Prior tubal surgery (including sterilization - especially laparoscopic partial salpingectomy or electrodestruction, particularly in women <28 years, 5-15 years after the procedure)
- Intrauterine contraceptive device (2-fold increased risk)
- Endometriosis / peritubal adhesions (appendicitis, prior surgery)
- Intrauterine tumors
- Infertility / assisted reproduction
- Smoking
Note: In many cases no anatomic cause is identified. - Roberts & Hedges', Robbins & Kumar
Pathology / Morphology
Early ectopic development proceeds normally - placental tissue, amniotic sac, and decidual changes all form. With tubal pregnancies, the invading placenta eventually burrows through the wall of the fallopian tube, causing:
- Hematosalpinx - intratubal hematoma
- Intraperitoneal hemorrhage
The tube is distended by clotted blood containing bits of placental and fetal tissue. Histologic diagnosis depends on visualization of placental villi or (rarely) the embryo. - Robbins & Kumar Basic Pathology, p. 912-914
Clinical Features
Classic triad (present in only ~45% of cases):
- Amenorrhea
- Vaginal bleeding / abnormal menses
- Unilateral lower abdominal/pelvic pain
Other presentations:
- Shoulder/referred pain (diaphragmatic irritation from hemoperitoneum)
- Adnexal mass and tenderness
- Cervical motion tenderness
- Syncope / near-syncope
- Isolated rectal or back pain
- Leukocytosis, anemia
Critically: Blood in the peritoneal cavity does NOT consistently correlate with peritoneal irritation, changes in blood pressure, or pulse rate. Relative bradycardia may occur in the presence of significant intraperitoneal bleeding (vagal stimulation). Vital signs may be completely normal even with significant hemoperitoneum. Fever is rare. - Roberts & Hedges' Clinical Procedures in Emergency Medicine
In one series of 300 consecutive cases, 50% of patients received medical evaluation at least twice before the correct diagnosis was made.
Diagnosis
Definitive diagnosis is made by ultrasound, laparoscopy, or at surgery. No single laboratory test has sufficient predictive value alone.
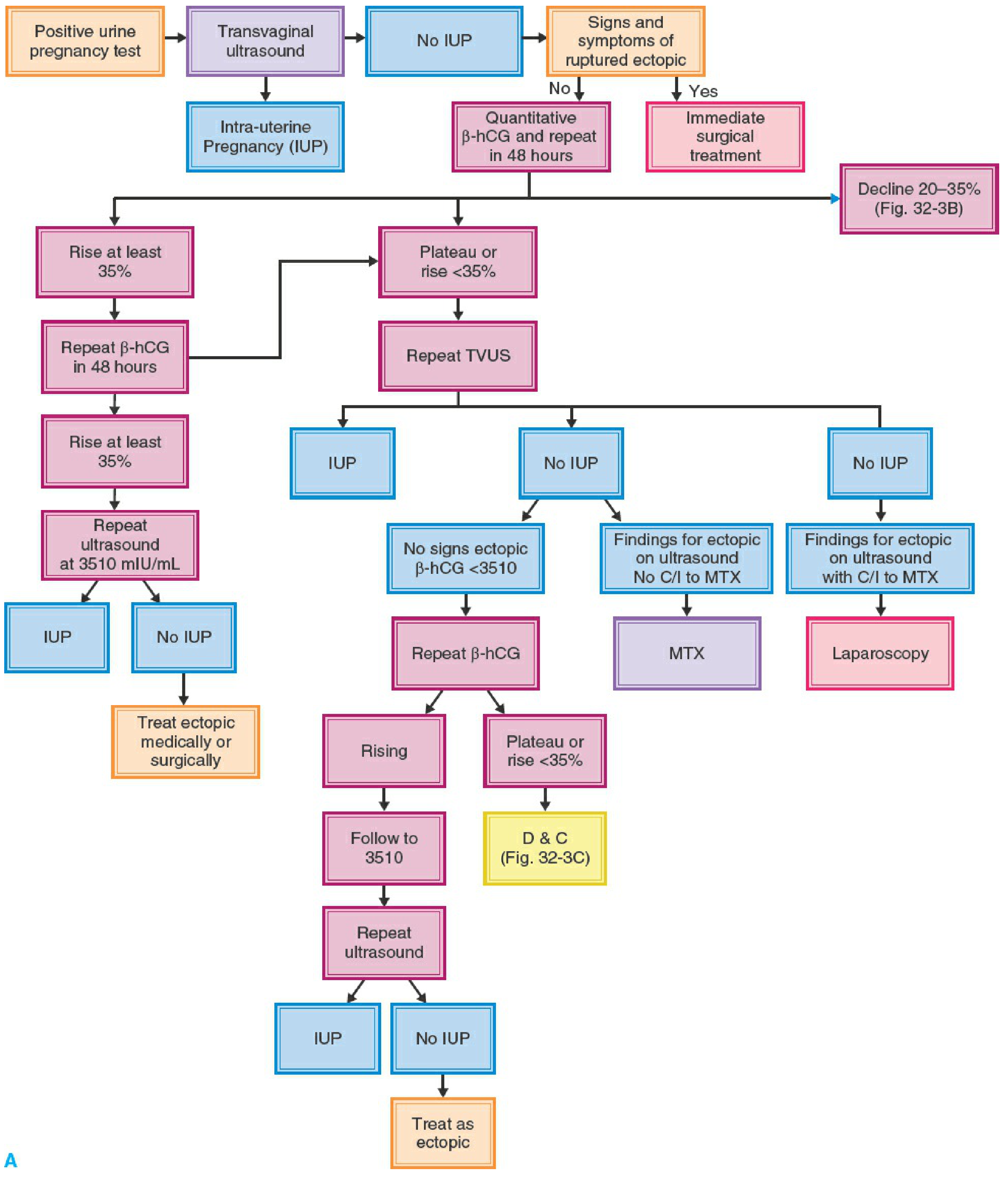
1. Serum β-hCG
- In a normal IUP, β-hCG rises ≥35% every 48 hours in early pregnancy (older literature cited 66%, but 35% is a more practical threshold)
- A plateau or rise <35% in 48 hours suggests ectopic pregnancy or a failing IUP
- A discriminatory zone exists: transvaginal US should detect an IUP at β-hCG ≥1,200-2,000 mIU/mL; transabdominal US at ≥6,000 mIU/mL
- When no IUP is seen by TVUS and β-hCG exceeds the discriminatory zone, probability of ectopic pregnancy is 86-100%
- A single quantitative β-hCG level is a poor predictor of ectopic pregnancy risk by itself
2. Transvaginal Ultrasound (TVUS) - First-Line Imaging
- An empty uterus combined with positive β-hCG is strongly suggestive
- An adnexal mass separate from the ovary is the most specific finding
- A gestational sac outside the uterus with a yolk sac or fetal pole confirms the diagnosis
- Fetal pole and cardiac activity detectable at ~6-7 weeks by endovaginal US
- Free fluid in the cul-de-sac suggests hemoperitoneum
3. Culdocentesis
- Accuracy 85-95% for detecting hemoperitoneum
- Positive test + positive pregnancy test = 99% probability of ectopic pregnancy (Romero et al.)
