In detail about neuropathic joint or charchot arthropathy for Orthopaedic postgraduate exam in simple words cover all aspects properly
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive data from multiple authoritative sources. Let me compile the complete, detailed orthopaedic PG exam answer.
Neuropathic Joint / Charcot Arthropathy
A Complete Guide for the Orthopaedic Postgraduate Exam
1. DEFINITION
Charcot arthropathy (neuropathic joint) is a chronic, progressive, destructive arthritis affecting bone architecture and joint alignment in patients who have lost protective sensation (pain, proprioception, or both). Without these protective mechanisms, joints undergo repeated microtrauma leading to progressive cartilage and bone destruction.
- Harrison's Principles of Internal Medicine 22E, p. 3012
- Miller's Review of Orthopaedics 9th Ed, p. 602
2. HISTORY
- First described by Jean-Martin Charcot in 1868 in patients with tabes dorsalis (neurosyphilis)
- Today, diabetes mellitus is the most common cause
- The term "Charcot joint" honors him; "neuropathic arthropathy" is the more accurate modern term
3. CAUSES (Etiology) - HIGH-YIELD
Remember: "DeLiSy A-SPICS"
| Cause | Joint most affected |
|---|---|
| Diabetes mellitus (most common today) | Midtarsal, tarsometatarsal, MTP |
| Leprosy | Tarsal, tarsometatarsal |
| Syringomyelia | Shoulder, elbow, wrist |
| Amyloidosis | Knee, ankle |
| Spina bifida / Myelomeningocele | Lower limb joints |
| Syphilis (Tabes dorsalis) | Knee, hip, ankle |
| Peripheral neuropathy (alcohol, avitaminosis) | Various |
| Intraarticular steroid injections (repeated) | Any injected joint |
| Congenital insensitivity to pain | Knee, ankle, intertarsal |
| Spinal cord injury | Below-injury joints |
Key memory tip: In tabes dorsalis - knee is #1; in syringomyelia - upper limb joints (shoulder, elbow, wrist); in diabetes - foot/ankle joints.
- Rheumatology 2-Volume Set 2022, p. 2088
- Campbell's Operative Orthopaedics 15th Ed, Box 7.7
4. PATHOPHYSIOLOGY - TWO THEORIES
Two competing theories exist; the true pathogenesis is a combination of both.
Theory 1: Neurovascular Theory (French theory - Charcot's own)
- Neurologic damage → autonomic dysfunction → arteriovenous shunting → increased local blood flow
- Increased blood flow → bone resorption (osteoclastic > osteoblastic activity)
- TNF-alpha and IL-1B → increased NF-kB → increased osteoclast production → bone loss
- This is the "vascular" mechanism - bone melts away
Theory 2: Neurotraumatic Theory (German theory - Virchow & Volkmann)
- Loss of deep pain and proprioception → protective neuromuscular reflexes gone
- Joint subjected to repeated unperceived microtrauma
- Ligament tears, microfractures accumulate without healing response
- This is the "mechanical" mechanism - joint is beaten to destruction
Bottom line: Bone resorption + repeated unprotected trauma = progressive joint disorganization.
- Campbell's Operative Orthopaedics 15th Ed (foot & ankle chapter)
5. JOINT DISTRIBUTION BY DISEASE
| Disease | Joints Affected |
|---|---|
| Diabetes mellitus | Midtarsal, tarsometatarsal (TMT), MTP, talotibial |
| Tabes dorsalis | Knee (most common), hip, ankle |
| Syringomyelia | Shoulder, elbow, wrist (upper limb) |
| Amyloidosis | Knee, ankle |
| Congenital sensory neuropathy | Knee, ankle, intertarsal, MTP |
| Leprosy | Tarsal, tarsometatarsal |
Exam tip: Syringomyelia → upper limb Charcot. All others → lower limb predominantly.
