circulation of csf csf analysis applied anatomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete answer.
Cerebrospinal Fluid (CSF) - Circulation, Analysis & Applied Anatomy
1. FORMATION OF CSF
CSF is a colorless, watery fluid secreted primarily by the choroid plexus located in the lateral, third, and fourth ventricles. Approximately 70% is produced by ultrafiltration and active secretion through the choroid plexuses; the ventricular ependymal lining and cerebral subarachnoid space contribute the rest.
Mechanism of formation (Costanzo Physiology):
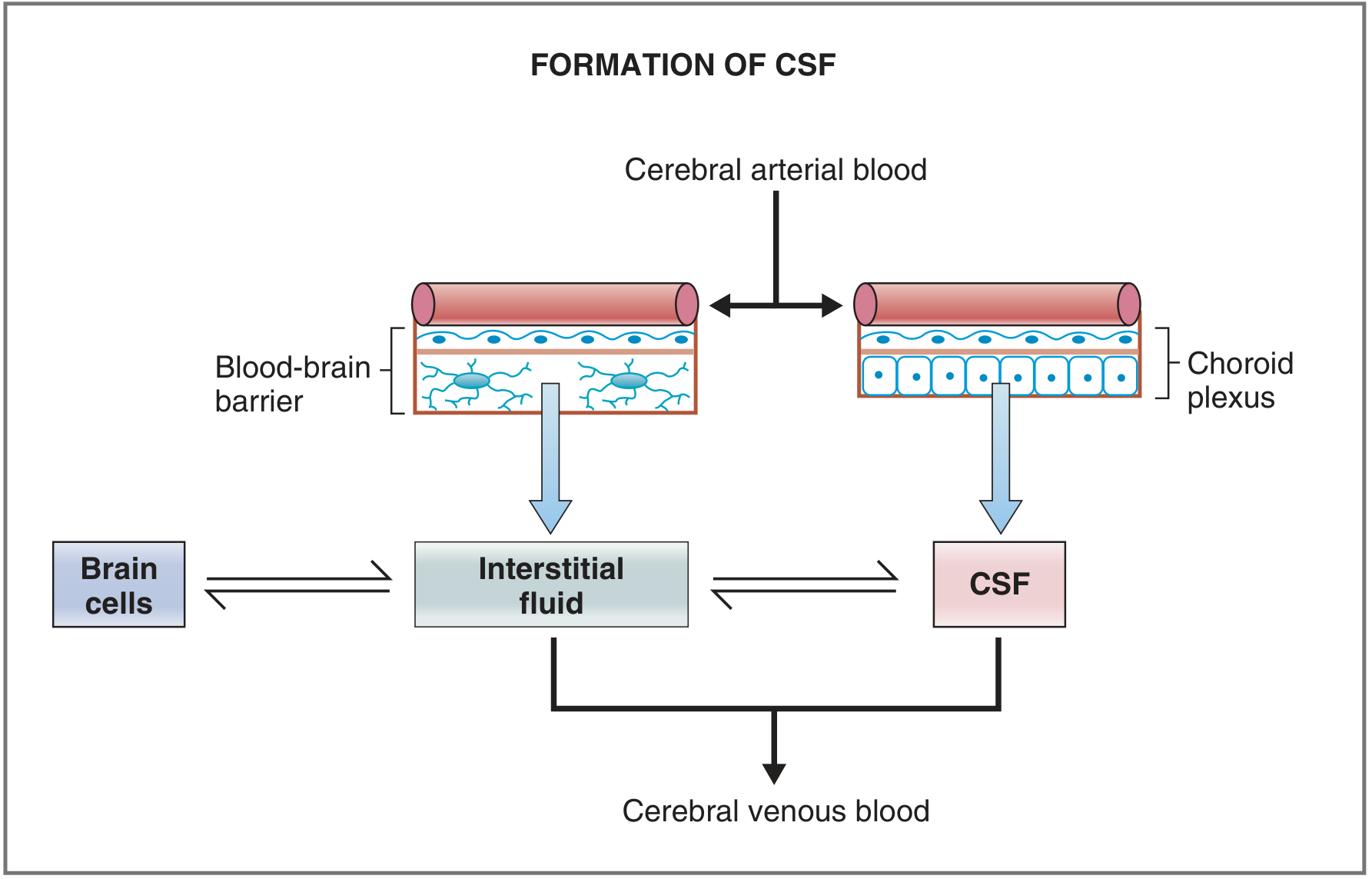
The choroid plexus acts as the brain's "kidney" - it actively transports Na+, Cl-, HCO3-, and water into the CSF, while absorbing K+ from CSF back into blood. Proteins and cholesterol are excluded due to large molecular size.
