Proliferative vitroretinopathy
Reading File
Finding Sources
Searching PubMed
proliferative vitreoretinopathy
Reading File
Searching Images
proliferative vitreoretinopathy retinal detachment
Reading File
Reading File
Reading File
I now have comprehensive content from Kanski's Clinical Ophthalmology. Here is the full structured answer:
Proliferative Vitreoretinopathy (PVR)
Definition & Pathogenesis
PVR is caused by epiretinal and subretinal membrane formation, with contraction of these membranes leading to tangential retinal traction and fixed retinal fold formation. The membranes arise from retinal pigment epithelial (RPE) cells, glial cells, and macrophages that migrate, proliferate, and undergo fibroblastic transformation on retinal surfaces.
Typical settings:
- Following surgery for rhegmatogenous retinal detachment (RD) — the most common context
- After penetrating ocular injury
- In eyes with rhegmatogenous RD that have had no prior retinal surgery
The main clinical hallmarks are retinal folds and retinal rigidity — decreased mobility during eye movements or scleral indentation.
Classification (Grading)
Progression from one stage to the next is not inevitable.
| Grade | Severity | Features |
|---|---|---|
| A | Minimal | Diffuse vitreous haze; tobacco dust; pigmented clumps on inferior retinal surface |
| B | Moderate | Wrinkling of inner retinal surface; decreased vitreous gel mobility; rolled edges of retinal breaks; tortuous vessels; retinal stiffness |
| C | Marked | Rigid, full-thickness retinal folds (often star-shaped); heavy vitreous condensation and strands |
Grade C is further subdivided:
- C-A (anterior) — proliferation anterior to the equator
