Give me in details what are the duties of a doctor in medical poisoning.
Duties of a Doctor in a Case of Medical (Suspected) Poisoning
A. Medical Duties - Care and Treatment of the Patient
1. Life-Saving / Resuscitative Measures (ABCD)
- (A) Airway - Open and clean the airway (oral cavity, nostrils) of secretions, vomit, or foreign bodies. Endotracheal intubation may be necessary to protect and secure the airway.
- (B) Breathing - If arterial blood gas cannot be maintained after establishing the airway, supplemental oxygen therapy is given (via ventimask or endotracheal tube).
- (C) Circulation - IV fluid administration may be life-sustaining.
- (D) CNS Depression - Must be corrected. An unconscious patient should be turned to lie on one side (recovery position) to prevent the tongue from blocking the throat and to allow fluid to drain from the mouth.
2. Removal of Unabsorbed Poison from the Body
- Inhaled poisons - Remove patient to fresh air; give artificial respiration and oxygen (6-8 L/min); keep air-passages free from mucus by postural drainage or aspiration; give Nikethamide 2 mL IV if necessary; aminophylline 250-500 mg for severe bronchospasm; diuretics for pulmonary edema.
- Injected poisons (from bite/injection) - Apply a tight ligature immediately above the wound (loosen 1 minute every 10 minutes to prevent gangrene); excise the wound; suck out the poison; neutralize with a suitable chemical; local adrenaline injection for vasoconstriction; immersing the extremity in cold water (10°C) slows absorption.
- Contact poisons - Remove contaminated clothes, contact lenses, and jewelry immediately. Wash skin/wound with water for 30 minutes or neutralize with specific chemical. Irrigate eyes with normal saline for at least 15 minutes.
- Ingested poisons (Gastric Lavage) - Useful within 2 hours of ingestion. Use a stomach tube (Ewald's or Boa's tube), or a soft non-collapsible rubber tube (1 cm diameter, 1.5 m length).
B. Legal Duties - Assisting the Police to Determine the Manner of Death
1. Note Preliminary Particulars
- Age, sex, address
- Date and time of presentation
- Identification marks and other identifying details
2. Confirm Suspicion Before Expressing an Opinion (Suspected Homicidal Poisoning)
- Route of exposure
- Quantity consumed
- Time elapsed since ingestion
- Collect vomit and urine and submit for chemical analysis
- Food - any change in color, taste, or smell of the food or drink
- Other persons affected at the same time
- Condition of the patient
- Explanation offered by the patient for the symptoms
- Statements of other persons present that appear relevant
- Engage nurses of confidence to administer medicine and food themselves
- Allow no one to be with the patient alone
- Maintain detailed records of the patient's condition and treatment given
- Record the number of visits, symptoms and signs observed, and treatment given from time to time
3. After Confirmation of Suspicion
4. Preserve Evidence
- Suspected articles of food, excreta, and stomach washings
- Full or empty bottles, capsules, paper packets, or liquids lying about
- Any recent stains on bedclothes or furniture (if possible)
Non-compliance is punishable under Section 238, BNS (formerly S. 201, I.P.C.) if it is proved that the doctor did this with the intention of protecting the accused.
5. Report Homicidal Poisoning to Police (Mandatory)
- Non-compliance is punishable under S. 176, I.P.C.
6. Suicidal Poisoning - Reporting NOT Mandatory for Private Practitioners
7. Duty When Summoned by Investigating Police Officer
- Concealing information - liable to prosecution under Section 239 and 202, BNS/I.P.C.
- Giving false information - liable to be charged under Section 212, BNS (formerly S. 177, I.P.C.)