Key figures:
- Production rate: ~500 mL/day (0.3-0.4 mL/min)
- Total CSF volume: 90-150 mL (25-30 mL in ventricles; ~120 mL in subarachnoid space)
- Turnover: the entire volume is replaced every 5-7 hours (roughly 3 times per day)
- Production is influenced by circadian rhythm, peaking during sleep
2. CIRCULATION OF CSF
The pathway of CSF flow:
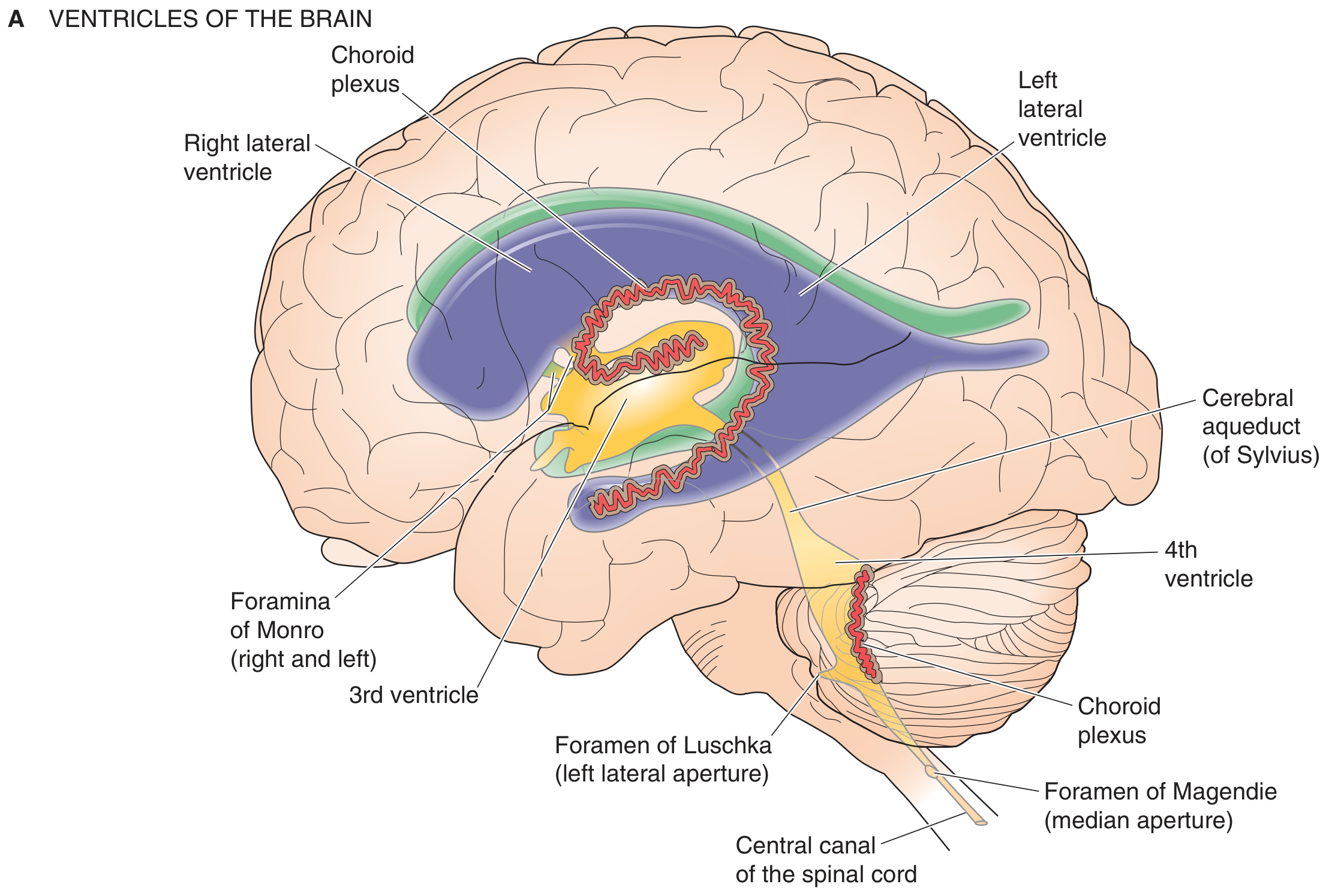
Step-by-step route (Medical Physiology - Boron & Boulpaep):
- Produced in lateral ventricles (choroid plexus along inner radius)
- Flows through foramina of Monro (interventricular foramina) into the 3rd ventricle
- Passes down the cerebral aqueduct of Sylvius into the 4th ventricle
- Exits the 4th ventricle via three openings:
- Two lateral foramina of Luschka (lateral apertures)
