Vibrant soundbridge. Ms ent university exam pattern for 10 marks.
Reading File
Searching the Web
Vibrant Soundbridge MS ENT exam answer 10 marks components indications
Finding Sources
Reading Web Page
Vibrant Soundbridge components indications contraindications results surgical technique
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive 10-mark university exam answer. Here it is:
Vibrant Soundbridge - 10 Mark Answer (MS ENT)
Definition / Introduction
The Vibrant Soundbridge (VSB) is a semi-implantable, active middle ear hearing device manufactured by MED-EL GmbH (Innsbruck, Austria). It was the first commercially available, FDA-approved middle ear implant - approved in Europe in 1998 and in the United States in 2000. It was originally developed by Symphonix Corporation and introduced in 1997. Over 8,000 patients have been implanted worldwide.
(Cummings Otolaryngology, p. 3055; Shambaugh Surgery of the Ear, p. 574)
Components
The VSB has two main parts:
1. External Component - Audio Processor (AP)
Worn behind the ear (BTE). Contains:
- Microphone
- Audio processing electronics
- Magnet (for transcutaneous coupling)
- Telemetry transmission equipment
- Standard 675 zinc battery
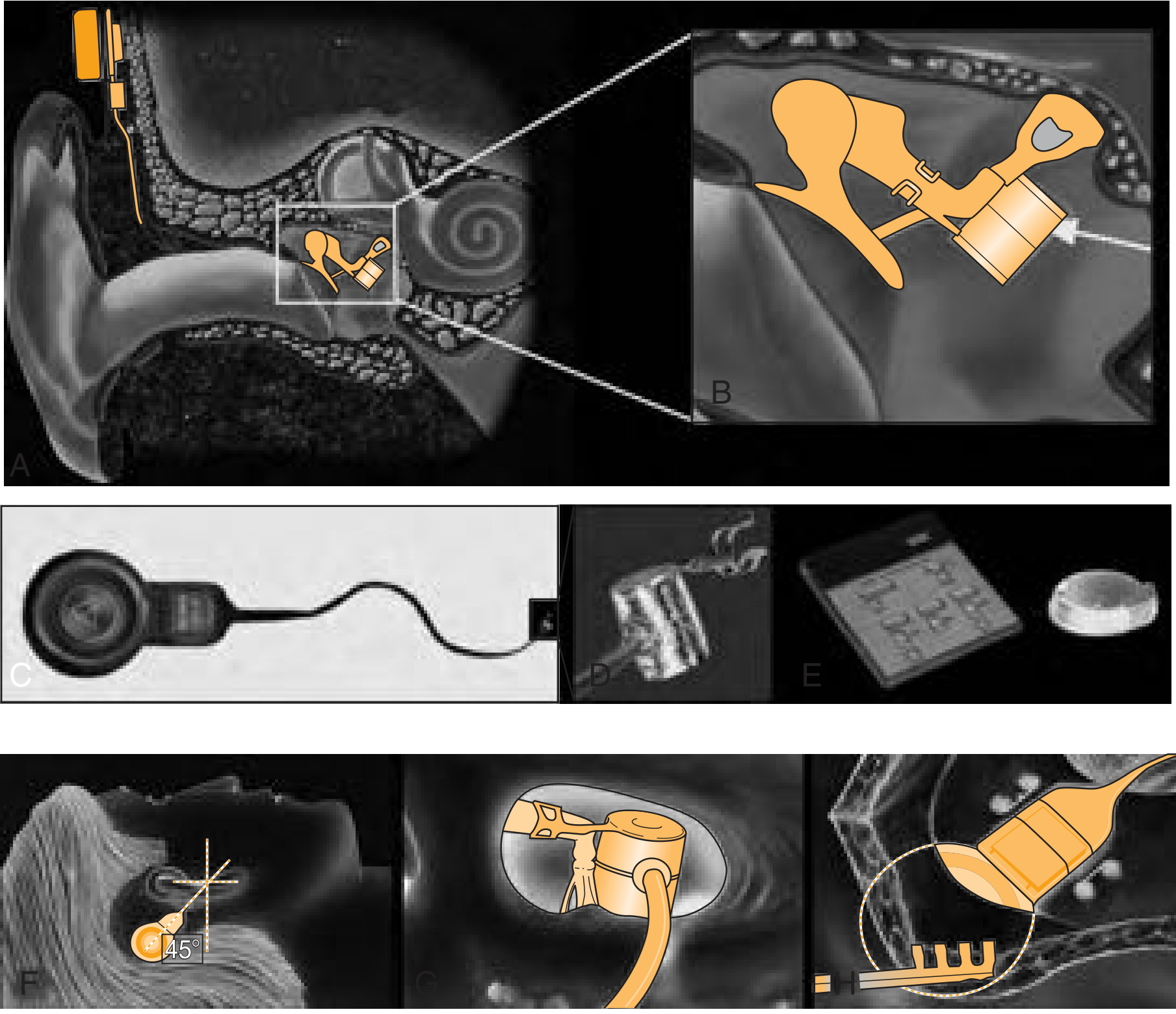
2. Internal Component - Vibrating Ossicular Reconstruction Prosthesis (VORP)
This is the key active implanted unit. It consists of:
| Sub-component | Function |
|---|---|
| Internal receiver/coil | Receives signal transcutaneously from the AP |
| Demodulator | Safety circuit that limits maximum power output and prevents overstimulation |
| Conductor link | Thin signal wire connecting receiver to FMT |
| Floating Mass Transducer (FMT) | The active vibrating element; contains a magnet surrounded by a coil |
| Titanium clip | Attaches FMT to the long process of the incus |
Working Principle / Mechanism
- Sound is picked up by the microphone in the external audio processor.
