Origin of bartholin cyst
Reading File
Finding Sources
Finding Sources
Searching the Web
Bartholin cyst origin pathophysiology anatomy
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough answer. Here it is:
Origin of a Bartholin Cyst
The Bartholin Glands - Anatomy
The Bartholin glands (also called the greater vestibular glands) are a pair of small, pea-sized glandular structures located at the 4 o'clock and 8 o'clock positions at the vaginal orifice, within the labia minora. They are normally impalpable in healthy women. Each gland:
- Is lined by cuboidal (mucus-secreting) epithelium
- Has a duct lined by transitional epithelium that drains into the posterior vestibule, just lateral to the hymeneal ring
- Begins functioning at puberty, secreting a mucoid fluid that lubricates the vulva
- Gradually involutes with age (postmenopausal women)
- Tintinalli's Emergency Medicine, p. 2554
How a Bartholin Cyst Forms
A Bartholin cyst arises from obstruction of the excretory duct of the gland. When the duct is blocked, the normal mucoid secretions of the gland have no outlet and gradually accumulate, causing progressive dilation of the duct or gland itself.
The sequence:
- Duct obstruction - caused by inflammation, infection, trauma, or fibrosis/stenosis from prior injury
- Mucous secretion accumulates behind the obstruction
- Cyst formation - the retained secretions distend the duct and gland into a cystic structure
The cyst wall is typically lined by transitional or squamous epithelium (reflecting the native duct lining). Cysts can enlarge to 3-5 cm in diameter, causing pain and local discomfort.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 916
- Schwartz's Principles of Surgery, p. 1819
Causes of Duct Obstruction
The most common underlying triggers:
| Cause | Mechanism |
|---|---|
| Infectious/inflammatory | Vulvitis or STI-related inflammation causes edema and scarring of the duct orifice |
| Gonorrhea / Chlamydia | N. gonorrhoeae causes suppurative infection of the vulvovaginal glands; C. trachomatis also implicated |
| Polymicrobial infection | E. coli is the most common isolate; many cases are polymicrobial |
| Post-trauma / fibrosis | Prior surgery, trauma, or chronic inflammation leads to duct stenosis |
| Thick secretions | Inspissated mucus may plug the duct without overt infection |
- Robbins & Kumar Basic Pathology, p. 287
- Tintinalli's Emergency Medicine, p. 2554
Cyst vs. Abscess
These are two points on the same continuum:
- Bartholin cyst - duct obstruction with sterile or mildly infected accumulated secretion; may be asymptomatic or mildly painful
- Bartholin abscess - secondary infection of the cyst (or direct gland infection without a preceding cyst), resulting in an acutely inflamed, tender, fluctuant mass
A cyst does not need to be present before an abscess can develop - primary abscess can arise directly from gland infection.
Clinical Points
- Most common in reproductive-age women (glands are active from puberty to menopause)
- Usually unilateral
- Benign in the vast majority; however, in women over 40, any solid mass within a Bartholin cyst or abscess warrants biopsy to exclude Bartholin gland carcinoma (which accounts for ~5% of vulvar carcinomas)
- Pfenninger and Fowler's Procedures for Primary Care, p. 3104
- Berek & Novak's Gynecology
Surgical Image
Below is an intraoperative view of a Bartholin cyst opened during marsupialization, showing the cyst cavity after the roof has been removed:
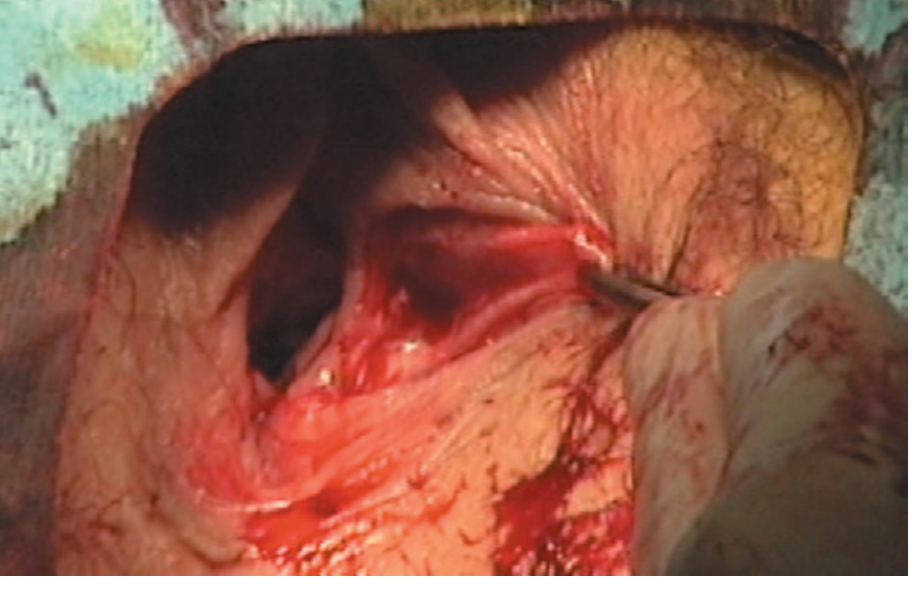
Figure: Bartholin's cyst opened with roof removed - Pfenninger and Fowler's Procedures for Primary Care
Procedure ot notes
Asking for Preferences
Reading File
Reading File
Searching the Web
Bartholin cyst marsupialization operative note dictation template
Reading Web Page
https://www.mtsamplereports.com/bartholins-cyst-marsupializa…
Reading File
I have all the information needed. Here is a complete operative note in standard dictation format:
OPERATIVE NOTE
Marsupialization of Bartholin's Cyst
DATE OF OPERATION: ___________
PREOPERATIVE DIAGNOSIS: Left/Right recurrent Bartholin's duct cyst
POSTOPERATIVE DIAGNOSIS: Left/Right recurrent Bartholin's duct cyst (with abscess formation, if applicable)
PROCEDURE PERFORMED: Marsupialization of left/right Bartholin's cyst (+ biopsy of cyst wall, if sent)
SURGEON: ___________
ASSISTANT: ___________
ANESTHESIA: General / Spinal / Local with IV sedation
ESTIMATED BLOOD LOSS: Negligible
COMPLICATIONS: None
SPECIMENS: Cyst wall biopsy sent to histopathology (if taken)
DRAINS: None
INDICATIONS FOR PROCEDURE
The patient is a ___-year-old female presenting with a symptomatic left/right Bartholin's duct cyst, measuring approximately ___ cm. She gave a history of (prior I&D / Word catheter placement / prior marsupialization - modify as applicable). Conservative management had been attempted/failed. After informed discussion of all available treatment options including risks and benefits, marsupialization was recommended. Consent was obtained and the patient was scheduled for the procedure.