- One midline foramen of Magendie (median aperture)
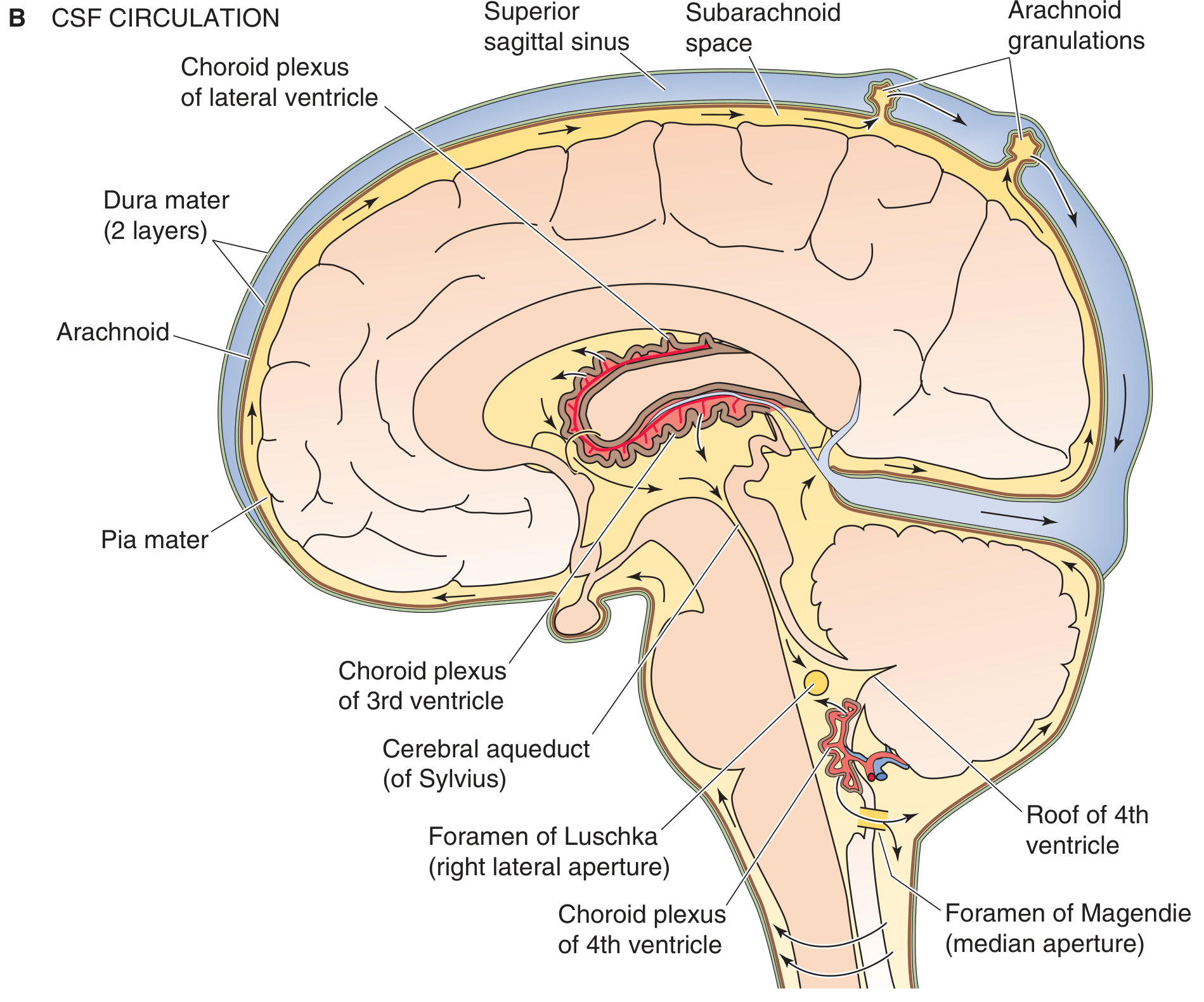
- Enters the subarachnoid space, bathing the brain and spinal cord completely
- Flows upward over the cerebral convexities
- Reabsorbed at the arachnoid granulations (Pacchionian granulations) into the superior sagittal sinus and other dural venous sinuses
The Glymphatic Pathway (Miller's Anesthesia): CSF also enters the periarterial space, moves through aquaporin-4 channels on astrocyte end-feet, travels through brain parenchyma by convective bulk flow, and exits via the perivenous space into meningeal and cervical lymphatics. This system is especially active during sleep and general anesthesia and acts as a waste-clearance mechanism.