6. INCIDENCE
- Occurs in approximately 1-1.5% of diabetic patients
- Up to 7.5% of diabetics with neuropathy
- Usually occurs at age ≥50 years in someone with diabetes for several years
- Up to 35% present with bilateral disease
- Pain is present in up to 50% of cases (not always painless!)
7. CLINICAL FEATURES
Symptoms:
- Swelling, warmth, redness, and deformity of the joint
- Disproportionately little pain for the degree of radiographic destruction (classic)
- Pain may occur in up to 50% from intraarticular fractures of osteophytes
- History of trivial or minor trauma triggering acute presentation
- Swelling and redness often improve in the morning (worse with activity)
Signs:
- Progressive joint enlargement (bony overgrowth + effusion)
- Joint instability, hypermobility
- Deformity - "rocker-bottom foot" in diabetic Charcot foot (downward collapse of tarsal bones → convexity of sole)
- Large bony prominences palpable (osteophytes protruding from top of foot)
- Calluses over metatarsal heads → pressure ulcers → osteomyelitis
- Crepitus, loose bodies
Classic Diabetic Charcot Foot:
-
Warm, swollen, erythematous foot
-
Arch collapse - rocker-bottom deformity
-
Often confused with cellulitis or osteomyelitis
-
No remembered significant trauma (or only trivial trauma)
-
Harrison's 22E, p. 3012
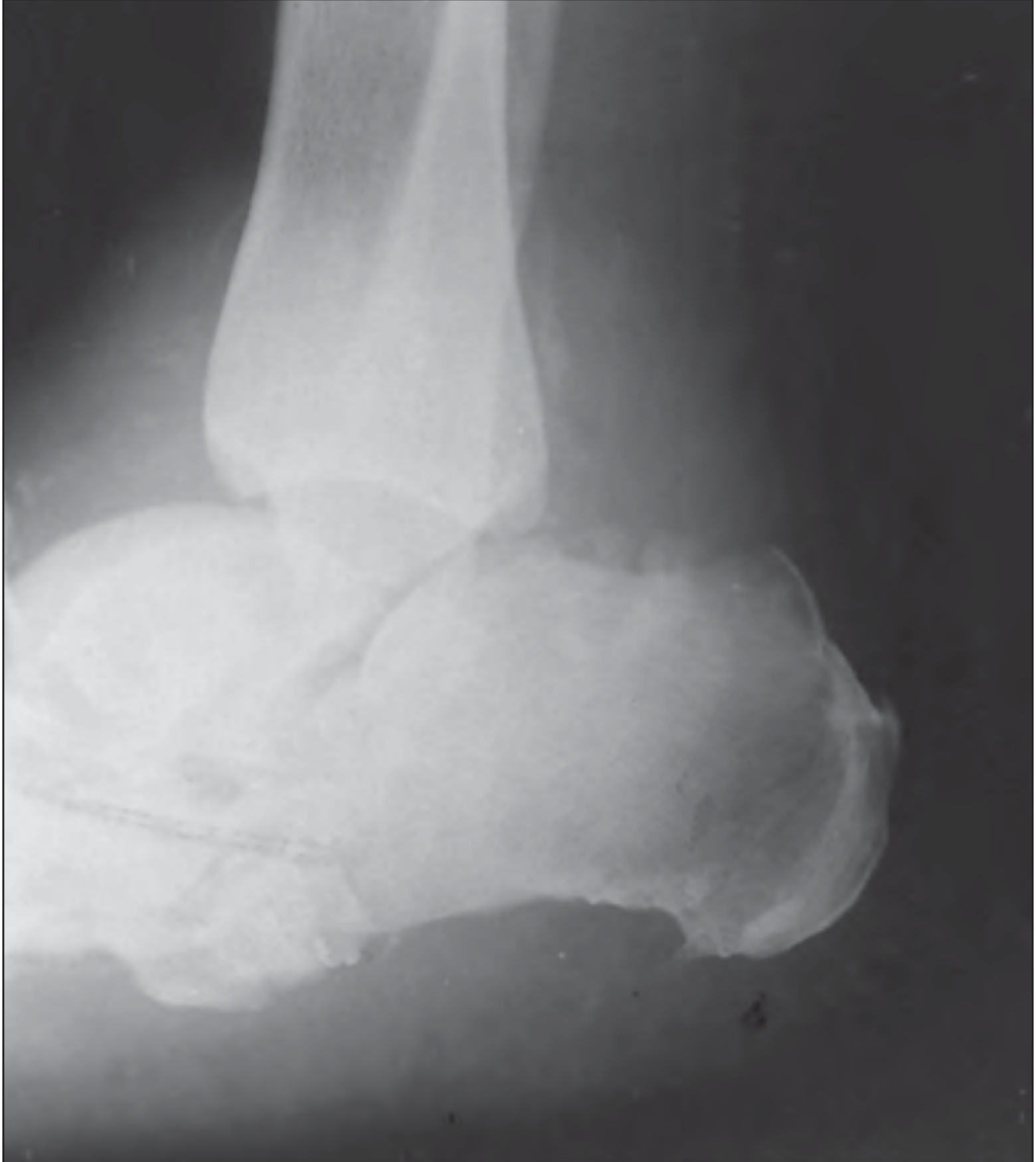
8. RADIOLOGICAL FEATURES
Radiographs are the key investigation. The classic X-ray features can be remembered as the "6 Ds":
- Distension of joint (effusion)
- Density increased (sclerosis/eburnation)
- Detritis (loose bodies, intraarticular fragments)
- Dislocation / subluxation
- Degenerative changes (joint space loss, osteophytes)
- Destruction / Disorganization (fragmentation of bone)
Additional features:
- Periarticular bone fragmentation
- Subchondral bone sclerosis (eburnation)