- C-P (posterior) — proliferation posterior to the equator
Severity within each zone is expressed as the number of clock hours of retina involved.
Advanced disease shows gross reduction of retinal mobility with retinal shortening and a characteristic funnel-like triangular conformation.
Development of PVR
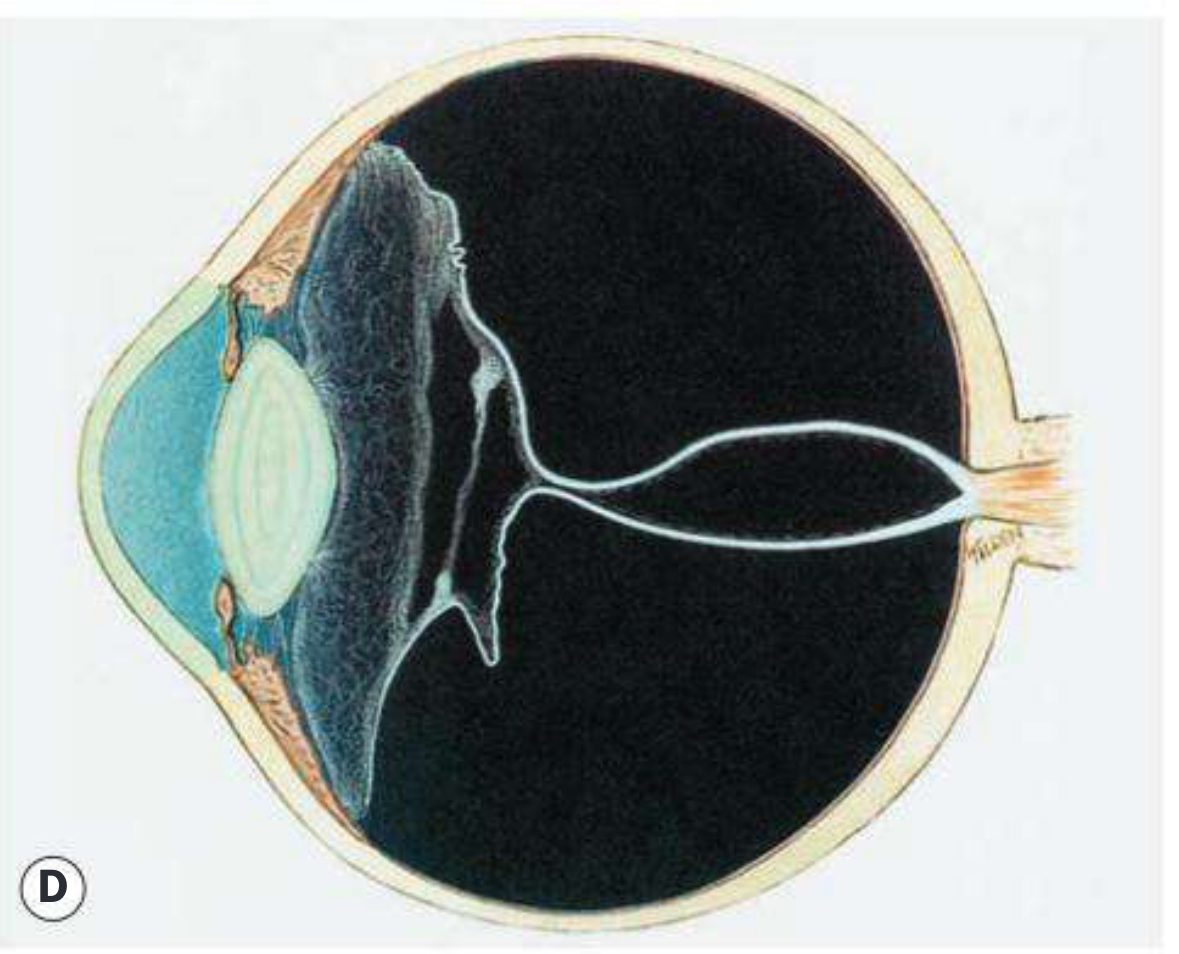
Fig. 16.24 Development of PVR. (A) Extensive vitreous syneresis; (B) total retinal detachment without PVR; (C) early PVR with anteriorly retracted vitreous gel and equatorial circumferential retinal folds; (D) advanced PVR with a funnel-like retinal detachment bridged by dense vitreous membranes. — Kanski's Clinical Ophthalmology 10th ed.
Clinical Appearance
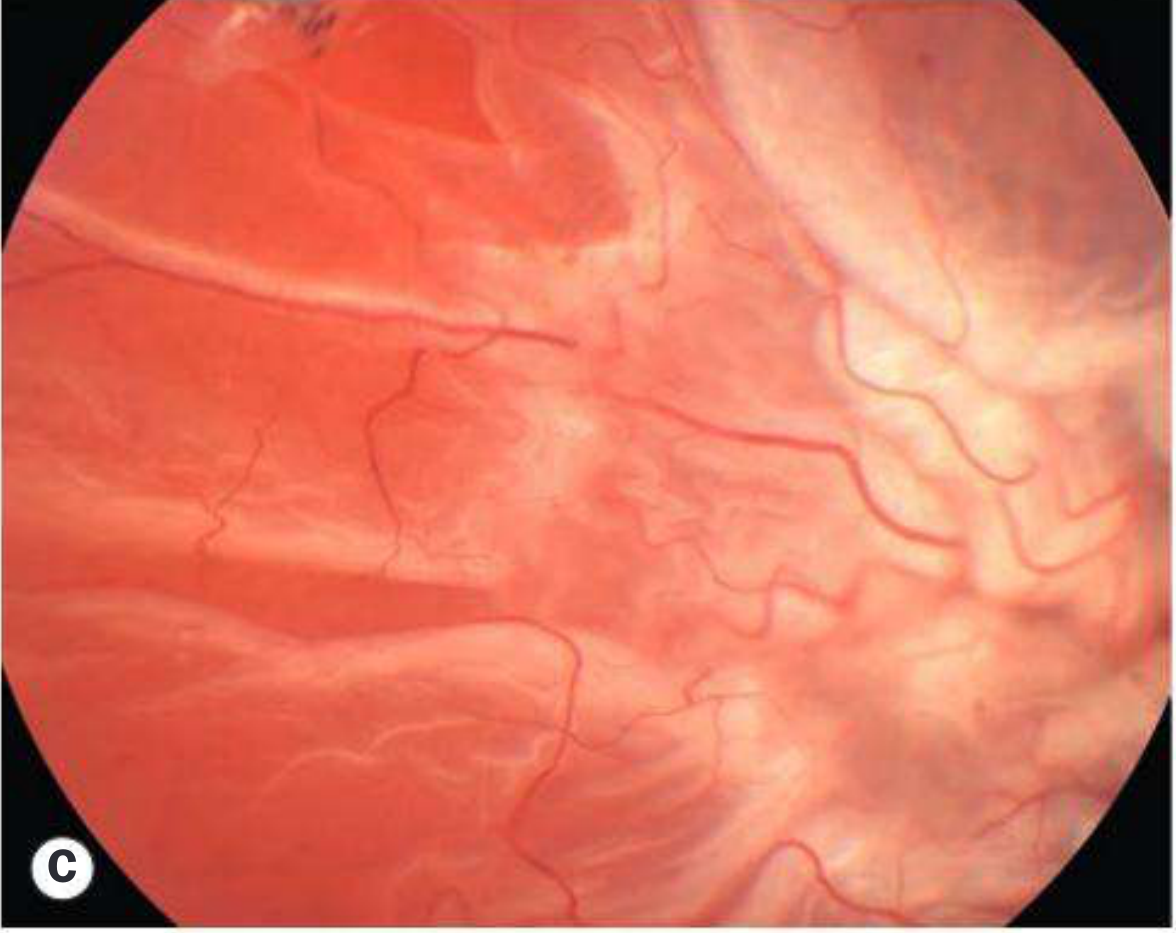
Fig. 16.25 PVR. (A) Early retinal wrinkling in minimal grade B; (B) marked grade B with rolled retinal break edges; (C) grade C with upper temporal tear; (D) grade C with prominent star fold. — Kanski's Clinical Ophthalmology 10th ed.
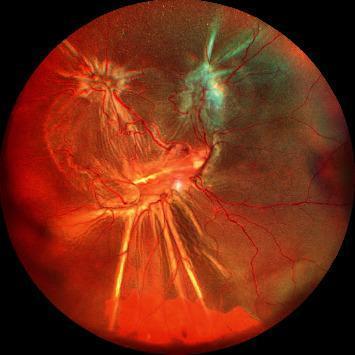
Wide-field Fundus Appearance (Grade C PVR)
Management
Medical (Adjunctive / Non-surgical)
PVR has no established pharmacological prophylaxis in routine clinical use, though recent systematic reviews have investigated several agents:
- 5-fluorouracil (5-FU) and low-molecular-weight heparin — used as adjuncts in vitreous infusion
- Methotrexate — under investigation as an intravitreal agent (2025 systematic review supports potential benefit)
- Daunorubicin, retinoic acid, and other antiproliferative/anti-inflammatory agents remain experimental
Surgical (Primary Treatment)
Goals of surgery are to release both:
- Transvitreal traction — via vitrectomy
- Tangential (surface) traction — via membrane dissection
