Write a notes on Basic principle on Cardiopulmonary by pass for MD Anaesthesiology exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed from authoritative anaesthesiology textbooks, including two excellent images. Let me now compile the comprehensive MD Anaesthesiology exam notes.
Basic Principles of Cardiopulmonary Bypass (CPB)
Compiled from: Morgan & Mikhail's Clinical Anesthesiology 7e, Barash Clinical Anesthesia 9e, Bailey & Love's Short Practice of Surgery 28e
1. Introduction & Historical Background
Cardiopulmonary bypass (CPB) was first used successfully in 1953 by John Gibbon and has since formed the cornerstone of open cardiac surgery. It allows the surgeon to operate on a still, bloodless heart while artificially maintaining circulation and oxygenation. CPB is used in any procedure requiring temporary cessation of cardiac and pulmonary function - including valve surgery, coronary artery bypass grafting (CABG), repair of congenital heart defects, aortic surgery, and cardiac transplantation.
Alternative uses of CPB (Summary Box):
- Rewarming in accidental hypothermia
- Resuscitation in severe respiratory failure
- Adjunct in pulmonary embolectomy
- Single- and double-lung transplantation
- Resection of highly vascular tumours invading large vessels (e.g. renal tumour invading the IVC)
The operation of a CPB machine is a complex task requiring a certified perfusionist, and optimal results demand close communication and teamwork among surgeon, anaesthesiologist, and perfusionist.
2. The CPB Circuit - Basic Components
The typical CPB machine has six essential components: a venous reservoir, an oxygenator, a heat exchanger, a main pump, an arterial line filter, and the connecting tubing. Modern machines incorporate the reservoir, oxygenator and heat exchanger as a single disposable unit.
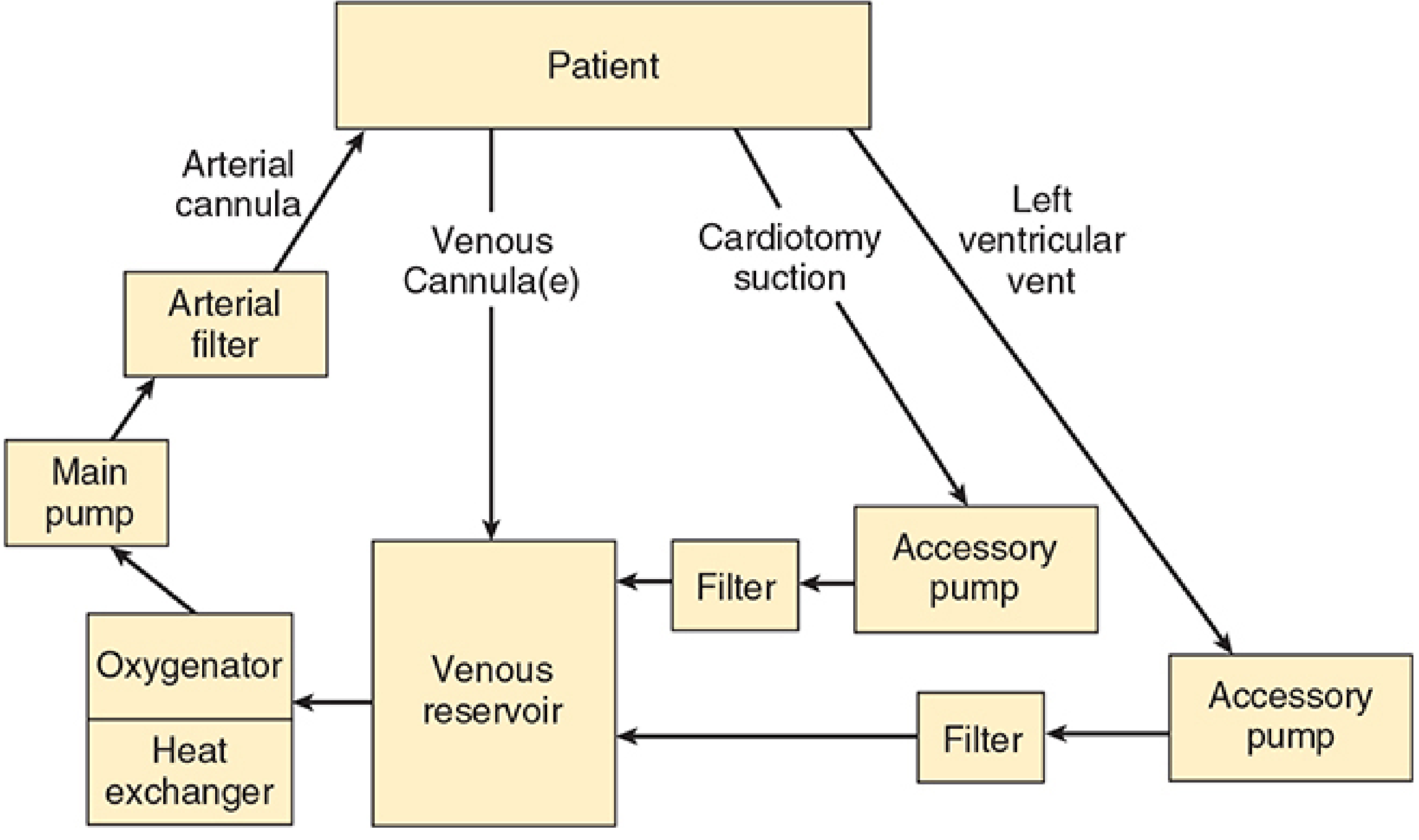
Figure: The basic design of a cardiopulmonary bypass machine (Morgan & Mikhail's Clinical Anesthesiology 7e)
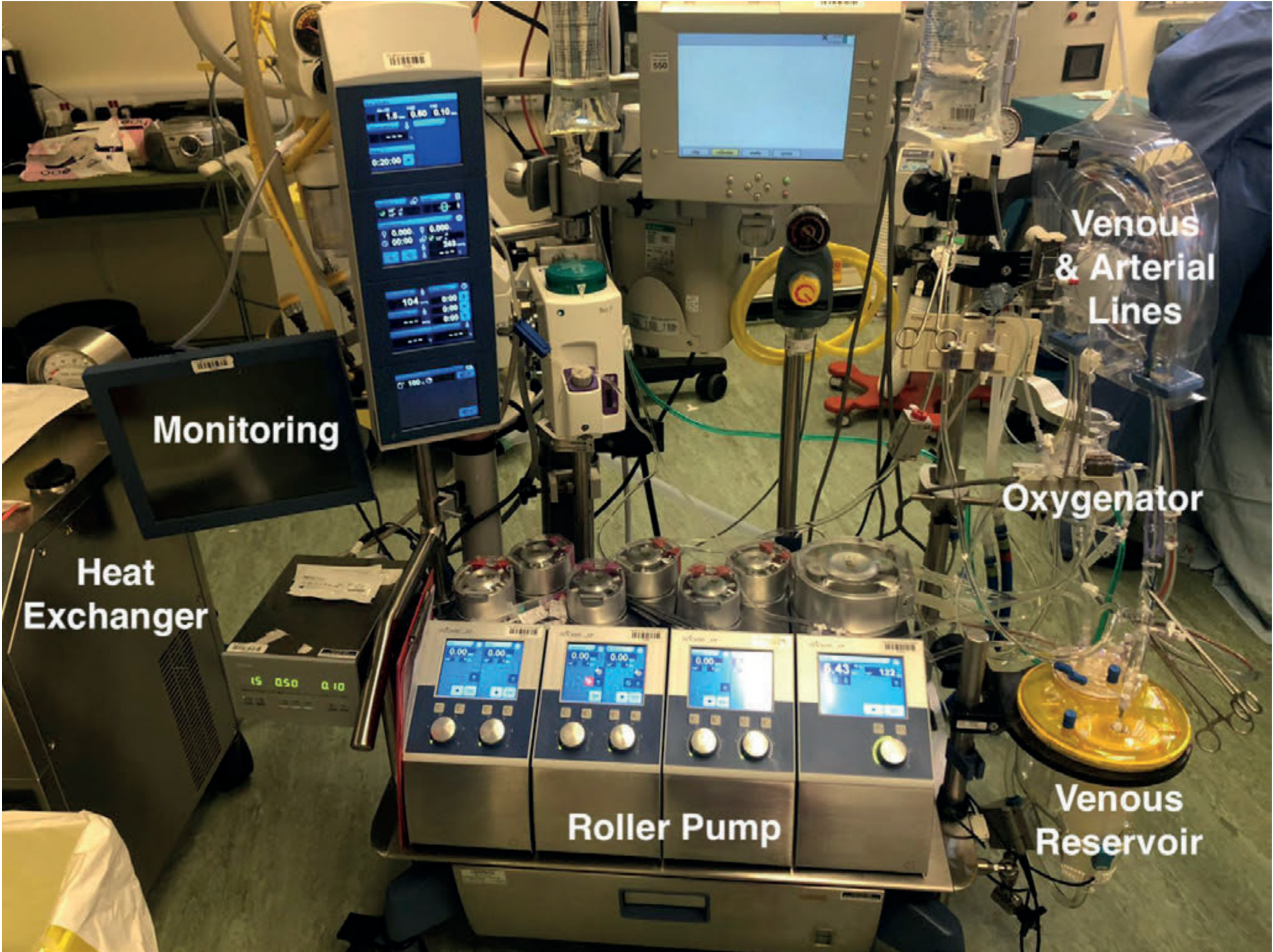
Figure: CPB circuit in use during "on-pump" cardiac surgery (Bailey & Love's 28e)
Flow of blood through the circuit:
- Venous blood drains from patient (via venous cannula in RA/SVC/IVC) by gravity siphon to the venous reservoir
- Blood flows through the oxygenator - CO₂ removed, O₂ added
- Heat exchanger adjusts temperature
- Main pump drives blood forward
- Arterial line filter removes micro-emboli and air
- Oxygenated blood returns to patient via arterial cannula (usually ascending aorta)
2.1 Venous Reservoir
- Receives deoxygenated blood from the venous cannula(e)
- Gravity drainage: reservoir positioned 50-70 cm below the level of the heart
- Acts as a buffer against fluctuations in venous return
- Air lock from entrained air can stop venous flow - a critical hazard