- Hemoperitoneum found in 45-60% of unruptured ectopic pregnancies
- A negative culdocentesis does not rule out ectopic pregnancy
Management
A. Surgical Treatment (most widely used)
Indications for surgery: hemodynamic instability, rupture, contraindications to methotrexate, failed medical management, or clinician/patient preference.
Laparoscopy vs. Laparotomy:
- Laparoscopy is the preferred approach in most cases - shorter hospital stay, less blood loss, shorter operative time, fewer adhesions, lower cost
- Laparotomy is indicated for hemodynamic instability, extensive adhesive disease, abdominal pregnancy, or lack of laparoscopic capability
Salpingostomy vs. Salpingectomy:
- Salpingostomy (tube-sparing) - preferred when future fertility is desired and the contralateral tube is damaged
- Salpingectomy - indicated when tube is severely damaged, patient does not desire fertility, or for hemostasis
B. Medical Treatment - Methotrexate (MTX)
Methotrexate is a folic acid analog that inhibits dihydrofolate reductase, preventing DNA synthesis. It targets rapidly dividing trophoblastic tissue. Success rate: 70-95% depending on patient selection. ~35% of ectopic pregnancies are candidates. - Berek & Novak's Gynecology, Textbook of Family Medicine 9e
Absolute Contraindications to MTX:
| Contraindication |
|---|
| Intrauterine pregnancy |
| Hemodynamically unstable patient |
| Ruptured ectopic pregnancy |
| Breastfeeding |
| Immunodeficiency |
| Moderate to severe anemia, leukopenia, or thrombocytopenia |
| Known sensitivity to methotrexate |
| Active pulmonary disease |
| Active peptic ulcer disease |
| Clinically important hepatic or renal dysfunction |
Relative Contraindications:
- Ectopic mass >4 cm on TVUS
- Embryonic cardiac motion detected on TVUS
- β-hCG >5,000 mIU/mL
- Unable to comply with follow-up
- Refusal to accept blood transfusion
Adapted from ASRM Practice Committee Guidelines, 2013 - Berek & Novak's Gynecology
Pre-treatment workup: CBC, blood type & screen, LFTs, electrolytes + creatinine, CXR (if pulmonary history). Repeated at 1 week post-treatment.
MTX Dosing Protocols:
- Single-dose: MTX 50 mg/m² IM on Day 1; monitor β-hCG on Days 4 and 7; if decline <15%, repeat dose
- Two-dose: MTX 50 mg/m² IM on Days 1 and 4; monitor β-hCG on Days 4 and 7
- Multi-dose (with leucovorin rescue): MTX 1 mg/kg IM alternating with leucovorin 0.1 mg/kg on Days 1, 3, 5, 7
Persistent ectopic pregnancy after salpingostomy can be treated with repeat salpingostomy, salpingectomy, or methotrexate. - Berek & Novak's Gynecology
C. Expectant Management
Can be considered in highly selected, asymptomatic patients with:
- Very low and declining β-hCG levels
- No evidence of rupture
- Willingness and ability to comply with close monitoring
Complications
- Rupture - most feared complication; can cause catastrophic hemorrhage, hemodynamic shock, and death. Requires prompt surgical intervention.
- Persistent trophoblastic tissue after salpingostomy
- Future ectopic pregnancy risk is elevated after one episode
- Reduced fertility if tube is lost
Special Scenarios
- Heterotopic pregnancy (IUP + ectopic simultaneously): rare spontaneously (~1:30,000) but more common with ART. An IUP on ultrasound does not exclude a concurrent ectopic.
- Post-hysterectomy: exceedingly rare; only ~27 case reports since 1918 via fistulous tract.
- Post-sterilization: any pregnancy after tubal ligation must be assumed ectopic until proven otherwise.
- Interstitial/cornual ectopic: higher risk of rupture at more advanced gestational age due to the thicker myometrium; often requires special surgical or hysteroscopic management.
Sources: Robbins & Kumar Basic Pathology; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Tintinalli's Emergency Medicine; Berek & Novak's Gynecology; Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.