- Large osteophytes at joint margins
- Marked joint destruction out of proportion to clinical pain
- Resorption and tapering of distal metatarsal bones (in diabetic foot)
- "Lisfranc fracture-dislocation" pattern at tarsometatarsal joints
Joint margins in neuropathic joint = DISTINCT (vs. osteomyelitis where they are blurred)


9. HISTOLOGY
On synovial biopsy:
- Osteochondral fragments embedded within the synovium - this is diagnostic of neuropathic arthropathy
- Similar to severe OA: cartilage fragmentation, subchondral eburnation, osteophytes, loose bodies
- More advanced: erosions, devitalized bone, microscopic bone/cartilage fragments
- Synovial fluid: noninflammatory, may be xanthochromic or bloody, contains fragments of synovium, cartilage, and bone
10. STAGING - EICHENHOLTZ CLASSIFICATION (Most Important)
This is the most exam-tested classification. It is based on clinical signs, symptoms, and radiographic changes over time.
| Stage | Name | Clinical Features | Radiograph Findings |
|---|---|---|---|
| 0 | Clinical (Pre-fragmentation) | Acute inflammation; confused with infection; earliest stage | Regional bone demineralization only |
| 1 | Dissolution (Fragmentation) | Acute inflammation, swelling, erythema, warmth | Bone demineralization + periarticular fragmentation, joint dislocation |
| 2 | Coalescence | Less inflammation, decreasing swelling and erythema | Absorption of bone debris; early bone healing, periosteal new bone |
| 3 | Resolution | Resolved erythema, swelling, warmth; consolidation | Smoothed bone edges, bony/fibrous ankylosis |
Continuum from bone resorption and fragmentation to bone formation and consolidation takes 6 to 18 months.
Treatment goal: Reach Stage 3 (resolution) while maintaining alignment and ambulatory status, minimizing soft tissue breakdown.