- Reservoir level is critical: if a roller pump runs dry, massive air embolism results (lethal)
- If drainage is inadequate (small cannula), assisted venous drainage using regulated vacuum is used
2.2 Mechanical Pumps
Two types are used:
| Feature | Roller (Occlusive) Pump | Centrifugal Pump |
|---|---|---|
| Mechanism | Compression of tubing | Rotating impeller/cone |
| Flow | Non-pulsatile, constant | Non-pulsatile |
| Risk | Spallation (particle release from tubing) | Less traumatic to blood cells |
| Air embolism risk | High if reservoir empty | Self-limiting (will not pump air) |
| Use | Standard main pump | ECMO, aortic surgery, when anti-air embolism safeguard needed |
Centrifugal pumps are increasingly preferred for the main pump as they are less traumatic to blood elements and will not pump air if the inlet runs dry.
2.3 Oxygenators
Currently, hollow-fibre membrane oxygenators are standard.
- Blood flows on one side of a microporous membrane, gas (O₂/CO₂ mixture) on the other
- Diffusion of O₂ into blood and CO₂ out replicates pulmonary gas exchange
- Older bubble oxygenators (blood directly exposed to gas) are now obsolete due to haemolysis and microemboli
- Membrane oxygenators cause far less blood trauma and inflammatory activation
FiO₂ and sweep gas flow (gas flow rate through the oxygenator) independently control PaO₂ and PaCO₂ respectively during bypass.
