Explain each and everything about the anterior abdominal wall. I want each minor detail about that topic. Also explain the clinical correlates along the content
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete, detailed answer.
The Anterior Abdominal Wall - A Complete Reference
1. Boundaries and Overview
The anterior abdominal wall forms the front and sides of the abdominal cavity. Its boundaries are:
- Superior: costal margins (ribs 7-10) and xiphoid process of sternum
- Inferior: inguinal ligaments, pubic crests, and pubic symphysis
- Posterior limit (functionally): anterior superior iliac spines (ASIS) laterally
It is more precisely called the anterolateral abdominal wall because the truly "anterior" muscles (rectus abdominis, pyramidalis) are flanked by three lateral flat muscles on each side.
The wall serves to: contain and protect viscera, maintain posture against gravity, increase intra-abdominal pressure (for micturition, defecation, parturition, coughing, vomiting), and assist quiet and forced expiration.
- Gray's Anatomy for Students, p. 326 - Schwartz's Principles of Surgery, p. 1549
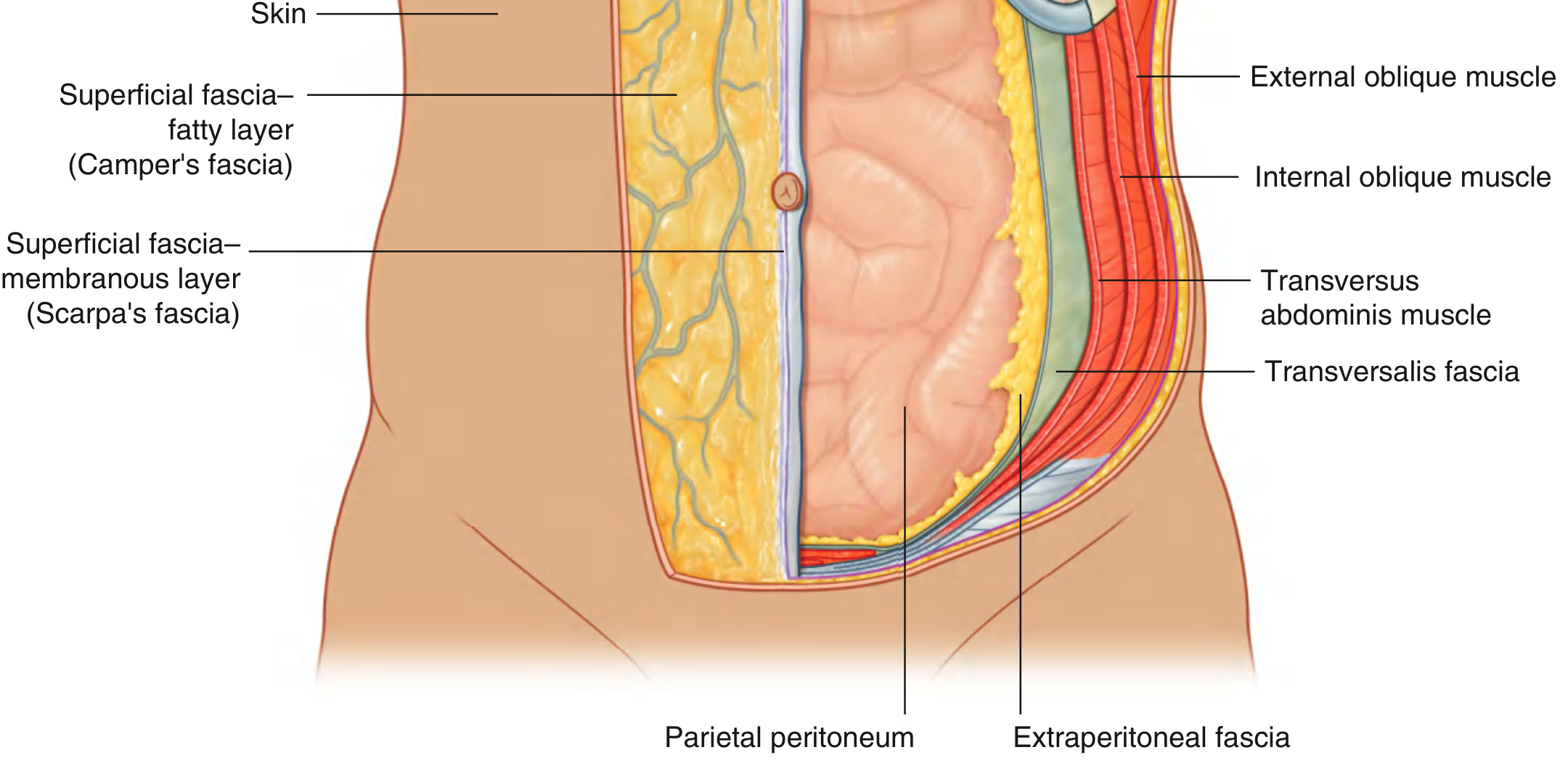
2. Layers of the Anterior Abdominal Wall (Deep to Superficial)
There are 9 distinct layers, memorized with the mnemonic "Skin, Sex, Camper, Scarpa, EOI, IOI, TA, TF, PP":
| Layer | Detail |
|---|---|
| 1. Skin | Thin, mobile, Langer's lines run transversely in most of the abdomen |
| 2. Superficial fascia - Camper's layer | Fatty layer (panniculus adiposus); continuous with superficial perineal fascia; contains dartos muscle fibers of scrotum |
| 3. Superficial fascia - Scarpa's layer | Membranous (fibrous) deep layer; fuses with fascia lata of thigh ~1 cm below inguinal ligament; continues onto penis/clitoris and scrotum/labia majora |
| 4. External oblique muscle/aponeurosis | Flat muscle |
| 5. Internal oblique muscle/aponeurosis | Flat muscle |
| 6. Transversus abdominis muscle/aponeurosis | Flat muscle |
| 7. Transversalis fascia | Deep fascia lining the inner surface |
| 8. Preperitoneal (extraperitoneal) adipose tissue | Variable fat layer |
| 9. Parietal peritoneum | Innermost layer |
- Schwartz's Principles of Surgery, p. 1549 - Greenfield's Surgery, p. 3632
3. Superficial Fascia in Detail
Camper's Fascia
- The outer, fatty layer of the superficial fascia
- Contains copious adipose tissue (the "panniculus adiposus") - can be enormous in obese individuals
- Contains the superficial epigastric vessels and superficial circumflex iliac vessels (both branches of the femoral artery and vein)
- Contains lymphatics draining into inguinal lymph nodes
- Inferiorly continuous with the outer perineal fascia
- Contains dartos smooth muscle fibers that form the dartos muscle of the scrotum
Scarpa's Fascia
-
The deep, membranous layer of the superficial fascia