- The AP processes the signal and transmits it via an inductive transcutaneous telemetry link to the internal receiver - similar to a cochlear implant.
- The signal passes to the demodulator, which generates a current encoding the sound.
- This current travels to the FMT, where electromagnetic induction between the coil and the magnet causes the FMT to vibrate.
- Since the FMT is firmly clipped to the long process of the incus, these vibrations are transmitted directly to the ossicular chain and then to the cochlea.
- This bypasses the outer ear and tympanic membrane entirely, eliminating occlusion and feedback problems seen with conventional hearing aids.
Indications (Audiologic Selection Criteria)
Standard (FDA-approved) indication:
- Moderate to severe sensorineural hearing loss (SNHL) - pure tone average (PTA) up to 70 dB HL
- Normal middle ear anatomy
- Word recognition score ≥ 50% using recorded material
- Absence of retrocochlear or central auditory involvement
- Patient age ≥ 18 years
- Medical contraindication or intolerance to conventional hearing aids (e.g., recurrent otitis externa, canal atresia, chronic skin reactions)
Extended indications (beyond FDA approval):
- Mixed hearing loss (otosclerosis, ossicular erosion/agenesis) - via VORP placement on stapes superstructure, oval window, or round window
- Conductive hearing loss
Contraindications
- Age < 18 years (pediatric use not FDA-approved at initial approval)
- Retrocochlear pathology (acoustic neuroma, central auditory processing disorder)
- Active middle ear disease
- Word recognition < 50%
- Hearing loss beyond 70 dB PTA (may require cochlear implant instead)
Surgical Technique
- Standard transmastoid, facial recess approach to the middle ear
- The internal receiver is placed in a bony trough drilled in the retromastoid/retrosigmoid bone behind the ear (similar to cochlear implant placement)
- The VORP is crimped onto the long process of the incus (crimping force must balance maximal vibration coupling against risk of incus ischemia and necrosis - same principle as stapedectomy)
- For mixed hearing loss: VORP may be placed on the stapes superstructure, oval window, or round window
Advantages Over Conventional Hearing Aids
| Feature | VSB | Conventional HA |
|---|---|---|
| Occlusion effect | None | Common |
| Feedback | None | Common |
| Sound quality | Superior (direct ossicular drive) | Limited |
| Cosmesis | Better (BTE processor only) | Variable |
| Patient satisfaction | Higher | Lower |
Clinical Results
- Phase III trial (53 patients): Statistically significant improvement in functional gain at all frequencies (250-8000 Hz), PHAP, and HDSS scores vs. conventional hearing aids
- Improvement >10 dB noted at 2, 4, and 6 kHz
- Implantation caused <10 dB residual hearing change in 96% of subjects
- Long-term multicenter data (97 patients, 5-8 year follow-up): 72% would repeat the procedure; ~40% interested in binaural implantation
- Device failure rate: 0.3% (post-1999 design); revision surgery needed in 5% due to fibrosis, malpositioning, or inadequate fixation
- Common side effects: persistent aural fullness (27%), taste alteration/dysgeusia (8%)
MRI Compatibility
Because the VORP contains a magnetic component, early models were contraindicated for MRI. The newer VORP 503 model is approved for 1.5T MRI but not for 3T scanners.
Summary Points for Exam
- Semi-implantable, active middle ear device (not fully implantable)
- Key component = FMT (Floating Mass Transducer) - distinguishes it from passive prostheses
- Indication: moderate-severe SNHL, PTA up to 70 dB
- Approach: transmastoid, facial recess
- VORP clipped to long process of incus (standard); alternatives - stapes, RW, OW
- No occlusion, no feedback - key advantages
- First FDA-approved middle ear implant (2000)
- MRI: 1.5T allowed (VORP 503), not 3T
Sources: Cummings Otolaryngology Head and Neck Surgery, p. 3055-3056; Shambaugh Surgery of the Ear, p. 574-575
This is a shared conversation. Sign in to Orris to start your own chat.