Bakers cyst
Reading File
Finding Sources
Searching PubMed
"Baker cyst" OR "popliteal cyst"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Baker's Cyst (Popliteal Cyst):
Baker's Cyst (Popliteal Cyst)
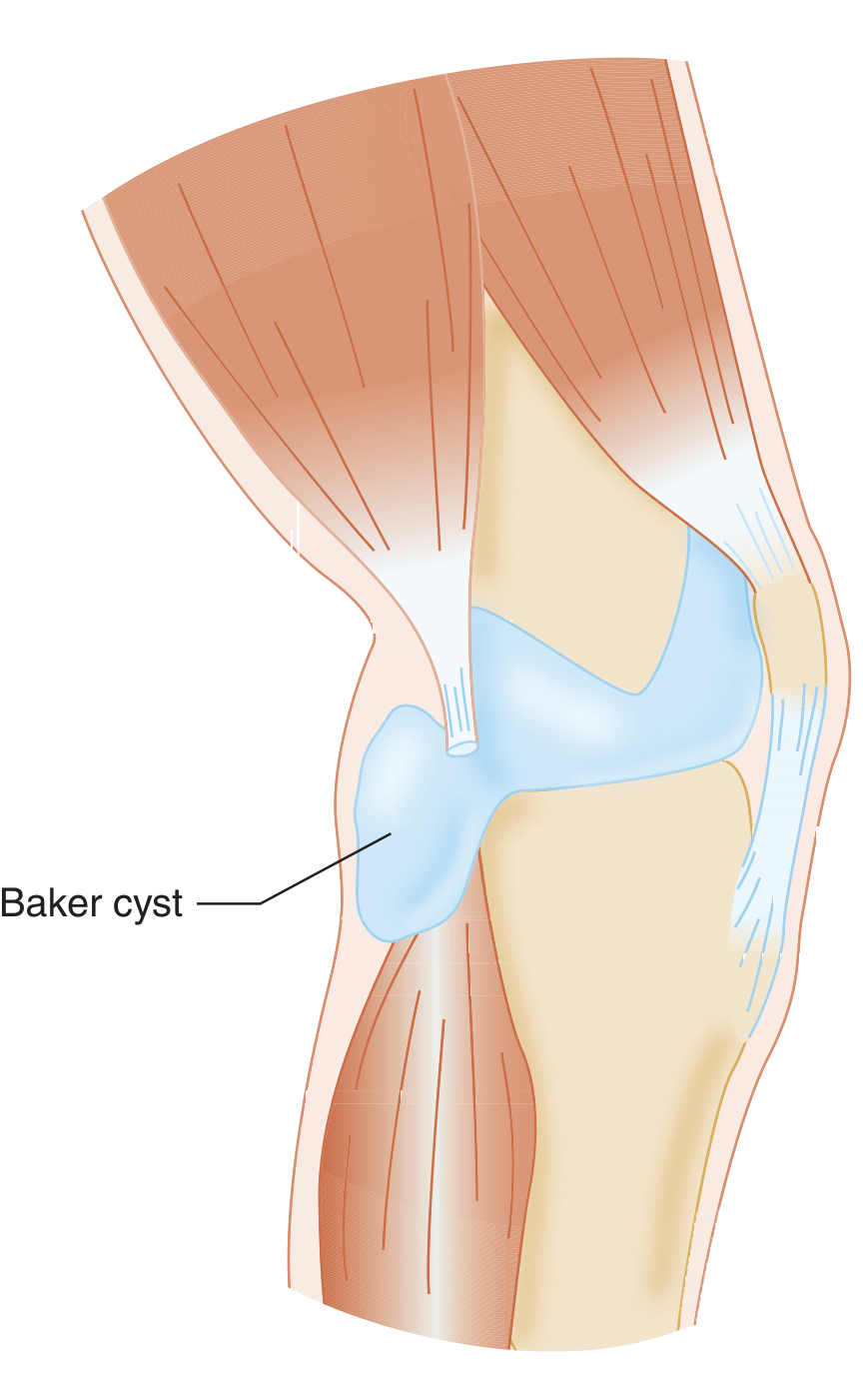
Figure: Baker cyst as an extension of the semimembranosus bursa (Tintinalli's Emergency Medicine)
Definition & Anatomy
A Baker's cyst, first described by Adams in 1840 and later named after Baker (1877), is a distended bursa or herniation of the synovial membrane through the posterior aspect of the knee joint capsule. Multiple bursae exist in the popliteal space, but symptoms develop most often in:
- The bursa beneath the medial head of the gastrocnemius, or
- The semimembranosus bursa (located between the semimembranosus tendon and the medial tibial condyle, and between the semimembranosus tendon and the medial gastrocnemius head)
The cyst typically forms when intra-articular pathology causes excess synovial fluid, which escapes through a normal communication between the bursa and the knee joint - acting like a one-way valve.