-
A condensation of fibrous components - not truly a distinct layer, but compressed fibrous tissue
-
Forms the fundiform ligament of the penis (suspensory ligament of the clitoris in women)
-
Continues onto the penis and scrotum, fusing with superficial perineal fascia
-
Clinical note: Scarpa's fascia fuses with fascia lata of the thigh just below the inguinal ligament. This seals off the potential space beneath the inguinal ligament - important in urine extravasation (see clinical section)
-
Greenfield's Surgery, p. 3632 - Gray's Anatomy for Students, p. 338
4. The Five Anterolateral Muscles
A. External Oblique
| Feature | Detail |
|---|---|
| Origin | Outer surface of ribs 5-12 |
| Insertion | Xiphoid process, linea alba, pubic tubercle, pubic crest, ASIS via iliac crest |
| Fiber direction | "Hands in pockets" - inferomedially |
| Aponeurosis | Wide sheet that covers the rectus; its inferior free border forms the inguinal ligament (Poupart's ligament) |
| Action | Compresses abdomen; flexes and rotates trunk (contralateral rotation) |
Key structures derived from the external oblique aponeurosis:
- Inguinal ligament: folded-under inferior edge running from ASIS to pubic tubercle
- Lacunar ligament (Gimbernat's ligament): horizontal fibers of the inguinal ligament that fan out medially to attach to the pectineal line of the pubis; forms the medial wall of the femoral canal
- Pectineal ligament (Cooper's ligament): extension of lacunar ligament along the pectineal line
- Superficial inguinal ring: triangular aperture in the aponeurosis, just superolateral to the pubic tubercle
B. Internal Oblique
| Feature | Detail |
|---|---|
| Origin | Thoracolumbar fascia, iliac crest (anterior 2/3), lateral inguinal ligament |
| Insertion | Ribs 10-12, xiphoid process, linea alba, pubic crest (via conjoint tendon) |
| Fiber direction | Superiomedially (perpendicular to external oblique) |
| Action | Compresses abdomen; ipsilateral rotation; bilateral: flexes trunk |
Key derivatives:
- Its inferior free border arches over the inguinal canal forming its roof
- Cremaster muscle arises from the internal oblique and cremasteric fascia that extend onto the spermatic cord
C. Transversus Abdominis
| Feature | Detail |
|---|---|
| Origin | Inner surface of ribs 7-12, thoracolumbar fascia, iliac crest, lateral inguinal ligament |
| Insertion | Xiphoid process, linea alba, pubic crest (via conjoint tendon) |
| Fiber direction | Transverse/horizontal - purely horizontal |
| Action | Compresses and supports abdomen; does NOT flex or rotate the trunk |
Key point: The lower free border of the transversus aponeurosis and internal oblique aponeurosis fuse to form the conjoint tendon (falx inguinalis) which reinforces the medial posterior wall of the inguinal canal and inserts on the pubic crest and pectineal line.