11. BRODSKY CLASSIFICATION (Anatomic - Exam Favourite)
Classifies Charcot foot by location:
| Type | Location | Frequency |
|---|---|---|
| 1 | Midfoot (tarsometatarsal joints) - most common | ~60% |
| 2 | Hindfoot (subtalar, talonavicular, calcaneocuboid joints) | ~10% |
| 3A | Tibiotalar (ankle) joint | ~20% |
| 3B | Calcaneal tuberosity fracture | <10% |
| 4 | Combination of areas | <10% |
| 5 | Forefoot | <10% |
Type 1 (midfoot) → hindfoot valgus caused by forefoot abduction with contracted gastrocsoleus complex
Type 2 → rocker-bottom deformity; varus or valgus hindfoot
Type 3A → ulcerations over prominent malleoli; generally requires surgery
Type 3B → pathologic calcaneal fracture
12. INVESTIGATIONS
Imaging:
- Plain X-ray - first line; shows the "6 Ds" as above
- MRI - early detection; differentiates from osteomyelitis; shows bone marrow edema, joint effusion
- Bone scan (Technetium-99m) - increased uptake in BOTH neuropathic joint AND osteomyelitis - cannot differentiate
- Indium-111 labeled WBC scan - increased uptake in osteomyelitis but NOT in neuropathic joint - useful for differentiation
- CT scan - better characterizes bony fragmentation and deformity
Lab:
- ESR, CRP - may be elevated in acute phase
- Blood glucose, HbA1c - to diagnose/control diabetes
- Serologic tests for syphilis (VDRL, TPHA) if suspected
- Synovial fluid analysis: noninflammatory; fragmented cartilage/bone; absence of crystals and low neutrophils (high neutrophils suggest osteomyelitis)
13. DIFFERENTIAL DIAGNOSIS
The key differentials are:
| Condition | Differentiating Features |
|---|---|
| Osteomyelitis | Most important DD in diabetic foot; blurred joint margins on X-ray; Indium-111 WBC scan positive; cultures positive |
| Avascular Necrosis | History, location, MRI pattern different |
| Advanced OA | No neuropathy; slower progression; less fragmentation |
| Stress fracture | Location, mechanism different |
| CPPD (Calcium pyrophosphate deposition) | Crystals on joint fluid analysis |
| Septic arthritis | Acute fever, high WBC count, positive cultures |
| Cellulitis | No bony changes on X-ray |
Key differentiator from osteomyelitis:
- Neuropathic joint: distinct joint margins, Indium-111 WBC scan NEGATIVE
- Osteomyelitis: blurred joint margins, Indium-111 WBC scan POSITIVE
- Technetium bone scan: positive in BOTH - not helpful for differentiation
14. TREATMENT
Goals:
- Achieve Eichenholtz Stage 3 (resolution)
- Maintain alignment and plantigrade foot
- Preserve ambulatory status
- Minimize soft tissue breakdown and ulceration
A. NON-OPERATIVE (Conservative) - First line
Step 1: Immobilization + Non-weight-bearing
- Total Contact Cast (TCC) - gold standard for acute Charcot foot
- Non-weight-bearing for at least 8 weeks (Harrison's) to 4-6 weeks (acute phase)
- Distributes pressure evenly, reduces edema
- Continued until warmth, swelling subside
- Once swelling/warmth resolve → transition to custom brace
- AFO (Ankle-Foot Orthosis)
- CROW boot (Charcot Restraint Orthotic Walker)
Step 2: Medical management
- Bisphosphonates (e.g., pamidronate, alendronate) - reduce osteoclast activity; useful in acute phase
- Neuroleptic medications (for neuropathic pain)
- Antidepressants (amitriptyline, duloxetine) - neuropathic pain
- Topical anesthetics
- Treatment of underlying cause (glucose control in diabetes)
- Protective inserts and orthotics + regular foot examination - extremely important for prevention
Success rate: Non-operative treatment successful in up to 75% of cases
B. OPERATIVE TREATMENT
Indications:
- Stable deformity with recurrent ulcers secondary to bony prominence
- Unstable/unbraceable deformity
- Ankle and hindfoot Charcot (high failure rate of conservative management)
- Failed conservative treatment
Procedures:
| Indication | Surgery |
|---|---|