DESCRIPTION OF PROCEDURE
The patient was brought to the operating theatre and placed on the operating table in the dorsal supine position. General/spinal anesthesia was administered without difficulty. The patient was then repositioned in the dorsal lithotomy position. An examination under anesthesia was performed, confirming the presence of a left/right Bartholin's duct cyst measuring approximately ___ x ___ cm at the ___-o'clock position of the posterior introitus. No other vulvar lesions were noted. Bimanual examination was otherwise unremarkable.
The perineum was prepped and draped in the usual sterile fashion with povidone-iodine solution.
The labium was retracted laterally to expose the cyst. The incision site was infiltrated with 2% lidocaine with epinephrine for local hemostasis. (If general anesthesia alone: "No additional local anesthetic was required.")
A fusiform/elliptical incision approximately 1.5-2 cm in length was made on the vaginal mucosal surface, internal to/just lateral to the hymenal ring, longitudinal with respect to the vagina, over the point of maximal fluctuation of the cyst. Care was taken to avoid excising any portion of the external skin.
The mucosa overlying the cyst was excised first. The cyst wall was grasped with two small hemostats before the segment was removed. The incision was extended to approximately ___ cm. On entering the cyst cavity, (clear mucoid / turbid / purulent / chocolate-colored) fluid was noted to drain freely. Cultures were obtained and sent to microbiology.
The cyst cavity was copiously irrigated with sterile normal saline via an Asepto syringe. The cavity was explored with small hemostats; no loculations were identified. The cyst wall was inspected - no neoplastic-appearing epithelium was identified. (If >40 years: "In view of the patient's age, a biopsy of the cyst wall was taken and sent for histopathological examination.")
Marsupialization was then performed by approximating the cut edge of the cyst wall to the adjacent edge of the vaginal mucosa using interrupted 3-0/4-0 Vicryl sutures placed approximately 0.5 cm apart around the excisional margins. This effectively sutures the cyst cavity open, allowing epithelialization of a new permanent opening. Good eversion of the cyst wall was confirmed.
Hemostasis was achieved. The wound was re-irrigated with normal saline. There was a gap of at least 1 cm across the open marsupialization site confirming adequate opening.
Sterile gauze packing was removed from the vagina. All instruments and sponge counts were confirmed correct. No further procedures were performed.
The patient was repositioned to the dorsal supine position and recovered from anesthesia without difficulty. She was transferred to the recovery unit in stable and satisfactory condition.
POST-OPERATIVE INSTRUCTIONS
- Sitz baths twice daily for 3-4 days
- Oral analgesics as needed
- Broad-spectrum antibiotics if abscess confirmed: (e.g., Amoxicillin-Clavulanate / Co-trimoxazole + Metronidazole - as per local protocol and culture sensitivity)
- Follow-up in 1 week
- Return immediately if fever, increasing pain, or purulent discharge
KEY POINTS / SURGICAL NOTES (for junior reference)
| Step | Key Point |
|---|---|
| Position | Dorsal lithotomy |
| Incision site | Mucosal surface, inside/lateral to hymenal ring, never through external skin |
| Incision size | 1.5-2 cm fusiform - must be wide enough to prevent premature closure |
| Cyst wall | Excise mucosa first, grasp wall with hemostats before removing |
| Irrigation | Copious normal saline |
| Sutures | 3-0 or 4-0 Vicryl, interrupted, cyst wall to vaginal mucosa edge |
| Biopsy | Mandatory if patient >40 years to exclude carcinoma |
| Final check | Confirm >1 cm opening remains after suturing |
Sources: Pfenninger and Fowler's Procedures for Primary Care (3rd ed.), p. 922; MT Sample Reports - Bartholin's Cyst Marsupialization Operative Report
This is a shared conversation. Sign in to Orris to start your own chat.