8. Government Medical Officer - Special Duty
9. Recording Dying Declaration
10. Death of the Patient
- Should NOT issue a death certificate
- Should inform the police immediately
11. Food Poisoning - Compulsory Notification
Summary Table
| Duty | Category | Key Action |
|---|---|---|
| ABCD resuscitation | Medical | Stabilize airway, breathing, circulation, CNS |
| Remove poison | Medical | By route - inhalation, ingestion, injection, contact |
| Record patient particulars | Legal | Age, sex, time, identification marks |
| Collect samples | Legal | Vomit, urine, stomach wash, food, bottles |
| Hospital transfer | Medical + Legal | Arrange safe environment if refused |
| Preserve evidence | Legal | Food, stains, containers |
| Report homicidal poisoning | Legal (Mandatory) | S. 2(33) BNSS; punishable if not done |
| Suicidal poisoning | Legal (Optional for private) | Not mandatory since BNS removes S. 309 |
| Cooperate with police | Legal (Mandatory) | S. 195 BNSS; false info = criminal offense |
| Dying declaration | Legal | Must be recorded if patient is serious |
| Death - no death certificate | Legal | Inform police; do not certify |
| Food poisoning notification | Legal (Compulsory) | Notify public health authorities |
- The Essentials of Forensic Medicine and Toxicology, 36th edition (2026), pp. 483-484 - primary source with full duties enumerated under Indian law (BNS/BNSS)
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology - compulsory and voluntary duties of a medical practitioner framework
Can you give mea full NIS Schedule in an image form?
India National Immunization Schedule 2024 2025 full UIP vaccines age
https://prod-cdn.preprod.co-vin.in/uwin-prod/pdf/National+Im…
A detailed, clean medical reference chart titled "India National Immunization Schedule (NIS) - Universal Immunization Programme (UIP)" as a vertical table poster with a white background and color-coded sections. The chart has columns: Age, Vaccines Given, Dose, Route, Site. Organized into four color-coded sections: SECTION 1 - PREGNANT WOMEN (light pink header): - Early pregnancy: Td-1 | 0.5 ml | IM | Upper Arm - 4 weeks after Td-1: Td-2 | 0.5 ml | IM | Upper Arm - If vaccinated within 3 years: Td-Booster | 0.5 ml | IM | Upper Arm SECTION 2 - INFANTS (0-1 Year) (light blue header): - At Birth: BCG | 0.1 ml (0.05 ml <1 month) | Intradermal | Left Upper Arm - At Birth: Hepatitis B (Birth dose) | 0.5 ml | IM | Anterolateral mid-thigh - At Birth: OPV-0 (Zero dose) | 2 drops | Oral | Oral - 6 Weeks: bOPV-1, Pentavalent-1, fIPV-1, RVV-1, PCV-1 | 2 drops/0.5 ml/0.1 ml/3 drops/0.5 ml | Oral/IM/ID/Oral/IM - 10 Weeks: bOPV-2, Pentavalent-2, RVV-2 - 14 Weeks: bOPV-3, Pentavalent-3, fIPV-2, RVV-3, PCV-2 - 9-12 Months: MR-1, JE-1*, PCV Booster, fIPV-3, Vitamin A (1st dose) SECTION 3 - CHILDREN (1-17 Years) (light green header): - 16-24 Months: MR-2, JE-2*, DPT Booster-1, bOPV Booster, Vitamin A (2nd dose) - 2-5 Years: Vitamin A every 6 months (doses 3rd-9th) - 5-6 Years: DPT Booster-2 - 10 Years: Td - 16 Years: Td FOOTNOTES at bottom: *JE vaccine only in endemic/selected districts Pentavalent = DPT + HepB + Hib Abbreviations: BCG=Bacillus Calmette-Guerin; bOPV=Bivalent Oral Polio Vaccine; fIPV=Fractional Inactivated Polio Vaccine; RVV=Rotavirus Vaccine; PCV=Pneumococcal Conjugate Vaccine; MR=Measles-Rubella; JE=Japanese Encephalitis; DPT=Diphtheria-Pertussis-Tetanus; Td=Tetanus-Diphtheria Source: Ministry of Health & Family Welfare, Government of India (UIP/NIS) The chart uses bold headers, alternating light gray row shading for readability, a thin border around each cell, and professional medical poster formatting. Font is clean and legible. Include a small syringe icon in the title area.