Techniques:
| Step | Detail |
|---|---|
| Pars plana vitrectomy (PPV) | Core procedure — removes vitreous and allows access to membranes |
| Membrane peeling / dissection | Epiretinal membranes freed using scissors, picks, or forceps; small-gauge cutters can engage membranes directly |
| ILM peeling | Peeling the internal limiting membrane at the time of surgery in advanced PVR improves surgical success rate |
| Relaxing retinotomy / retinectomy | Performed when residual traction prevents adequate retinal reattachment |
| Perfluorocarbon liquid (PFCL) | Used intraoperatively to stabilize and unfold the retina |
| Tamponade | Retina is finally tamponaded with long-acting gas (C₃F₈) or silicone oil |
Localized fixed retinal folds are freed by removing the central plaque of epiretinal membrane, engaging the instrument in the valley between adjacent folds.
Recent Evidence Updates
Three recent systematic reviews (2025) are noteworthy:
- Non-surgical interventions for PVR (Hunter et al., Eye 2025) — comprehensive review of all pharmacological and non-surgical strategies [PMID: 40437039]
- Methotrexate in PVR treatment (Toh et al., Eye 2025 Feb) — supports potential role as intravitreal adjunct [PMID: 39674839]
- Pharmacological agents — network meta-analysis (Khosravi Mirzaei et al., Survey of Ophthalmology 2025) — comparative efficacy of multiple agents [PMID: 40032070]
These reinforce that surgery remains the mainstay of PVR treatment, while pharmacological adjuncts are gaining evidence but not yet standard of care.
— Kanski's Clinical Ophthalmology: A Systematic Approach, 10th edition, pp. 698–699, 711
This is a shared conversation. Sign in to Orris to start your own chat.