Inverted papilloma name reason
Reading File
Finding Sources
Reading File
Here is the complete, textbook-confirmed explanation:
Why Is It Called "Inverted" Papilloma?
The name comes directly from its histological growth pattern - specifically the direction in which the epithelium grows.
Normal papilloma vs. inverted papilloma
- A typical (exophytic) papilloma grows outward from the surface, projecting finger-like fronds above the mucosal surface into the lumen.
- An inverted papilloma does the opposite - the epithelium turns inward and proliferates downward into the underlying stroma, rather than outward.
As described in Cummings Otolaryngology:
"Inverted papilloma is composed exclusively or almost exclusively of hyperplastic ribbons of basement membrane-enclosed epithelium that grow downward into the underlying stroma."
The epithelium is still multilayered (squamous or ciliated columnar cells with mucocytes), but instead of evaginating outward, it invaginates inward - hence the term "inverted."
In simple terms:
| Feature | Exophytic Papilloma | Inverted Papilloma |
|---|---|---|
| Epithelial growth direction | Outward (toward lumen) | Inward (into stroma) |
| Gross appearance | Warty, projecting mass | Smooth surface, bulk is submucosal |
| Histology | Exophytic fronds | Endophytic nests/ribbons into stroma |
Clinical significance of knowing the name
The "inverted" architecture is not just a naming curiosity - it has real implications:
- Higher tendency for local aggression and bone destruction
- High recurrence rate after surgery
- Risk of malignant transformation (5-15% of cases, mostly to squamous cell carcinoma)
- Most common in the lateral nasal wall and maxillary sinus, predominantly in men in the 5th-6th decade
So the name "inverted" is purely descriptive of the microscopic behavior: the epithelium grows into the tissue rather than out of it.
- Cummings Otolaryngology Head and Neck Surgery, p. 985
How to differentiate from polyp
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Here is a full comparison across all key differentiating parameters:
Inverted Papilloma vs. Nasal Polyp - How to Differentiate
1. Laterality (Most Important Clue)
| Inverted Papilloma | Nasal Polyp | |
|---|---|---|
| Side affected | Unilateral (almost always) | Usually bilateral |
Unilateral nasal mass should always raise suspicion for inverted papilloma (or malignancy) rather than simple inflammatory polyp. As Goldman-Cecil Medicine states: "Unilateral nasal polyposis is suggestive of an antral choanal polyp, malignancy, inverted papilloma, or allergic fungal sinusitis; early biopsy is recommended."
2. Clinical/Endoscopic Features
| Feature | Inverted Papilloma | Nasal Polyp |
|---|---|---|
| Appearance | Pale/pink, papillary or cerebriform (brain-like) surface | Smooth, glistening, translucent ("grape-like") |
| Surface texture | Irregular, lobulated | Smooth |
| Consistency | Firm | Soft, compressible |
| Bleeding | More prone to bleeding on touch | Less vascular |
| Origin | Lateral nasal wall / middle meatus | Ethmoid sinuses (bilateral), evenly distributed |