D. Rectus Abdominis
| Feature | Detail |
|---|---|
| Origin | Pubic symphysis and pubic crest |
| Insertion | Xiphoid process, costal cartilages of ribs 5, 6, 7 |
| Shape | Strap-like, longitudinal, paired muscles flanking the linea alba |
| Tendinous inscriptions | 3 transverse fibrous bands that cross the muscle and are fused to the anterior rectus sheath (not the posterior) - basis of the "six pack" |
| Semilunar line | The slight lateral depression corresponding to the lateral edge of the rectus - marks the lateral edge of the rectus sheath |
| Action | Flexes trunk; compresses abdomen; stabilizes pelvis during walking |
E. Pyramidalis
-
Small triangular muscle anterior to the rectus abdominis, within the rectus sheath
-
Origin: pubic symphysis; Insertion: linea alba
-
Often absent (20% of people)
-
Action: tenses the linea alba
-
Innervated by subcostal nerve (T12)
-
Gray's Anatomy for Students, p. 333-336 - Schwartz's Principles of Surgery, p. 1549
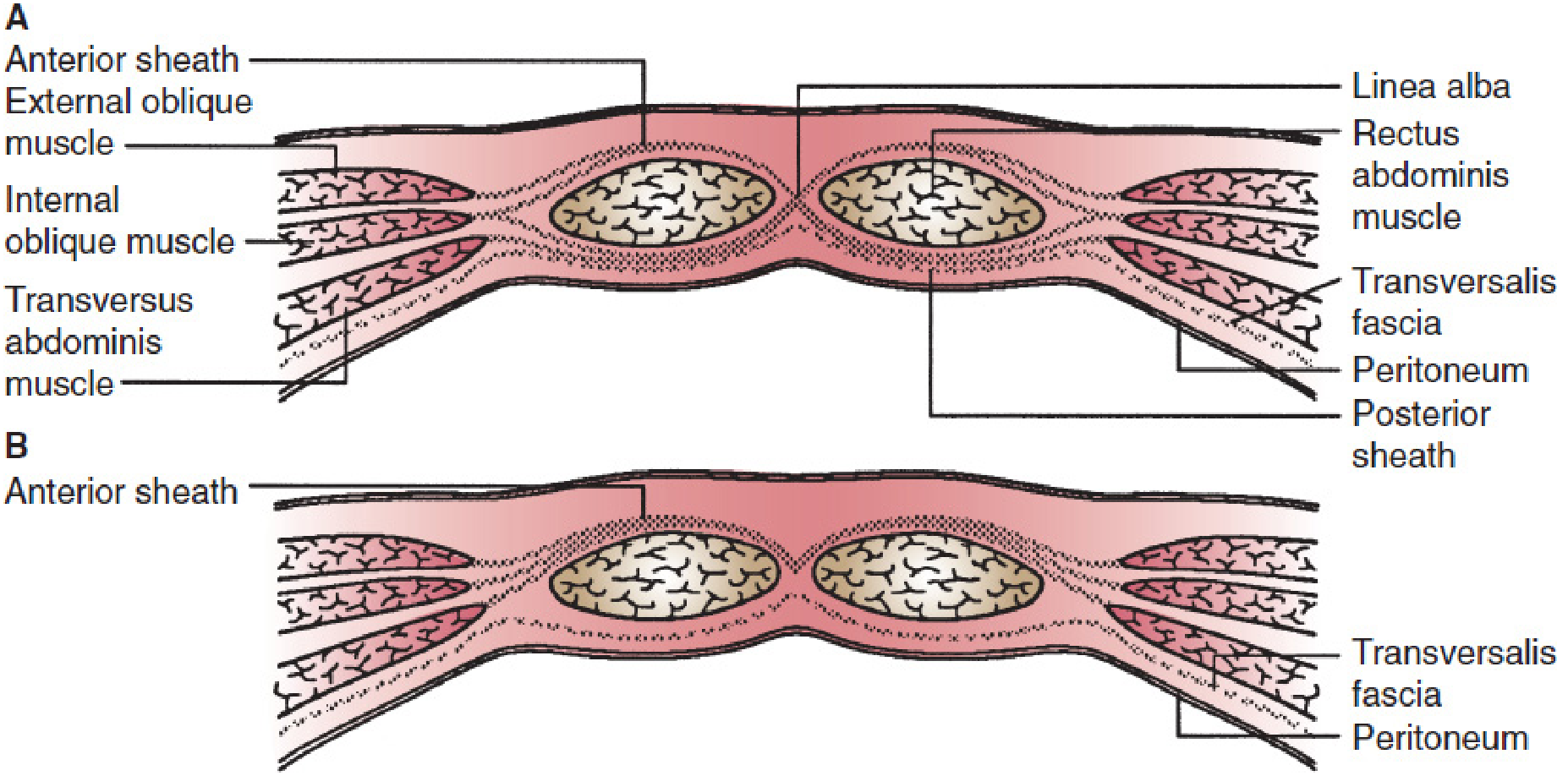
5. The Rectus Sheath
The rectus sheath is a fibrous compartment formed by the fusion of the aponeuroses of all three flat muscles. Its composition differs above and below the arcuate line (of Douglas).
Above the Arcuate Line (most of the abdomen):
- Anterior sheath: aponeurosis of external oblique + anterior lamina of internal oblique
- Posterior sheath: posterior lamina of internal oblique + aponeurosis of transversus abdominis
- Transversalis fascia and peritoneum lie deep to the posterior sheath
Below the Arcuate Line (lower 1/4 of abdomen):
- Anterior sheath: ALL three aponeuroses pass anteriorly (external oblique + both laminae of internal oblique + transversus abdominis)
- Posterior sheath: ABSENT (only transversalis fascia and peritoneum remain)
- The arcuate line is typically located about midway between the umbilicus and the pubic symphysis
Clinical Correlate - Arcuate line significance: Below the arcuate line, the posterior rectus sheath is absent - only transversalis fascia and peritoneum cover the deep surface of the rectus muscle. A rectus sheath hematoma (from inferior epigastric artery injury) below the arcuate line can spread more freely than above it. The epigastric vessels lie posterior to the rectus in this region and are at risk during laparoscopic trocar placement.