3. MENINGES - ANATOMY
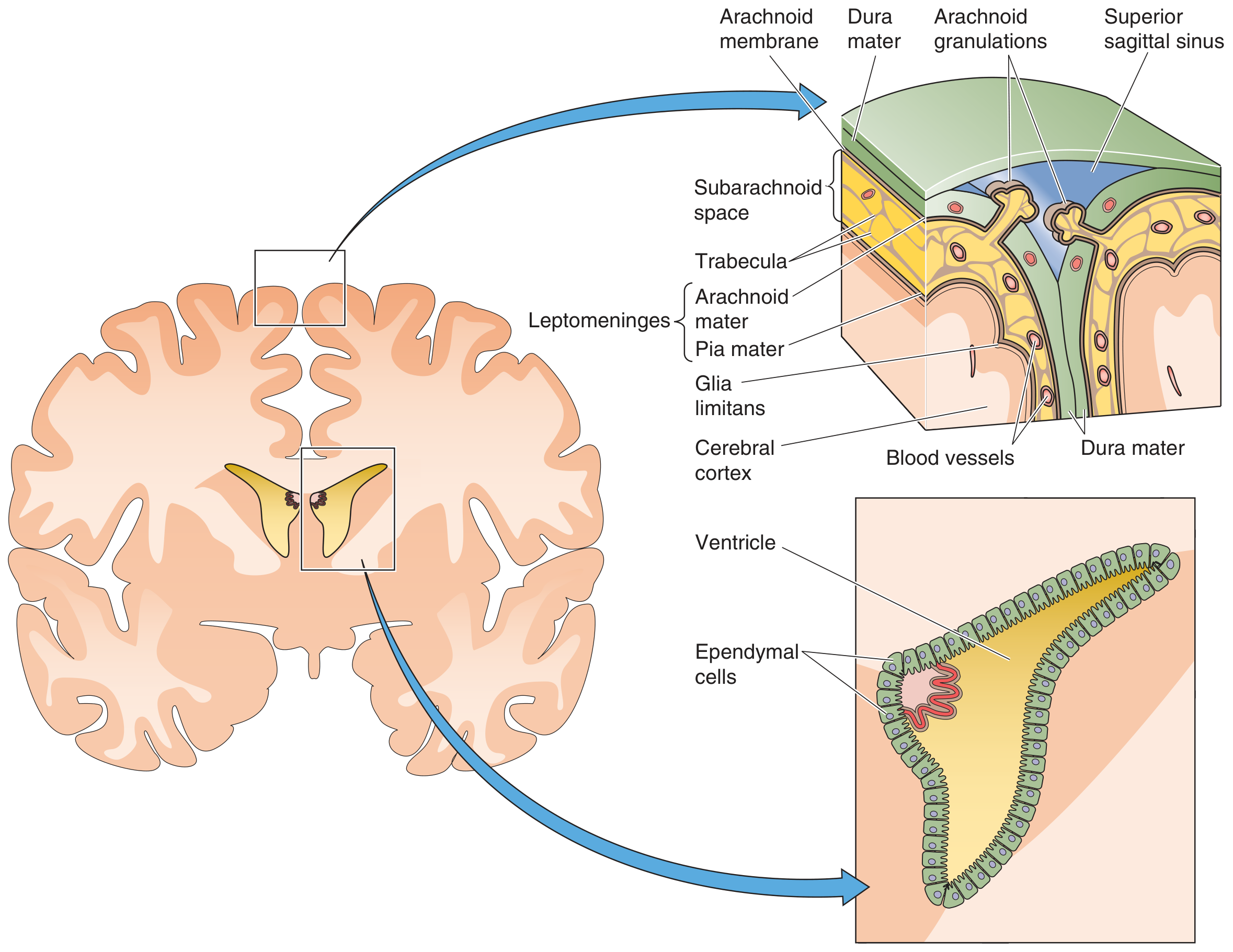
Three layers surround the brain and spinal cord:
| Layer | Description |
|---|---|
| Dura mater | Outermost, tough; two layers intracranially (periosteal + meningeal); splits to form dural venous sinuses |
| Arachnoid mater | Middle; cells connected by tight junctions; forms arachnoid granulations projecting into venous sinuses |
| Pia mater | Innermost, thin; closely applied to brain surface; follows blood vessels into brain parenchyma |
The subarachnoid space lies between arachnoid and pia mater and contains CSF, blood vessels, and trabeculae. Dilated regions of the subarachnoid space are called subarachnoid cisterns (e.g., cisterna magna, pontine cistern, lumbar cistern).