| Association | No allergy/asthma association | Strongly associated with allergic rhinitis, asthma, aspirin sensitivity (Samter's triad) |
From Cummings Otolaryngology: "Nasal endoscopy typically shows a pale, polypoid mass with a papillary or cerebriform appearance protruding from the middle meatus, which strongly suggests the nature of the lesion."
3. Imaging (CT and MRI)
| Feature | Inverted Papilloma | Nasal Polyp |
|---|---|---|
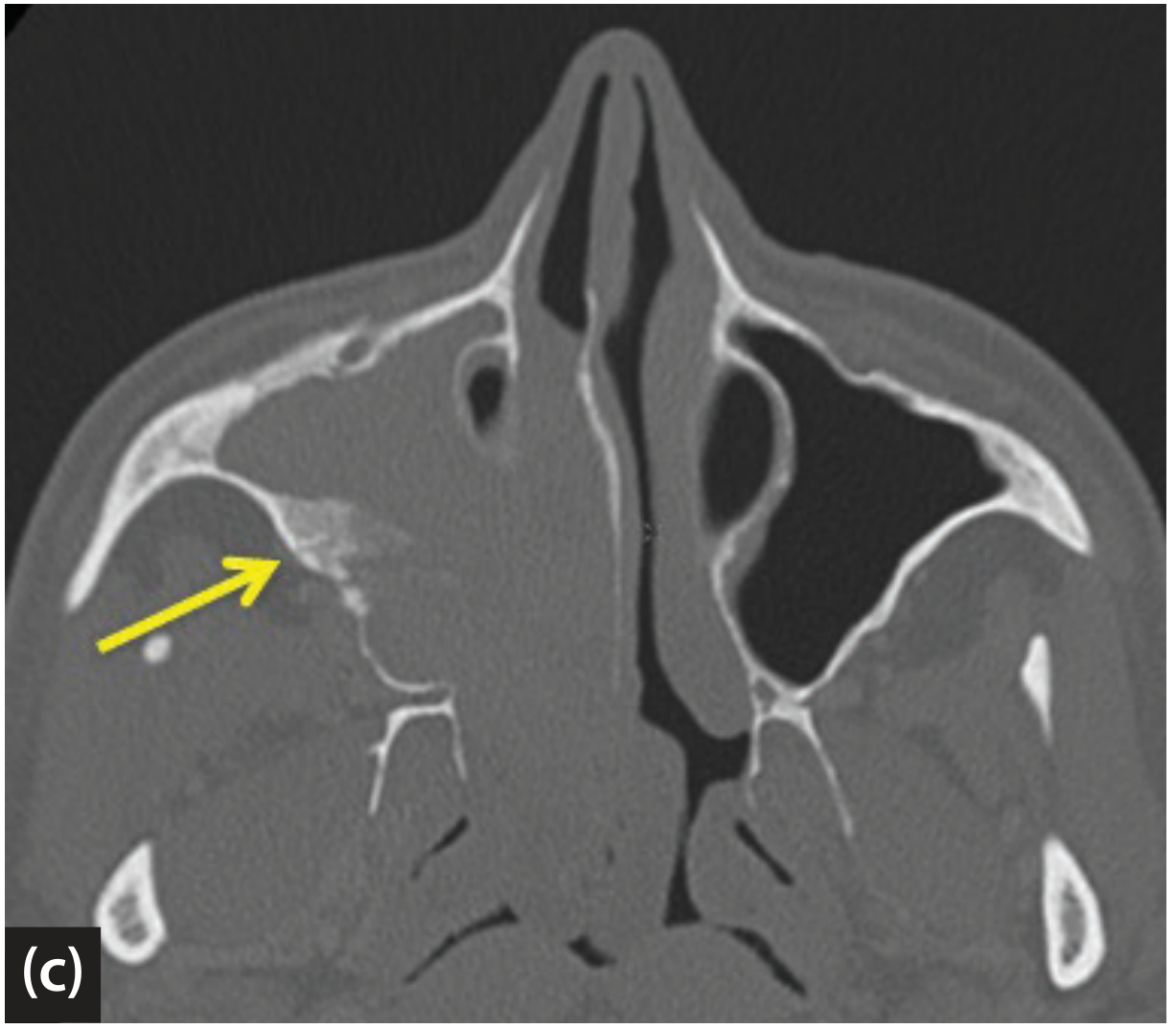
| CT finding | Focal hyperostosis at site of origin; bony remodeling | No hyperostosis; bony thinning/erosion from pressure only |
| MRI - T2 signal | Cerebriform/columnar striated pattern (alternating hypointense and hyperintense bands) | Homogeneously hyperintense (mucus-like) |
| MRI - enhancement | Heterogeneous enhancement | Peripheral or no enhancement |
The cerebriform (striated) pattern on MRI is the most specific radiological sign of inverted papilloma. From Cummings: "The so-called cerebriform-columnar pattern, which is highly predictive of inverted papilloma, can be easily detected by MRI. This radiologic finding reflects the histologic arrangement characterized by the alternation of regular parallel folds made of a highly cellular metaplastic epithelium and an underlying less cellular stroma."

4. Histology (Gold Standard)
| Feature | Inverted Papilloma | Nasal Polyp |
|---|---|---|
| Epithelium | Hyperplastic ribbons invaginating into stroma | Respiratory epithelium (normal thickness) |
| Stroma | Fibrous with infiltrating epithelial nests | Edematous stroma with eosinophils, plasma cells |
| Mucocytes | Present within epithelial ribbons | Sparse |
| Basement membrane | Intact but epithelium inverts through it | Intact, epithelium stays on surface |
| Malignancy risk | 5-15% transformation to SCC | Nil |
5. Behavior
| Inverted Papilloma | Nasal Polyp | |
|---|---|---|
| Recurrence | High (requires complete surgical excision) | Recurs but responds to steroids |
| Malignant transformation | Yes (5-15%) | No |
| Treatment | Surgery (endoscopic or external) | Intranasal steroids, surgery for refractory cases |
| Response to steroids | No | Yes (characteristic shrinkage) |
Summary: The Red Flags for Inverted Papilloma over Polyp
- Unilateral mass
- Irregular/cerebriform surface on endoscopy
- No response to steroids
- Focal hyperostosis on CT
- Cerebriform striated pattern on MRI
- Biopsy - always definitive
Biopsy is mandatory whenever inverted papilloma is suspected, as it is the only way to confirm the diagnosis and rule out synchronous malignancy.
- Cummings Otolaryngology Head and Neck Surgery, p. 985-986; Scott-Brown's Otorhinolaryngology Vol 1, p. 5547; Goldman-Cecil Medicine
How to read a nasopharyngeal xray
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Now I have comprehensive textbook material. Here is the full guide:
How to Read a Nasopharyngeal X-ray (Lateral Soft Tissue Neck View)
The standard view used to assess the nasopharynx is the lateral soft tissue radiograph of the neck/nasopharynx. This is the most clinically useful plain film view for this region.