- Greenfield's Surgery, p. 3640 - Schwartz's Principles of Surgery, p. 1549
Important Aponeurotic Structures:
- Linea alba: midline fusion of all six layers of aponeuroses (from both sides). Broad superiorly (up to 1 cm between umbilicus and xiphoid), nearly absent (a mere fibrous line) below the umbilicus
- Linea semilunaris: curved lateral border of the rectus muscle / rectus sheath - visible in lean individuals
- Spigelian line: another name for the lateral edge of the rectus sheath at the point where the transversus aponeurosis begins; site of Spigelian hernias (see below)
6. The Transversalis Fascia
- The deep fascia lining the deep surface of the transversus abdominis
- Part of the general "endoabdominal fascia" that lines the entire abdominal cavity
- Superiorly: continuous with the diaphragmatic fascia
- Inferiorly: blends with the iliac fascia
- Medially: participates in the midline structures
- Forms the internal spermatic fascia as it evaginates at the deep inguinal ring to surround the spermatic cord/round ligament
- Iliopubic tract: a thickened band of the transversalis fascia running parallel to and posterior to the inguinal ligament - important in laparoscopic hernia repair (marks the lower limit of mesh placement to avoid femoral nerve injury)
7. Blood Supply
Deep/Main Arteries:
| Artery | Origin | Course |
|---|---|---|
| Superior epigastric | Internal thoracic (mammary) artery | Enters rectus sheath from above, runs posterior to rectus |
| Inferior epigastric | External iliac artery (just above inguinal ligament) | Enters rectus sheath from below the arcuate line; runs posterior to rectus |
| Deep circumflex iliac | External iliac artery | Runs along inner surface of iliac crest, supplies lower lateral wall |
| Lower posterior intercostals | Aorta (T7-T11) | Supply upper lateral abdominal wall |
| Subcostal artery | Aorta (T12) | Supplies lowest lateral abdominal wall |
| Musculophrenic artery | Internal thoracic | Supplies upper lateral wall |
Superior and inferior epigastric arteries anastomose within the rectus sheath along the posterior surface of the rectus muscle - creating a continuous channel from internal thoracic to external iliac arteries. This anastomosis is clinically exploited in TRAM (transverse rectus abdominis myocutaneous) flap breast reconstruction.
Superficial Arteries:
- Superficial epigastric artery: branch of femoral artery; runs superiorly in Camper's fascia toward the umbilicus
- Superficial circumflex iliac artery: branch of femoral artery; runs laterally toward the ASIS
- Superficial external pudendal arteries: supply the scrotum/labia