2.4 Heat Exchanger
- Allows active cooling and rewarming of the patient's blood
- Water (at controlled temperature) passes through coils in counter-current to blood
- Used to induce systemic hypothermia and to re-warm before weaning from bypass
- Temperature gradient between water and blood must be kept < 10°C to avoid gas coming out of solution (nitrogen emboli)
2.5 Arterial Line Filter
- Positioned between the pump and the arterial cannula
- Removes micro-emboli, air bubbles, and debris from the circuit
- Contains a 20-40 micron screen filter
2.6 Ancillary Components
- Cardiotomy suction pump: returns blood from the operative field to the venous reservoir after filtering
- LV vent: small cannula placed in the LV to drain blood that accumulates (from bronchial venous return, thebesian veins) - prevents LV distension, which impairs myocardial preservation
- Cardioplegia delivery pump: delivers cardioplegic solution to the coronary arteries
3. Cannulation
3.1 Arterial Cannulation
- Standard site: ascending aorta (most physiological, antegrade flow)
- Alternatives (when ascending aorta not suitable):
- Femoral artery - retrograde flow, risk of atheroembolism, limb ischaemia
- Axillary artery - antegrade flow, preferred in aortic dissection, complex aortic surgery; provides selective antegrade cerebral perfusion
- Before cannulation, manual or epiaortic ultrasound inspection rules out severe calcification to reduce stroke risk
- Two purse-string sutures placed, air excluded from cannula before connection
3.2 Venous Cannulation
- Single two-stage cannula (tip in IVC, side holes in RA) - standard for most procedures
- Bicaval cannulation (separate SVC + IVC cannulae) - essential for right heart, tricuspid valve, and atrial surgery
- Alternatively: femoral vein (for minimally invasive or re-do surgery)
- Prerequisite: full systemic heparinisation before cannulation
4. Pump Prime (Priming Solution)
Before use, the entire CPB circuit must be primed with fluid, completely free of bubbles.
- Volume: 1200-1800 mL for adults
- Standard composition: balanced salt solution (lactated Ringer's) is the base; commonly added components include:
- Colloid (albumin or starch) - to maintain oncotic pressure
- Mannitol (0.5 g/kg) - promotes diuresis, free radical scavenger
- Heparin (500-5000 units) - to anticoagulate circuit
- Sodium bicarbonate - buffer
Haemodilution: At onset of bypass in adults using crystalloid prime, hematocrit typically falls to 22-27%. This is generally tolerated and actually has advantages (reduced blood viscosity at hypothermic temperatures, improved microcirculatory flow).
Blood is added to the prime for neonates, small infants, and severely anaemic adults to prevent dangerous haemodilution.
5. Anticoagulation
5.1 Heparin
- Mandatory before cannulation and bypass
- Dose: 300-400 units/kg IV (unfractionated heparin)
- Mechanism: Activates antithrombin III → inhibits thrombin and factor Xa → prevents clot formation within the circuit
5.2 Monitoring - Activated Clotting Time (ACT)
- Baseline ACT: 80-130 seconds (normal)
- Target ACT on CPB: ≥ 400-480 seconds (most centres use ≥ 480 sec)
- ACT is checked every 30-60 minutes during bypass; additional heparin given as needed
- Heparin resistance (due to antithrombin III deficiency, prior heparin use) may require fresh frozen plasma or antithrombin III concentrate
5.3 Heparin Reversal - Protamine
- Given at termination of bypass to reverse heparinisation
- Dose: approximately 1 mg protamine per 100 units heparin given (titrated to ACT)
- Adverse reactions to protamine:
- Hypotension (most common, dose/rate-dependent)
- Anaphylaxis (especially in patients with fish allergy, prior protamine insulin use, or vasectomy)
- Catastrophic pulmonary vasoconstriction (rare but fatal)
- Given slowly (over 10-15 min) via a peripheral vein to minimise reactions
6. Systemic Hypothermia
Hypothermia is one of the most important organ-protective strategies during CPB.