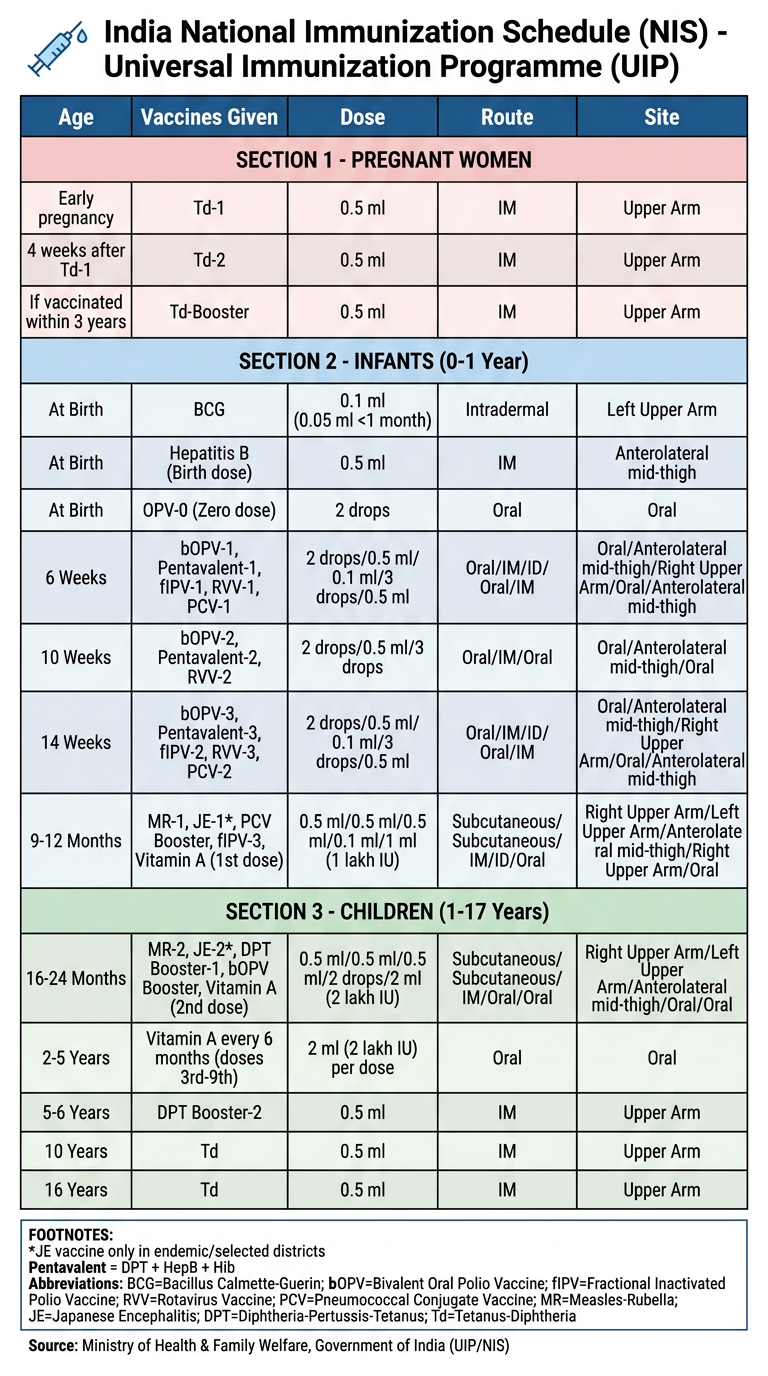
- Td-1 at registration, Td-2 four weeks later, or Td-Booster if previously vaccinated within 3 years.
- Birth: BCG (intradermal, left upper arm), Hepatitis B (IM), OPV-0 (oral)
- 6 Weeks: bOPV-1, Pentavalent-1 (DPT+HepB+Hib), fIPV-1, Rotavirus-1, PCV-1
- 10 Weeks: bOPV-2, Pentavalent-2, Rotavirus-2
- 14 Weeks: bOPV-3, Pentavalent-3, fIPV-2, Rotavirus-3, PCV-2
- 9-12 Months: MR-1, JE-1*, PCV Booster, fIPV-3, Vitamin A 1st dose
- 16-24 Months: MR-2, JE-2*, DPT Booster-1, bOPV Booster, Vitamin A 2nd dose
- 2-5 Years: Vitamin A every 6 months (up to 9th dose)
- 5-6 Years: DPT Booster-2
- 10 Years: Td
- 16 Years: Td