Venous Drainage:
- Follows the arteries
- Thoracoepigastric vein: superficial longitudinal vein connecting femoral vein below to axillary vein above; becomes visible and enlarged in portal hypertension or SVC/IVC obstruction ("caput medusae")
Clinical Correlate - Caput Medusae: In portal hypertension, blood is diverted through portal-systemic anastomoses. The paraumbilical veins (running in the falciform ligament) dilate and connect with the epigastric veins of the anterior abdominal wall, creating visible dilated veins radiating from the umbilicus - "caput medusae."
8. Nerve Supply
Anterior Rami of Intercostal Nerves (T7-T11):
- Enter the anterior abdominal wall laterally, pass between the internal oblique and transversus abdominis, and enter the posterior rectus sheath
- Pierce the anterior rectus sheath to become anterior cutaneous nerves
- Also give lateral cutaneous branches
Subcostal Nerve (T12):
- Anterior ramus of T12
- Runs in same plane as intercostal nerves, entering lateral abdominal wall
Iliohypogastric Nerve (L1):
- Branch of lumbar plexus (L1)
- Runs between internal oblique and transversus, pierces internal oblique above ASIS
- Lateral cutaneous branch: supplies skin of the gluteal and hip region
- Anterior (medial) cutaneous branch: supplies skin above the pubis
Ilioinguinal Nerve (L1):
- Closely related to iliohypogastric; passes through the inguinal canal
- Exits through the superficial inguinal ring
- Supplies skin of upper medial thigh, root of penis/clitoris, superior scrotum/labia majora
Genitofemoral Nerve (L1-L2):
- Femoral branch: passes under inguinal ligament to supply skin of femoral triangle
- Genital branch: passes through deep inguinal ring and inguinal canal; supplies cremaster muscle and skin of scrotum/labia majora
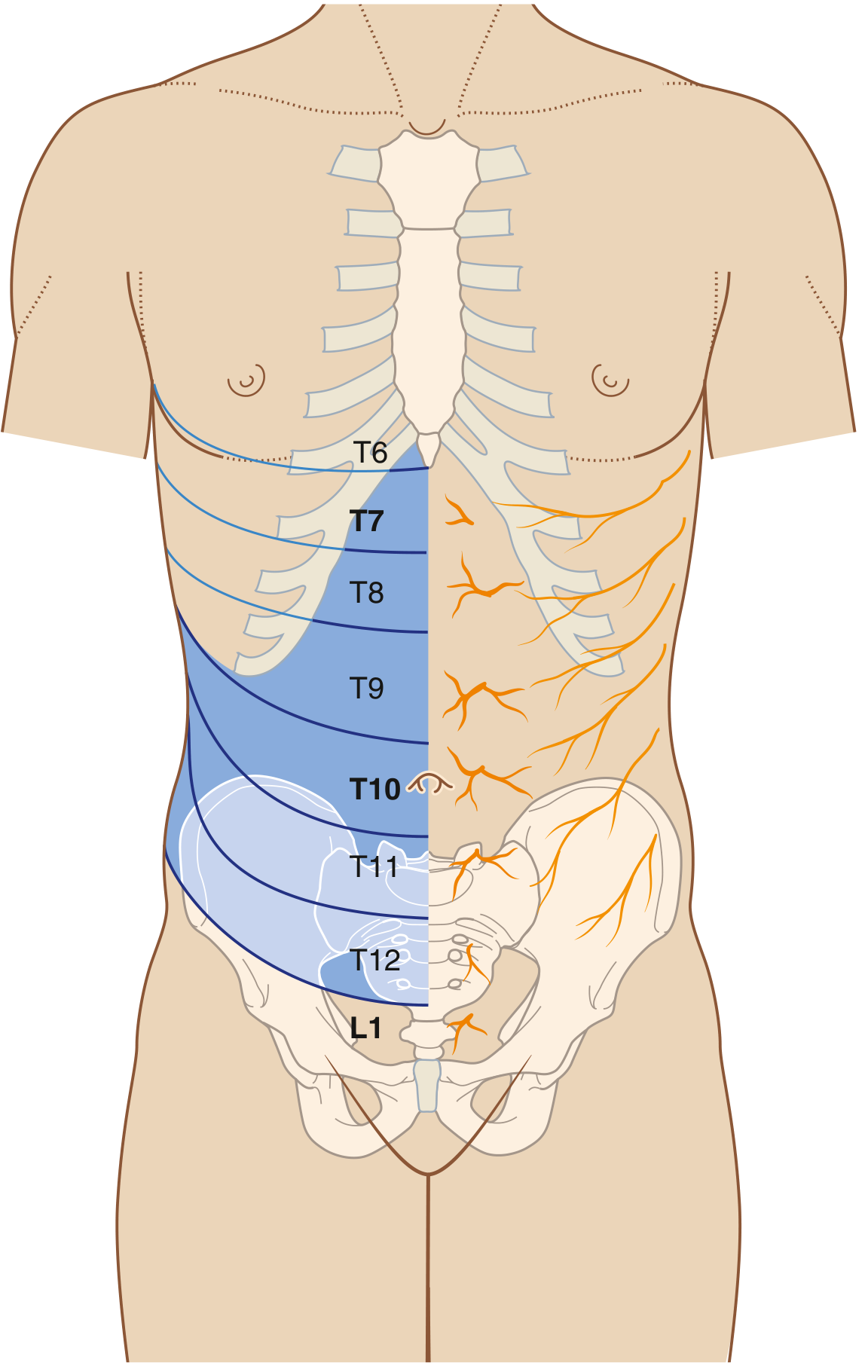
Dermatome Map:
| Region | Innervation |
|---|---|
| Infrasternal angle (xiphoid) | T6 |
| Umbilicus | T10 |
| Inguinal / suprapubic region | L1 |
Clinical Correlate - Referred Pain: Appendicitis classically begins as central/periumbilical pain (T10 - the level of the appendix's visceral innervation) before localizing to the right iliac fossa (via somatic innervation of the parietal peritoneum at McBurney's point). Ureteric colic from a stone at the ureterovesical junction refers to the groin/scrotum/labia (L1).
- Gray's Anatomy for Students, p. 326
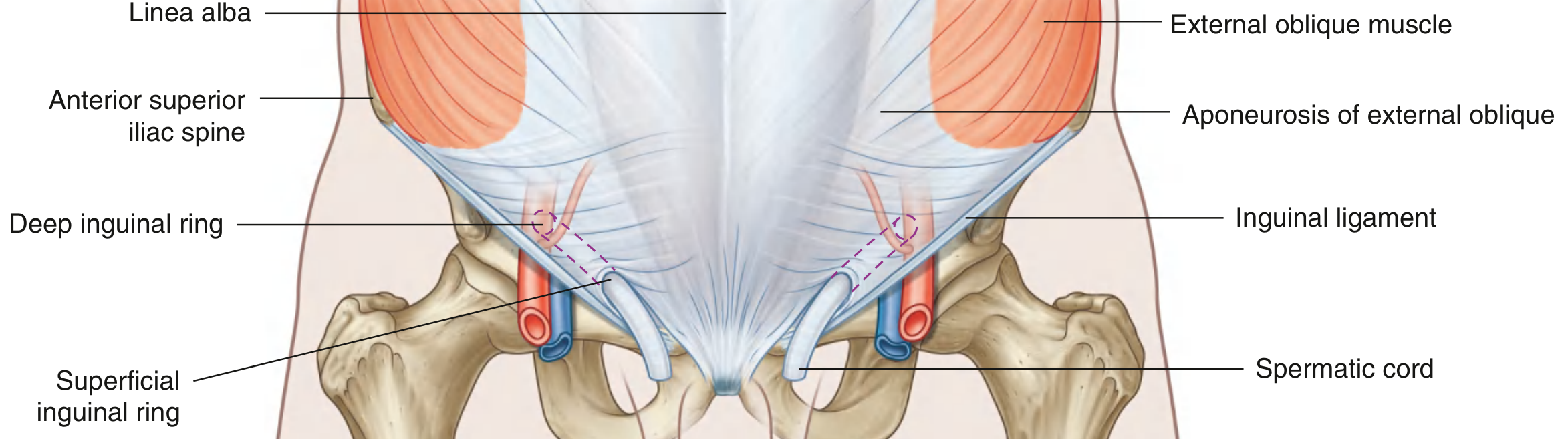
9. The Inguinal Canal
The inguinal canal is a 4 cm oblique passage through the lower anterior abdominal wall, running parallel and just above the medial half of the inguinal ligament.