Classification by core temperature:
| Degree | Temperature | Use |
|---|---|---|
| Mild (warm/tepid) bypass | 34-37°C | Simple CABG, short procedures |
| Moderate hypothermia | 28-32°C | Most open cardiac surgery |
| Deep hypothermia | 20-28°C | Complex repairs |
| Profound hypothermia + DHCA | 15-18°C | Neonatal/infant surgery, total aortic arch |
Rationale: Metabolic oxygen requirements are roughly halved for every 10°C reduction in body temperature (Q₁₀ effect). At 18°C, cerebral metabolism is reduced to about 17% of normal, allowing brief periods of circulatory arrest.
Deep Hypothermic Circulatory Arrest (DHCA):
- Core temp cooled to 15-18°C
- Both heart and CPB machine stopped
- Provides a bloodless, motionless field for complex aortic arch repairs and complex congenital heart defects
- Safe arrest duration: up to 60 minutes with good cerebral protection
- Brain protection adjuncts: ice packing around the head, methylprednisolone 30 mg/kg, mannitol 0.5 g/kg
Adverse effects of hypothermia:
- Platelet dysfunction and coagulopathy
- Depression of myocardial contractility
- Increased blood viscosity (mitigated by haemodilution)
- Prolonged drug metabolism (hypothermia reduces hepatic/renal drug elimination)
Rewarming: Via the heat exchanger; patient must be fully rewarmed (nasopharyngeal ≥ 37°C, rectal/bladder ≥ 35°C) before weaning from bypass.
7. Myocardial Protection
7.1 Aortic Cross-Clamping
- Ascending aorta is cross-clamped to completely exclude the coronary arteries
- Heart becomes anoxic - permanent myocardial damage begins within 15-20 minutes
- Cardioplegia arrests the heart and limits ischaemic injury
7.2 Cardioplegia
Definition: A chemical solution delivered to the coronary arteries to arrest myocardial electrical and metabolic activity during aortic cross-clamping.
Key arresting agent: Potassium (high concentration, 15-30 mEq/L) - causes depolarisation of the cardiac myocyte membrane, arresting the heart in diastole (lowest energy state).
Routes of delivery:
| Route | Description | Indication |
|---|---|---|
| Antegrade | Into aortic root or coronary ostia | Standard; ensures even distribution |
| Retrograde | Via coronary sinus cannula | Severe coronary disease, aortic regurgitation, redo surgery |
| Combined antegrade + retrograde | Most complete protection |
Temperature of cardioplegia:
- Cold (4-10°C): Reduces metabolic requirements; standard approach; requires redosing every 15-20 minutes
- Warm (37°C): May improve myocardial recovery by supporting enzymatic function; used for "hot shot" terminal warm cardioplegia
- Blood cardioplegia: Mixes blood with crystalloid solution (4:1 ratio); provides oxygen and buffering; considered superior for longer cross-clamp times
Cardioplegia must be repeated every 15-20 minutes to maintain diastolic arrest and metabolic suppression. Single-dose solutions (e.g. Bretschneider's/HTK solution) are used for longer procedures.
7.3 Topical Hypothermia
- Ice-slush poured around the heart after cross-clamping
- Provides local epicardial cooling to reinforce cardioplegia
7.4 Intermittent Cross-Clamp Fibrillation (ICXF)
- Intermittent ventricular fibrillation (VF) induced during cross-clamping without cardioplegia
- Used for beating-heart valve surgery and some CABG procedures
- Less metabolic protection than cardioplegia
7.5 Myocardial Injury Despite Protection
Myocardial "stunning" (reversible systolic/diastolic dysfunction) is common after CPB. The stunned myocardium responds to inotropes. True necrosis produces irreversible injury.
Risk factors for poor myocardial protection:
- Poor preoperative LV function
- Ventricular hypertrophy
- Diffuse severe coronary artery disease
- Cross-clamp time > 120 minutes
- Total CPB time > 120 minutes
8. Physiological Effects of CPB
CPB creates profoundly non-physiological conditions.