4. APPLIED ANATOMY - LUMBAR PUNCTURE
Site: Between L3-L4 or L4-L5 interspaces (below the conus medullaris, which ends at L1-L2 in adults). The needle passes through:
- Skin and subcutaneous tissue
- Supraspinous ligament
- Interspinous ligament
- Ligamentum flavum
- Epidural space
- Dura mater
- Arachnoid mater
- Subarachnoid (lumbar cistern)
CSF is also obtainable by:
- Cisternal puncture - needle into cisterna magna (between atlas and occipital bone)
- Lateral cervical puncture
- Ventricular cannulas/shunts (when already present)
Opening pressure (normal adult, lateral decubitus): 90-180 mm H2O
-
250 mm H2O = intracranial hypertension
-
200 mm H2O: remove no more than 2 mL
- Pressure varies with respiration (~10 mm), Valsalva, posture
Contraindications/Complications:
- Cerebellar tonsillar herniation (if raised ICP - most serious)
- Paresthesia, post-LP headache
- Hematoma
- Infection introduction if lumbar sepsis present
- Spinal cord compression (spinal tumors)
5. CSF ANALYSIS
Normal Reference Values (Adult Lumbar CSF)
| Parameter | Normal Value |
|---|---|
| Appearance | Crystal clear, colorless |
| Opening pressure | 90-180 mm H2O |
| WBC count | 0-5 cells/µL |
| RBC count | 0 (none) |
| Protein | 15-60 mg/dL |
| Glucose | 50-80 mg/dL (CSF:serum ratio >0.6) |
| Sodium | 135-150 mEq/L |
| Potassium | 2.6-3.0 mEq/L |
| Chloride | 115-130 mEq/L |
| Lactate | 10-22 mg/dL |
| pH (lumbar) | 7.28-7.32 |
Differential cell count (adults): Lymphocytes 62%, Monocytes 36%, Neutrophils ~2% (rare), eosinophils rare
Tube Collection Protocol
- Tube 1: Chemistry (glucose, protein) and immunology/serology
- Tube 2: Microbiology (culture, Gram stain)
- Tube 3: Hematology (cell count, differential) - least contaminated by traumatic tap
- Tube 4 (if needed): Cytology if malignancy suspected
6. INTERPRETATION OF CSF FINDINGS
Appearance
- Turbid/cloudy: WBC >200 cells/µL or RBC >400/µL, or protein >150 mg/dL
- Xanthochromia (yellow): Subarachnoid hemorrhage (bilirubin forms ~12 hrs post-bleed, peaks 2-4 days, persists 2-4 weeks); also high protein, hyperbilirubinemia
- Pink/red: RBCs from SAH or traumatic tap (distinguish by xanthochromia in supernatant after centrifuge)
- Viscous: Cryptococcal meningitis (capsular polysaccharide), mucin-secreting adenocarcinoma
- Clot formation: Traumatic tap, Froin syndrome (complete spinal block), suppurative/TB meningitis
Cellular Analysis
| Finding | Significance |
|---|---|
| Neutrophilia (PMNs >60%) | Bacterial meningitis (most common); early viral/TB/fungal meningitis; SAH; CNS infarct; post-seizure |
| PMNs >1180/µL or WBC >2000/µL | 99% predictive value for bacterial meningitis |
| Lymphocytosis (>50%) | Viral, TB, fungal, syphilitic meningitis; MS; GBS; sarcoidosis |
| Mixed cells | TB, fungal, chronic bacterial meningitis (Listeria), leptospiral, ruptured brain abscess |
| Eosinophilia (>10%) | Parasitic CNS infection (most common worldwide); Coccidioides; shunt malfunction |
| Plasma cells | Not normally present; viral meningoencephalitis, inflammatory/infectious conditions |
| Erythrophages | SAH (12-48 hrs post-bleed) |
| Siderophages (hemosiderin) | SAH (after 48 hrs, persist weeks) |
Protein