Direction: superolateral to inferomedial (from deep to superficial ring)
Walls:
| Wall | Structure |
|---|---|
| Anterior wall | Aponeurosis of external oblique (entire length); reinforced laterally by internal oblique |
| Posterior wall | Transversalis fascia (entire length); reinforced medially by conjoint tendon |
| Roof | Arching fibers of internal oblique and transversus abdominis |
| Floor | Inguinal ligament + lacunar ligament (medially) |
Rings:
Deep (internal) inguinal ring:
- Located midway between ASIS and pubic symphysis (approximately 1.5 cm above the midpoint of the inguinal ligament)
- Immediately lateral to the inferior epigastric vessels
- Not a true hole - is the beginning of the tubular evagination of transversalis fascia
- Forms the internal spermatic fascia
Superficial (external) inguinal ring:
- Triangular opening in the aponeurosis of external oblique
- Located just superolateral to the pubic tubercle
- Apex points superolaterally; base = pubic crest
- Medial crus attaches to pubic symphysis; lateral crus to pubic tubercle
- Intercrural fibers (from inguinal ligament) prevent the ring from widening
- Forms the external spermatic fascia
Contents:
In men: spermatic cord, ilioinguinal nerve, genital branch of genitofemoral nerve
In women: round ligament of uterus, ilioinguinal nerve, genital branch of genitofemoral nerve
The Spermatic Cord contains (3+3+3):
- Arteries (3): testicular artery, artery of vas deferens, cremasteric artery
- Veins (3): pampiniform plexus (becomes testicular vein), lymphatics
- Other (3): ductus (vas) deferens, genital branch of genitofemoral nerve, sympathetic nerves
Coverings of the Spermatic Cord (from inner to outer):
- Internal spermatic fascia - from transversalis fascia at the deep ring
- Cremasteric muscle and fascia - from internal oblique
- External spermatic fascia - from external oblique aponeurosis at the superficial ring
- Gray's Anatomy for Students, p. 351-353
10. Hesselbach's Triangle (Inguinal Triangle)
Defines the area of the posterior wall of the inguinal canal through which direct inguinal hernias emerge:
| Border | Structure |
|---|---|
| Medial | Lateral border of rectus abdominis |
| Lateral/Inferior | Inferior epigastric vessels |
| Inferior | Inguinal ligament (medial half) / iliopubic tract |
The floor of Hesselbach's triangle is formed by the conjoint tendon medially and transversalis fascia laterally. Direct hernias pass through the medial aspect (posterior) and emerge directly through the superficial ring without traversing the full inguinal canal.
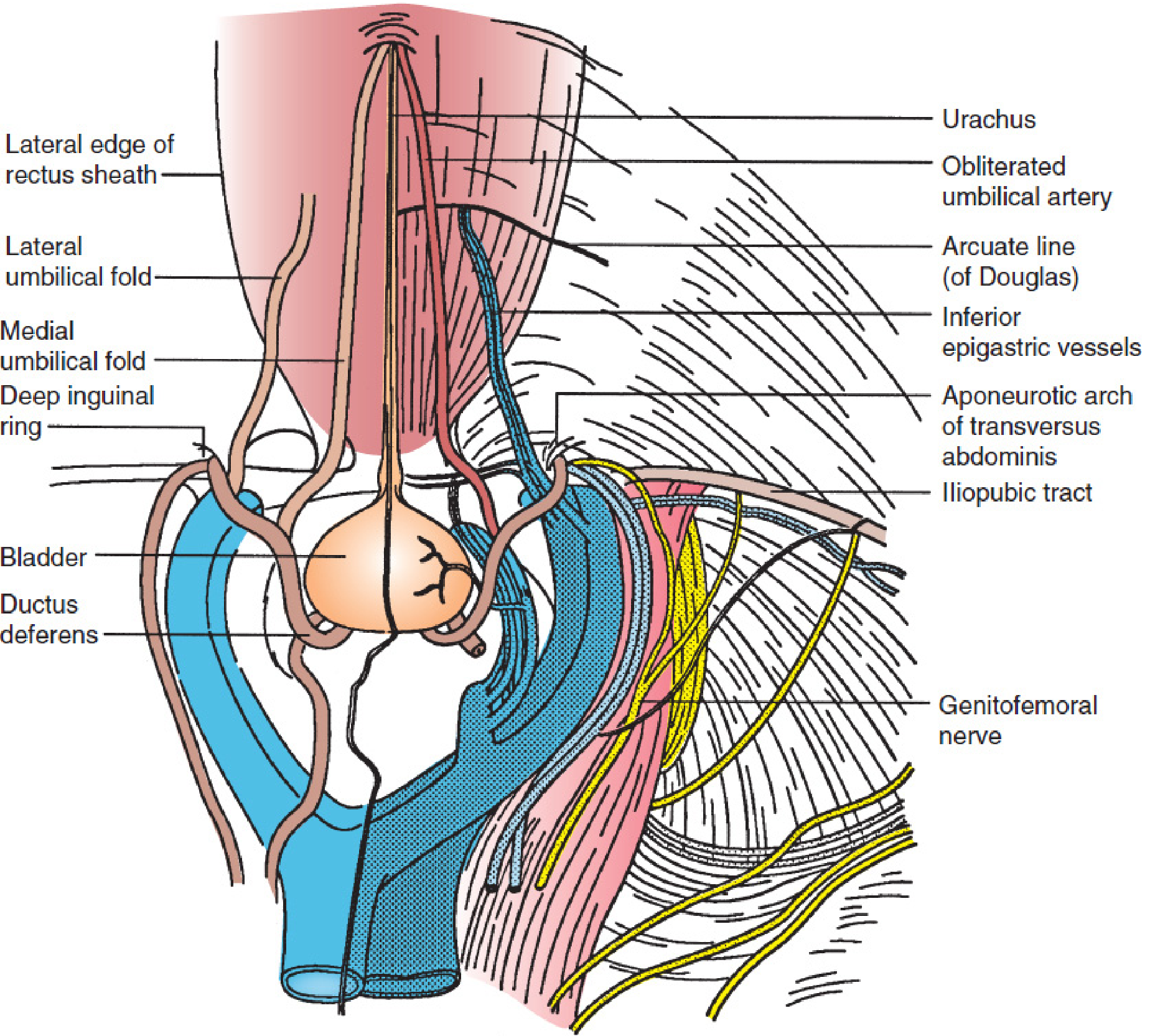
11. The Umbilicus and Peritoneal Folds
Umbilicus:
- Scar of the former umbilical cord attachment
- Located at the level of the fibrocartilaginous disc between L3 and L4 vertebrae
- Weakest point of the linea alba - common site for umbilical hernias
Peritoneal Folds (visible on the inner surface of the anterior abdominal wall):
| Fold | Contents | Remnant of |
|---|---|---|
| Median umbilical fold | Median umbilical ligament | Urachus (allantois remnant) |
| Medial umbilical folds (paired) | Medial umbilical ligaments | Obliterated umbilical arteries |
| Lateral umbilical folds (paired) | Inferior epigastric vessels | - (carries live vessels) |
Clinical Correlate: The median umbilical fold (urachus) can persist as a patent urachus connecting the bladder to the umbilicus, causing urinary drainage at the umbilicus.
Fossae between the folds (laparoscopic landmarks):
- Supravesical fossa: between median and medial folds
- Medial inguinal fossa: between medial and lateral umbilical folds (the area of Hesselbach's triangle - site of direct hernia)
- Lateral inguinal fossa: lateral to the lateral umbilical fold, over the deep inguinal ring (site of indirect hernia emergence)
12. Clinical Correlates
A. Hernias
Inguinal Hernias (most common overall):
| Feature | Indirect Inguinal | Direct Inguinal |
|---|---|---|
| Cause | Congenital (patent processus vaginalis) or acquired | Acquired weakness of posterior wall |