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 595
Pathophysiology
- Excess synovial fluid (from any cause) accumulates and pushes through the posterior capsule or through the normal bursal-joint communication
- A valvular mechanism is often present - capsular folds allow fluid to pass from the joint into the cyst but not freely back
- In adults, the cyst almost always communicates with the knee joint; in children, this communication is less common
- Giant synovial cysts extending into the calf are classically associated with rheumatoid arthritis
Causes / Associated Conditions
| Category | Examples |
|---|---|
| Degenerative | Osteoarthritis, degenerative posterior horn medial meniscus tear |
| Inflammatory | Rheumatoid arthritis, other inflammatory arthropathies |
| Mechanical | Meniscal tears (especially posterior horn), chondromalacia patella |
| Traumatic | Post-traumatic effusions |
| Any knee effusion | Gout, pseudogout, infection |
Clinical Features
- Posteromedial popliteal mass - typically soft, fluctuant, and transilluminable
- Pressure, pain, and limitation of knee ROM
- Fullness or tightness behind the knee, worse with activity
Complications
-
Rupture - fluid dissects into the calf, causing sudden calf pain and swelling - can mimic DVT or compartment syndrome ("pseudothrombophlebitis")
-
Acute compartment syndrome (rare, from rupture)
-
Popliteal vein thrombosis - can occur concurrently with a dissecting cyst
-
Spontaneous venous bleeding in patients on anticoagulants (blood dissects into calf)
-
Note: DVT and Baker's cyst can coexist, so DVT must always be excluded
-
Rosen's Emergency Medicine, p. 725
Differential Diagnosis
- DVT / thrombophlebitis
- Popliteal artery aneurysm
- Lipoma
- Xanthoma
- Fibrosarcoma / other soft tissue tumors
- Vascular tumor
- Pyogenic abscess
- Ganglion cyst
Diagnosis
| Modality | Role |
|---|---|
| Transillumination | Simple bedside test - cyst lights up (confirms cystic nature) |
| Ultrasound | First-line - confirms cyst, rules out DVT, guides aspiration; shows anechoic/hypoechoic popliteal mass |
| MRI | Gold standard - confirms cyst AND identifies intra-articular pathology (meniscal tears, OA, etc.); preferred modality |
| Arthrography | Demonstrates communication with the joint; largely replaced by MRI |
| Venous duplex | Excludes concurrent DVT; may identify cyst remnants |
Baker's cyst is a diagnosis of exclusion in the ED - DVT must be ruled out when there is clinical suspicion.
Treatment
Conservative (first-line)
- Relative rest, compression, NSAIDs
- Treat the underlying intra-articular pathology (the cyst is a secondary problem)
- Observation alone is appropriate in children - most resolve spontaneously
Aspiration / Injection
- US-guided aspiration with a large-bore needle, followed by corticosteroid instillation (e.g., methylprednisolone acetate), is effective and safe for symptomatic cysts
- Not recommended in the ED; done on an outpatient basis
Surgical Options (when conservative fails)
| Approach | Details |
|---|---|
| Arthroscopic treatment of intra-articular pathology | Most common - treats the root cause (meniscal debridement, partial meniscectomy, chondral treatment) |
| Arthroscopic cystectomy | Resection of cyst wall + enlarging the articular-cyst communication via posterior portals; best outcomes; recurrence <2% |
| Open cystectomy | Posteromedial (Henderson) incision or posterior incision for large midline cysts; recurrence rate ~40% when done alone |
| Synovectomy | Added for RA-associated giant synovial cysts to prevent recurrence |
Key surgical principles:
-
Arthroscopic cystectomy significantly outperforms open surgery
-
The valvular capsular fold should be resected arthroscopically with a motorized shaver
-
Loose bodies may travel between the joint and cyst - can be retrieved via accessory posteromedial portal
-
Campbell's Operative Orthopaedics 15th Ed 2026, p. 595-596
-
Rheumatology 2-Volume Set (Elsevier 2022)
Key Clinical Pearls
- In adults - always look for intra-articular pathology (most common: degenerative posterior horn medial meniscus tear)
- In children - cysts rarely communicate with the joint, intra-articular pathology is rare, and most resolve with watchful waiting
- A ruptured cyst mimics DVT - but both can coexist, so always do a duplex ultrasound
- Patients on anticoagulants are at risk for hemorrhage into the cyst with calf dissection
- RA patients can develop giant synovial cysts extending deep into the calf - require synovectomy to prevent recurrence
This is a shared conversation. Sign in to Orris to start your own chat.