Step 1 - Technical Adequacy (Before Reading)
Before interpreting, check:
- Position: Patient must be upright, neck extended, during full inspiration
- This is critical - if the neck is flexed or film taken during expiration, the retropharyngeal soft tissues bulge anteriorly and mimic a retropharyngeal abscess (called a "pseudoretropharyngeal mass")
- Projection: True lateral (no rotation)
- Exposure: Soft tissue technique (low kV) to distinguish air, soft tissue, and bone interfaces
Step 2 - Identify the Key Anatomical Landmarks (Top to Bottom)
On a lateral nasopharyngeal X-ray, you should identify:
| Structure | What to Look For |
|---|---|
| Hard palate | Horizontal bony line at top - roof of the oral cavity |
| Soft palate | Soft tissue continuation posteriorly from hard palate |
| Adenoid pad | Soft tissue mass on the posterior-superior wall of nasopharynx |
| Nasopharyngeal airway | Black (air-filled) space between adenoid and soft palate |
| Posterior pharyngeal wall | Smooth soft tissue column running vertically |
| Retropharyngeal space | Thin space between posterior pharyngeal wall and cervical spine (should be narrow) |
| Cervical vertebrae | Bony column posteriorly (C1-C4 usually visible) |
| Epiglottis | Leaf-shaped structure at base of tongue |
Step 3 - Assess the Adenoid (Primary Purpose of the Film)
This X-ray is mainly used in children to assess adenoid size when endoscopy is not tolerated.
The Adenoidal-Nasopharyngeal (A/N) Ratio:
Draw two lines:
- A = thickness of the adenoid shadow (from its anterior face to the posterior nasopharyngeal wall)
- N = total nasopharyngeal width (from the posterior edge of the hard palate to the anterior surface of the cervical spine, at the same level)
| A/N Ratio | Interpretation |
|---|---|
| < 0.6 | Normal |
| 0.6 - 0.7 | Borderline |
| > 0.7 | Significant adenoid hypertrophy |
| > 0.8 | Severe obstruction |
As Cummings states: "Adenoidal size can be evaluated subjectively, but objective methods of assessing adenoidal size using an adenoidal:nasopharyngeal ratio have been described."
Step 4 - Assess the Soft Tissue Shadows Systematically
A. Posterior Pharyngeal / Retropharyngeal Space:
- At C2 level: should be < 7 mm in adults and children
- At C6 level: should be < 14 mm in children, < 22 mm in adults
- Widening suggests retropharyngeal abscess, hematoma, or tumor
B. Nasopharyngeal Airway Column:
- Should be a clear, unobstructed black air column
- Narrowing = adenoid hypertrophy, mass, or choanal stenosis
C. Soft Palate:
- Should be a thin, smooth soft tissue structure
- Thickening or displacement is abnormal
Step 5 - What the Lateral View Identifies Specifically
From Cummings Otolaryngology: "The lateral radiograph is useful in evaluating the tongue, adenoids, tonsils, epiglottis, aryepiglottic folds, piriform sinuses, laryngeal ventricle, and subglottic trachea."
Specific pathologies visible:
| Finding | Diagnosis |
|---|---|
| Adenoid pad obliterating nasopharyngeal airway | Adenoid hypertrophy |
| Soft tissue mass in nasopharynx | Nasopharyngeal carcinoma, angiofibroma, polyp |
| Widened retropharyngeal space | Retropharyngeal abscess / cellulitis |
| Rounded, thumb-like epiglottis | Epiglottitis ("thumb sign") |
| Narrowed subglottis ("steeple sign") | Croup |
| Radiopaque foreign body | Ingested/inhaled foreign body |
Step 6 - Limitations to Know
- A plain nasopharyngeal X-ray is neither sensitive nor specific for nasopharyngeal tumors (e.g. NPC) and has been superseded by CT and MRI for that purpose - Scott-Brown's states plainly: "A plain radiograph of the nasopharynx is neither sensitive nor specific enough for any clinical use and has been superseded by other modalities."
- Main clinical value today = assessing adenoid size in children when endoscopy is not feasible, and screening for foreign bodies
- For any suspected tumor, abscess, or vascular lesion, CT or MRI is the investigation of choice
Summary: Reading Order
- Check technical quality (position, inspiration, neck extension)
- Identify bony landmarks (hard palate, cervical spine)
- Trace the nasopharyngeal airway column
- Assess adenoid pad size - calculate A/N ratio if needed
- Measure retropharyngeal space
- Look for masses, foreign bodies, calcifications
- Assess epiglottis and subglottis below
- Cummings Otolaryngology Head and Neck Surgery, p. 1955-1957; Scott-Brown's Otorhinolaryngology Vol 2, p. 331
This is a shared conversation. Sign in to Orris to start your own chat.