| Location | Enters through deep ring, lateral to inferior epigastric vessels | Pushes through Hesselbach's triangle, medial to inferior epigastric vessels |
| Path | Traverses entire inguinal canal; can enter scrotum | Directly through posterior wall; rarely enters scrotum |
| Age | Any age (especially young males) | Older adults |
| Strangulation risk | Higher | Lower |
| Reduction | Indirect pressure superolateral | Pressure directly medial |
The relationship to the inferior epigastric vessels is the definitive intraoperative distinction: indirect hernia sac is lateral, direct hernia sac is medial to the vessels.
Femoral Hernia:
- Passes through the femoral canal (medial compartment of the femoral sheath) below the inguinal ligament
- More common in women (wider pelvis, wider femoral canal)
- Has the highest strangulation risk of all groin hernias (narrow neck of femoral ring)
- Presents as a swelling below and lateral to the pubic tubercle (vs. inguinal hernia, which is above and medial to pubic tubercle)
Umbilical Hernia:
- Through the umbilical ring (physiological hernia is normal in neonates - closes by 2 years)
- True umbilical hernias in children vs. paraumbilical hernias in adults (through linea alba near umbilicus)
- Associated with obesity, ascites, multiple pregnancies
Epigastric Hernia:
- Protrusion of preperitoneal fat (and occasionally peritoneum) through defects in the linea alba between xiphoid and umbilicus
- More common in males, 20-50 years
- Usually small, can be multiple, frequently painful disproportionate to size
Spigelian Hernia:
- Hernia through the linea semilunaris (lateral border of rectus sheath), typically at the level of the arcuate line
- Often interparietal (between layers of the abdominal wall) - can be missed clinically
- Diagnosis often requires CT or ultrasound
Congenital Wall Defects:
- Omphalocele: midgut fails to return to abdomen at ~12 weeks gestation; contents herniate through umbilical ring covered by an amniotic/peritoneal membrane
- Gastroschisis: paraumbilical defect (usually right side) without amniotic sac coverage; bowel is exposed, thickened, and matted; associated with vascular compromise rather than genetic defects
B. Rectus Sheath Hematoma
- Rupture of the superior or inferior epigastric artery (or directly from the rectus muscle)
- Causes: violent coughing, physical exertion, anticoagulant therapy, trauma
- Presents as sudden onset unilateral abdominal pain with a tender abdominal mass
- Carnett's sign: pain increases (not decreases) on tensing the abdominal muscles (distinguishes from intra-abdominal pathology)
- Below the arcuate line: hematoma can spread across the midline because of the absent posterior sheath
- Diagnosed by CT or ultrasound; usually managed conservatively
C. Surgical Incisions
| Incision | Layers Cut | Use | Clinical Note |
|---|---|---|---|
| Midline (linea alba) | Skin, subcutaneous, linea alba, preperitoneal fat, peritoneum | Most abdominal surgery | Relatively avascular; good exposure; but prone to incisional hernia |
| Paramedian | Through rectus sheath, retracting rectus laterally | Large resections | Stronger closure (muscle falls back over closure) |
| Subcostal (Kocher) | Rectus sheath, cutting rectus | Cholecystectomy (right), splenectomy (left) | Cuts T7-T9 nerves - risk of muscle atrophy |
| McBurney's / Gridiron | Splitting (not cutting) each muscle layer along their fibers | Appendectomy | Muscle-splitting = stronger; nerves preserved |
| Pfannenstiel | Transverse skin, rectus sheath opened transversely, rectus muscles retracted laterally | Cesarean section, pelvic surgery | Excellent cosmesis; limited exposure |
| Lanz | Similar to McBurney, more transverse | Appendectomy (cosmetic) | Better scar |
| Rocky Davis | Transverse muscle-cutting variant | Appendectomy | Better lateral exposure |
Nerve injury in subcostal incisions: Cutting the subcostal and lower intercostal nerves (T7-T11) during right subcostal (Kocher) incisions can cause denervation of the ipsilateral rectus abdominis, leading to unilateral bulging of the abdomen.