- Elevated (>60 mg/dL): Meningitis (bacterial highest), GBS, acoustic neuroma, spinal block (Froin syndrome - CSF clots due to very high protein), MS, malignancy, DM neuropathy
- Decreased (<20 mg/dL): CSF leaks, hyperthyroidism, increased ICP (increased resorption)
Glucose
- Decreased CSF glucose (<50 mg/dL or CSF:serum ratio <0.4): Bacterial, TB, fungal meningitis; carcinomatous meningitis; hypoglycemia
- Normal glucose: Viral meningitis/encephalitis (key distinguishing feature)
Diseases Detected by CSF Examination
- High sensitivity, high specificity: Bacterial, TB, viral, fungal meningitis; viral encephalitis
- High sensitivity, moderate specificity: SAH, MS, CNS syphilis, GBS, paraspinal abscess
- Moderate sensitivity, high specificity: Meningeal malignancy
7. FUNCTIONS OF CSF
- Buoyancy/mechanical support - a 1500 g brain weighs only ~50 g when suspended in CSF
- Shock absorption against acute changes in blood pressure or impact
- Waste excretion - acts as the CNS lymphatic system (no true lymphatics in the brain parenchyma)
- Transport of hypothalamic releasing factors to the median eminence
- Ionic homeostasis of the CNS environment
8. HYDROCEPHALUS (Clinical Application)
| Type | Mechanism | Cause |
|---|---|---|
| Obstructive (noncommunicating) | Block within ventricular system (CSF can't reach subarachnoid space) | Aqueductal stenosis (3rd+lateral ventricles dilate), foramen of Monro obstruction (unilateral lateral ventricle dilation), 4th ventricle outlet obstruction (all ventricles dilate) |
| Communicating | Block at arachnoid granulations; ventricles communicate with subarachnoid space | Post-meningitis, post-SAH, carcinomatous meningitis |
| Normal pressure hydrocephalus (NPH) | Impaired absorption at convexity granulations; pressure normalizes but ventricles enlarge | Classic triad: gait apraxia, dementia, urinary incontinence |
| Pseudotumor cerebri (IIH) | Raised ICP without increased CSF volume | Obesity, tetracycline, vitamin A toxicity |
- Bradley and Daroff's Neurology, Chapter 40 | Medical Physiology (Boron) | Henry's Clinical Diagnosis and Management by Laboratory Methods | Miller's Anesthesia | Costanzo Physiology
Can u write according to mbbs student
Here is the complete MBBS-level notes on CSF - written in simple, exam-friendly language with all the key points you need.
CSF - Cerebrospinal Fluid
(For MBBS Students - Anatomy + Physiology + Pathology)
WHAT IS CSF?
CSF is a clear, colorless, watery fluid that surrounds and cushions the brain and spinal cord. Think of it as the "water jacket" around your CNS.
FORMATION OF CSF
Where is it formed?
- Mainly by the Choroid Plexus (present in all 4 ventricles)
- 70% from choroid plexus
- Remaining 30% from ependymal cells lining the ventricles + cerebral subarachnoid space
How is it formed?
- Ultrafiltration of plasma + Active secretion
- The choroid plexus works like a kidney - it secretes Na+, Cl-, HCO3-, and water into CSF, and absorbs K+ back from CSF
How much is produced?
- Rate: 500 mL/day (0.3-0.4 mL/min)
- Total volume in the body at any time: 90-150 mL
- ~25-30 mL in ventricles
- ~120 mL in subarachnoid space
- The whole CSF volume is replaced 3 times a day (every 5-7 hours)
CIRCULATION OF CSF
Exam Tip: Learn this as a one-way flow pathway. This is frequently asked!