8.1 Haemodynamic Changes
- Non-pulsatile flow (steady state, not pulsatile) - affects peripheral organ perfusion and baroreflex responses
- Mean arterial pressure (MAP) is typically lower than normal on CPB (50-80 mmHg acceptable)
- Flow rate: 2.0-2.4 L/min/m² at normothermia; can be reduced at hypothermic temperatures
8.2 Stress Hormone & Inflammatory Response
CPB initiates a massive systemic inflammatory response:
- Hormone surge: Catecholamines, cortisol, arginine vasopressin (ADH), angiotensin all increase markedly
- Complement activation: Via both the alternate (C3) and classical pathways from blood-artificial surface contact
- Coagulation cascade activated
- Platelet dysfunction: CPB depletes glycoprotein receptors; platelet count falls; platelet function impaired - major cause of post-CPB bleeding
- Leukocyte activation: Neutrophils release proteases and reactive oxygen species
- Kallikrein system and fibrinolysis activated
This inflammatory response can produce a post-CPB systemic inflammatory response syndrome (SIRS) similar to sepsis, potentially leading to multi-organ failure.
Strategies to attenuate the inflammatory response:
- Leukocyte-depleted blood cardioplegia
- Haemofiltration/ultrafiltration (removes inflammatory cytokines - particularly valuable in neonates/infants)
- Systemic corticosteroids (methylprednisolone) - modulate but do not eliminate response
- Miniaturised CPB circuits (reduce surface area of blood-artificial surface contact)
- Heparin-bonded circuits
8.3 Effects on Pharmacokinetics
CPB significantly alters drug behaviour:
- Volume of distribution: Suddenly increases with haemodilution - plasma concentrations of water-soluble drugs (e.g. muscle relaxants) drop abruptly
- Protein binding: Reduced (haemodilution, hypothermia, altered pH, free fatty acids from heparin-activated lipoprotein lipase)
- Drug elimination: Reduced hepatic and renal perfusion lowers drug clearance
- Hypothermia: Slows drug metabolism
- Net result: Lipid-soluble drugs (fentanyl, sufentanil) are relatively well-maintained; water-soluble drugs show marked concentration changes
Clinical implication: Muscle relaxant redosing is often required; opioid plasma concentrations may become unpredictably high during rewarming as sequestered drug is released.
8.4 Renal Effects
- Reduced renal perfusion (non-pulsatile flow, hypotension, low cardiac output)
- Acute kidney injury (AKI) is a common complication
- Maintained urine output (target: 0.5-1 mL/kg/hr during bypass) monitored via urinary catheter
8.5 Neurological Effects
- Cerebral autoregulation may be impaired during CPB
- Acid-base management during hypothermic CPB:
- Alpha-stat: Maintain normal pH/PaCO₂ uncorrected for temperature; preferred in adults (better autoregulation, lower cerebral embolic load)
- pH-stat: Add CO₂ to maintain temperature-corrected pH 7.4; increases CBF, may improve cerebral cooling; preferred in paediatric patients undergoing circulatory arrest
- Monitoring: EEG, NIRS (cerebral oximetry), transcranial Doppler (TCD) may be used; NIRS is increasingly integrated
- Complications: Stroke, post-operative cognitive dysfunction (POCD), delirium
9. Conducting CPB - Sequence of Events
Step 1: Initiation of Bypass
- Heparin given IV, ACT confirmed ≥ 480 seconds
- Arterial and venous cannulation
- Circuit connected; gradual transition to full CPB flow
- Ventilator stopped once full flow established
- Gradual cooling begins if hypothermia planned
Step 2: Maintenance of Bypass
- Full CPB flow (2.0-2.4 L/min/m²)
- Aortic cross-clamp applied; cardioplegia delivered
- Surgeon performs the cardiac procedure
- Anaesthesiologist maintains: ACT, MAP, temperature, gases, anaesthetic depth, urine output
- Cardioplegia repeated every 15-20 min
Step 3: Preparation for Weaning
- Surgical repair completed