D. Urine Extravasation
- Rupture of the urethra in the perineum allows urine to track in the superficial perineal pouch
- Because Scarpa's fascia fuses with fascia lata below the inguinal ligament, urine cannot track down into the thigh
- Instead, urine tracks up the penis, over the scrotum, and into the anterior abdominal wall deep to Scarpa's fascia
- Clinically: penile/scrotal bruising and swelling + suprapubic swelling tracking up the abdomen
E. Nerve Injuries in Hernia Surgery (Inguinodynia)
- Ilioinguinal nerve (most commonly injured): numbness/pain in inner thigh and scrotum/labia
- Iliohypogastric nerve: numbness of suprapubic skin
- Genitofemoral nerve (femoral branch): numbness of anterior thigh
- Nerve entrapment in mesh is a common cause of chronic groin pain (inguinodynia) after herniorrhaphy
F. Cremasteric Reflex
- Stroking the upper inner thigh (L1 afferents via ilioinguinal/genitofemoral nerve) causes contraction of the cremaster muscle (genital branch of genitofemoral, L1-2) and retraction of the ipsilateral testis
- An absent cremasteric reflex on one side raises concern for testicular torsion
- The reflex arc: L1-L2 spinal level
G. Inguinal Lymph Node Enlargement
- Superficial inguinal lymph nodes drain the lower limb, perineum, lower anterior abdominal wall (below umbilicus), scrotum/labia majora, lower anal canal, and skin of the penis/clitoris
- The testis (being an embryological retroperitoneal structure) drains to para-aortic lymph nodes, NOT inguinal nodes
- Clinical pearl: A scrotal skin melanoma drains to inguinal nodes; testicular cancer drains to para-aortic nodes at the L1-L2 level
H. McBurney's Point
- Located 1/3 of the way from the ASIS to the umbilicus on the right side
- The surface marking of the base of the appendix
- Point of maximum tenderness in acute appendicitis
- Rebound tenderness (Blumberg's sign), Rovsing's sign, psoas sign, obturator sign are elicited near this landmark
I. Surface Anatomy and Regions
Nine-region subdivision (clinically most useful):
| Left | Central | Right | |
|---|---|---|---|
| Superior | Left hypochondrium | Epigastric | Right hypochondrium |
| Middle | Left lumbar (lateral) | Umbilical | Right lumbar (lateral) |
| Inferior | Left iliac (inguinal) | Hypogastric (pubic) | Right iliac (inguinal) |
Four-quadrant system (quick clinical reference):
- Right Upper Quadrant (RUQ): liver, gallbladder, right kidney, hepatic flexure
- Left Upper Quadrant (LUQ): stomach, spleen, left kidney, splenic flexure, tail of pancreas
- Right Lower Quadrant (RLQ): appendix, cecum, right ovary, right ureter
- Left Lower Quadrant (LLQ): sigmoid colon, left ovary, left ureter
Key Images Available from Textbooks
The following diagrams are referenced in these textbooks and capture the above anatomy visually:
Summary Table: Muscles at a Glance
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| External oblique | Ribs 5-12 (outer surface) | Iliac crest, inguinal ligament, linea alba, pubis | T7-T12 | Compresses abdomen; contralateral rotation |
| Internal oblique | Iliac crest, thoracolumbar fascia, inguinal ligament | Ribs 10-12, linea alba, pubis (conjoint tendon) | T7-T12, L1 | Compresses abdomen; ipsilateral rotation |
| Transversus abdominis | Ribs 7-12, thoracolumbar fascia, iliac crest, inguinal ligament | Linea alba, pubis (conjoint tendon) | T7-T12, L1 | Compresses abdomen only |
| Rectus abdominis | Pubic symphysis and crest | Xiphoid, costal cartilages 5-7 | T7-T12 | Flexes trunk; compresses abdomen |
| Pyramidalis | Pubic symphysis | Linea alba | T12 (subcostal) | Tenses linea alba |
Sources: Gray's Anatomy for Students (9780323934237) | Schwartz's Principles of Surgery, 11e (9781259835346) | Greenfield's (Mulholland) Surgery, 7e (9781975143169) | General Anatomy and Musculoskeletal System - THIEME Atlas (9781626237186)
This is a shared conversation. Sign in to Orris to start your own chat.