Lateral Ventricles (choroid plexus)
↓ (via Foramen of Monro / Interventricular foramen)
3rd Ventricle (choroid plexus in roof)
↓ (via Cerebral Aqueduct of Sylvius)
4th Ventricle (choroid plexus in roof)
↓ (via 3 openings)
├── Foramen of Magendie (1, median/midline)
└── Foramina of Luschka (2, lateral)
↓
Subarachnoid Space
(surrounds brain + spinal cord)
↓ (flows upward over cerebral convexities)
Arachnoid Granulations (Pacchionian Granulations)
↓
Superior Sagittal Sinus → Venous Blood
Key memory tricks:
- "2L + 1M" = 2 Luschka (Lateral) + 1 Magendie (Midline) openings of 4th ventricle
- Monro = connects Lateral to 3rd
- Sylvius = connects 3rd to 4th
MENINGES (Layers around brain and spinal cord)
From outside to inside:
| Layer | Key Feature |
|---|---|
| Dura mater | Outermost, tough; 2 layers intracranially; forms venous sinuses between the layers |
| Arachnoid mater | Middle; forms arachnoid granulations that project into superior sagittal sinus for CSF reabsorption |
| Pia mater | Innermost; closely stuck to brain surface; follows blood vessels |
- Subarachnoid space = between arachnoid and pia = filled with CSF
- Expanded parts of subarachnoid space = Cisterns (e.g., cisterna magna, lumbar cistern)
FUNCTIONS OF CSF
- Protection - cushions brain from trauma (a 1500 g brain weighs only 50 g when floating in CSF!)
- Buoyancy - reduces effective weight of brain
- Waste removal - acts as lymphatics for CNS (brain has no true lymphatics)
- Homeostasis - maintains constant ionic environment for neurons
- Transport - carries hypothalamic hormones to pituitary (median eminence)
APPLIED ANATOMY - LUMBAR PUNCTURE (LP)
Why do we do LP?
To collect CSF for diagnosis of:
- Meningitis (bacterial, viral, TB, fungal)
- Subarachnoid hemorrhage
- Multiple sclerosis
- Malignancy (meningeal carcinomatosis)
Site of LP
- Between L3-L4 or L4-L5 (safest - below conus medullaris which ends at L1-L2)
- Patient position: lateral decubitus (fetal position) or sitting - to open up the interspaces
Layers the needle passes through (from outside to inside):
Mnemonic: "Some Say Liars Love Doing All Procedures" Skin → Subcutaneous tissue → Supraspinous ligament → Interspinous Ligament → Ligamentum flavum → Epidural space → Dura mater → Arachnoid mater → Subarachnoid space ✓
- Skin
- Subcutaneous tissue
- Supraspinous ligament
- Interspinous ligament
- Ligamentum flavum
- Epidural space
- Dura mater
- Arachnoid mater
- Subarachnoid space (CSF obtained here)
Other routes of CSF collection:
- Cisternal puncture - needle into cisterna magna (between atlas and occipital bone, at back of head)
- Lateral cervical puncture
- Ventricular tap - through burr hole (neurosurgical)
Contraindications to LP:
- Raised ICP (risk of cerebellar tonsillar herniation - most dangerous complication!)
- Infection at LP site (cellulitis, abscess)
- Coagulopathy
- Spinal cord tumors with neurological deficit
Complications of LP:
- Post-LP headache (most common) - worse on sitting, relieved by lying flat
- Cerebellar herniation (most dangerous)
- Paresthesia
- Infection/meningitis
- Hematoma
CSF ANALYSIS
Collection of tubes:
| Tube No. | Goes to | Tests |
|---|---|---|
| Tube 1 | Chemistry | Glucose, Protein |
| Tube 2 | Microbiology | Culture, Gram stain |
| Tube 3 | Hematology | Cell count, Differential |
| Tube 4 (if needed) | Cytology | Malignant cells |
Tip: Tube 3 is used for cell count because it is least contaminated by a traumatic (bloody) tap.
NORMAL CSF VALUES (must memorize!)
| Parameter | Normal Value |
|---|---|
| Appearance | Clear, colorless (like water) |
| Opening pressure | 90-180 mm H2O (lateral decubitus) |
| WBC | 0-5 cells/µL (all lymphocytes/monocytes) |
| RBC | 0 (nil) |
| Protein | 15-45 mg/dL (some say up to 60) |
| Glucose | 50-80 mg/dL |
| CSF:Serum glucose ratio | >0.6 (i.e., CSF glucose = ~2/3 of blood glucose) |
| Chloride | 115-130 mEq/L |
INTERPRETATION - WHAT ABNORMAL CSF TELLS YOU
1. Appearance
| CSF Appearance | Cause |
|---|---|
| Turbid/cloudy | Bacterial meningitis (pus), high WBC |
| Xanthochromic (yellow) | Subarachnoid hemorrhage (old blood), high protein, jaundice |
| Pink/bloody | SAH or traumatic tap |
| Viscous | Cryptococcal meningitis |
| Clot forms | Froin syndrome (spinal block), TB meningitis |
Traumatic tap vs SAH: In traumatic tap, blood clears from tube 1 to tube 3. In SAH, blood is uniformly present in all tubes + xanthochromia in supernatant after centrifuge.