- De-airing of cardiac chambers (critical - air embolism is fatal)
- Aortic cross-clamp released; coronary perfusion restored
- Rewarming to normothermia (nasopharyngeal ≥ 37°C)
- Correction of: acidosis, hypokalaemia, hypocalcaemia, Hb
- Heart rhythm established (spontaneous or by defibrillation/pacing)
- Epicardial pacing wires placed
Step 4: Weaning from CPB
- Ventilation restarted
- Venous inflow to pump reservoir gradually reduced
- Heart gradually takes over circulation
- TEE assessment of ventricular function
- Inotropic/vasopressor support initiated as needed
- When haemodynamics acceptable, CPB discontinued
Step 5: Termination of Bypass
- CPB discontinued
- Protamine given to reverse heparin (ACT returns to baseline)
- Cannulae removed
- Haemostasis achieved
10. Complications of CPB
| System | Complication |
|---|---|
| Neurological | Stroke, POCD, delirium, hypoxic brain injury |
| Cardiac | Myocardial stunning, low cardiac output, arrhythmias, tamponade |
| Respiratory | Post-bypass lung injury, ARDS, pleural effusion |
| Renal | AKI (most common organ complication) |
| Haematological | Coagulopathy, DIC, thrombocytopenia, haemolysis, transfusion reactions |
| Inflammatory | Post-CPB SIRS, multi-organ failure |
| Embolic | Air embolism, atheroembolism (fat, thrombus, plaque) |
| Technical | Aortic dissection (from cannulation), oxygenator failure, pump failure, circuit disconnection |
11. Off-Pump Surgery (OPCAB)
Surgery on the beating heart without CPB, using mechanical heart stabilisers. Advantages include avoidance of the inflammatory response, reduced embolic burden, and no haemodilution. Restricted mainly to CABG. Weaning is not required. The anaesthetic management focuses on maintaining haemodynamic stability during cardiac manipulation (heart displacement for posterior vessel access can cause profound hypotension).
12. Paediatric Considerations
- Circuit prime is 3x the infant's blood volume - blood is added to prevent excessive haemodilution
- Higher flow rates required (up to 200 mL/kg/min in neonates)
- MAP during CPB is lower (20-50 mmHg acceptable)
- pH-stat preferred during hypothermic CPB for better cerebral cooling before DHCA
- Intense inflammatory response due to large surface-area-to-blood-volume ratio; corticosteroids and modified ultrafiltration (after bypass) are used
- DHCA (15°C, up to 60 minutes) necessary for complex congenital repairs
- Calcium supplementation more frequently needed than in adults
- Weaning difficulty should prompt TEE evaluation for residual defects
Summary of Key Points for Exam
- First successful CPB: Gibbon, 1953
- Basic components: Venous reservoir → Oxygenator + Heat exchanger → Main pump → Arterial filter → Patient
- Standard arterial cannulation site: Ascending aorta; alternatives - femoral, axillary artery
- Priming volume (adults): 1200-1800 mL; causes haemodilution (Hct 22-27%)
- Heparin dose: 300-400 units/kg; target ACT ≥ 480 sec; reversed with protamine
- Hypothermia rationale: O₂ requirements halved per 10°C; DHCA at 15-18°C allows 60 min arrest
- Cardioplegia: Potassium arrests heart in diastole; cold/warm, blood/crystalloid; antegrade/retrograde; repeat every 15-20 min
- Non-pulsatile flow + hypothermia are major non-physiological aspects of CPB
- Post-CPB SIRS: Complement, coagulation, kallikrein activation → inflammatory cascade
- Alpha-stat for adults; pH-stat for paediatric patients undergoing DHCA
- De-airing before cross-clamp removal is mandatory to prevent air embolism
- Protamine adverse effects: Hypotension, anaphylaxis, pulmonary vasoconstriction
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e (pp. 811-825), Barash Clinical Anesthesia 9e (pp. 3281+), Bailey & Love's Short Practice of Surgery 28e (pp. 966-968)
This is a shared conversation. Sign in to Orris to start your own chat.