2. Pressure
| Pressure | Cause |
|---|---|
| High (>180 mm H2O) | Meningitis, brain tumor, cerebral edema, SAH |
| Very high (>200 mm H2O) | Remove max 2 mL only |
| Low (<80 mm H2O) | CSF leak, dehydration, spinal block above puncture site |
3. Cells (Pleocytosis)
| Cell type increased | Causes |
|---|---|
| Neutrophils (PMNs) | Bacterial meningitis (early viral/TB too, but shifts to lymphocytes in 2-3 days) |
| Lymphocytes | Viral meningitis, TB meningitis, fungal, MS, GBS, syphilis |
| Mixed (PMN + lymphocytes) | TB meningitis, fungal meningitis, Listeria, ruptured brain abscess |
| Eosinophils | Parasitic infection (most common worldwide), Coccidioides, shunt malfunction |
High-yield exam fact: PMN count >1180/µL = 99% predictive of bacterial meningitis
4. Protein
| Protein level | Causes |
|---|---|
| Increased | Bacterial meningitis (highest), TB meningitis, GBS (up to 1000 mg/dL), MS, spinal tumors, acoustic neuroma, DM neuropathy |
| Decreased | CSF leaks, hyperthyroidism, high ICP |
| Very high (clots) | Froin syndrome (complete spinal block) |
GBS (Guillain-Barré): Classic finding = Albuminocytologic dissociation = very high protein + normal/near-normal cell count
5. Glucose
| Glucose | Causes |
|---|---|
| Low CSF glucose (ratio <0.4) | Bacterial meningitis, TB meningitis, fungal meningitis, carcinomatous meningitis |
| Normal CSF glucose | Viral meningitis (KEY feature distinguishing viral from bacterial!) |
6. Summary Comparison Table (Most Exam-Tested!)
| Feature | Normal | Bacterial | Viral | TB/Fungal |
|---|---|---|---|---|
| Appearance | Clear | Turbid/Purulent | Clear | Slightly turbid |
| Pressure | 90-180 | High | Normal/slightly high | High |
| WBC | 0-5 | 100-10,000 (PMN) | 50-1000 (Lymph) | 100-500 (Lymph/Mixed) |
| Protein | 15-45 | Very high | Mildly high | High |
| Glucose | 50-80 | Low (<45) | Normal | Low |
| CSF:Serum glucose | >0.6 | <0.4 | >0.6 | <0.4 |
HYDROCEPHALUS (Applied)
| Type | Mechanism | Cause |
|---|---|---|
| Non-communicating (Obstructive) | Block inside ventricular system | Aqueductal stenosis, tumor |
| Communicating | Block at arachnoid granulations | Post-meningitis, post-SAH |
| Normal Pressure Hydrocephalus (NPH) | Impaired absorption | Triad: Wet, Wobbly, Wacky (incontinence + gait + dementia) |
| Pseudotumor cerebri (IIH) | Raised ICP, no structural cause | Obese women, OCP, tetracycline |
QUICK REVISION (Before Exams)
Foramen of Monro = Lateral → 3rd ventricle
Aqueduct of Sylvius = 3rd → 4th ventricle
Foramen of Magendie = 4th ventricle → subarachnoid (midline)
Foramina of Luschka = 4th ventricle → subarachnoid (lateral, x2)
Arachnoid granulations = CSF reabsorbed into superior sagittal sinus
LP site = L3-L4 or L4-L5 (below conus medullaris = L1/L2)
Normal protein = 15-45 mg/dL
Normal WBC = 0-5 cells/µL
Normal glucose = 50-80 mg/dL (2/3 of blood glucose)
Normal pressure = 90-180 mm H2O
Albuminocytologic dissociation = GBS (high protein, normal cells)
Low glucose + high PMNs = Bacterial meningitis
Normal glucose + Lymphocytes = Viral meningitis
Xanthochromia = SAH (not traumatic tap)
Please add reference
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.