| Bony prominence causing recurrent ulcers | Exostectomy (removal of the prominence) |
| Unstable midfoot deformity | Arthrodesis (fusion) |
| Hindfoot/ankle Charcot | Tibiotalocalcaneal (TTC) arthrodesis |
| Midfoot deformity (rocker-bottom) | Plantar closed-wedge osteotomy + arthrodesis |
| Achilles contracture | TAL (Tendo-Achilles Lengthening) - almost universally required |
Fixation for ankle/hindfoot:
- Intramedullary (IM) rod - provides internal stability; can be left indefinitely
- Multiplanar external fixator - alternative option
- Even with radiographic nonunion, many patients can be pain-free and functional
Arthroplasty (TKA/THA) in Charcot joint:
- Generally a relative contraindication
- TKA: fair results reported; requires attention to alignment, ligamentous balancing, bone grafting
- THA: high rates of recurrent dislocation and loosening; surgery only for severe disability
15. COMPLICATIONS
- Pressure ulcers - over bony prominences/metatarsal heads
- Osteomyelitis - from infected ulcers; major cause of morbidity
- Recurrent deformity - especially with high BMI
- Amputation - in severe, uncontrolled cases with osteomyelitis
- Deep vein thrombosis - with prolonged immobilization
- Nonunion after surgical fusion
- Dislocation/loosening after arthroplasty
- Bilateral disease in up to 35%
16. PROGNOSIS / NATURAL HISTORY
- Natural history: acute inflammation → bone resorption → consolidation → stable deformity
- Takes 6-18 months to progress through stages
- Development of Charcot in diabetics is not related to body weight
- Recurrence linked to higher BMI
- Medial column of foot fails before lateral (pull of posterior tibial tendon)
- Sagittal plane deformities more likely to cause ulceration than transverse plane abnormalities
- Early immobilization prevents progression to advanced stages
- Diabetic patients with Charcot have lower quality of life than diabetics without it
17. KEY EXAM POINTS SUMMARY
| Fact | Answer |
|---|---|
| First described by | Jean-Martin Charcot, 1868, in tabes dorsalis |
| Most common cause today | Diabetes mellitus |
| Most common joint in diabetes | Midfoot (tarsometatarsal) |
| Most common joint in tabes dorsalis | Knee |
| Most common joint in syringomyelia | Shoulder |
| Most important classification | Eichenholtz (stages 0-3) |
| Most common Brodsky type | Type 1 (midfoot) ~60% |
| Gold standard treatment | Total Contact Cast + Non-weight bearing |
| Best imaging to differentiate from osteomyelitis | Indium-111 WBC scan |
| Technetium scan | Positive in BOTH - not useful for differentiation |
| Gold standard for ankle/hindfoot Charcot | TTC arthrodesis |
| Histological diagnosis | Osteochondral fragments embedded in synovium |
| Joint fluid character | Noninflammatory, xanthochromic/bloody, fragmented debris |
| Bilateral disease incidence | Up to 35% |
| Pain incidence | Up to 50% have some pain (not always "painless") |
| Non-operative success rate | 75% |
Sources:
- Campbell's Operative Orthopaedics 15th Edition 2026
- Miller's Review of Orthopaedics 9th Edition
- Harrison's Principles of Internal Medicine 22E (2025)
- Rheumatology 2-Volume Set (2022, Elsevier)
In detail about complete foot drop and its evaluation for Orthopaedic postgraduate exam in simple words
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive data. Let me compile the complete, detailed answer for the orthopaedic PG exam.
Foot Drop - Complete Guide for Orthopaedic Postgraduate Exam
1. DEFINITION
Foot drop (drop foot) is the inability to dorsiflex the foot and toes, resulting from weakness or paralysis of the ankle dorsiflexors. The foot hangs in a plantar-flexed (and often inverted) position at rest and cannot be lifted upward during the swing phase of walking.
It is a symptom/sign, not a diagnosis - always find the cause.
2. ANATOMY - THE FOUNDATION (Know This Inside Out)
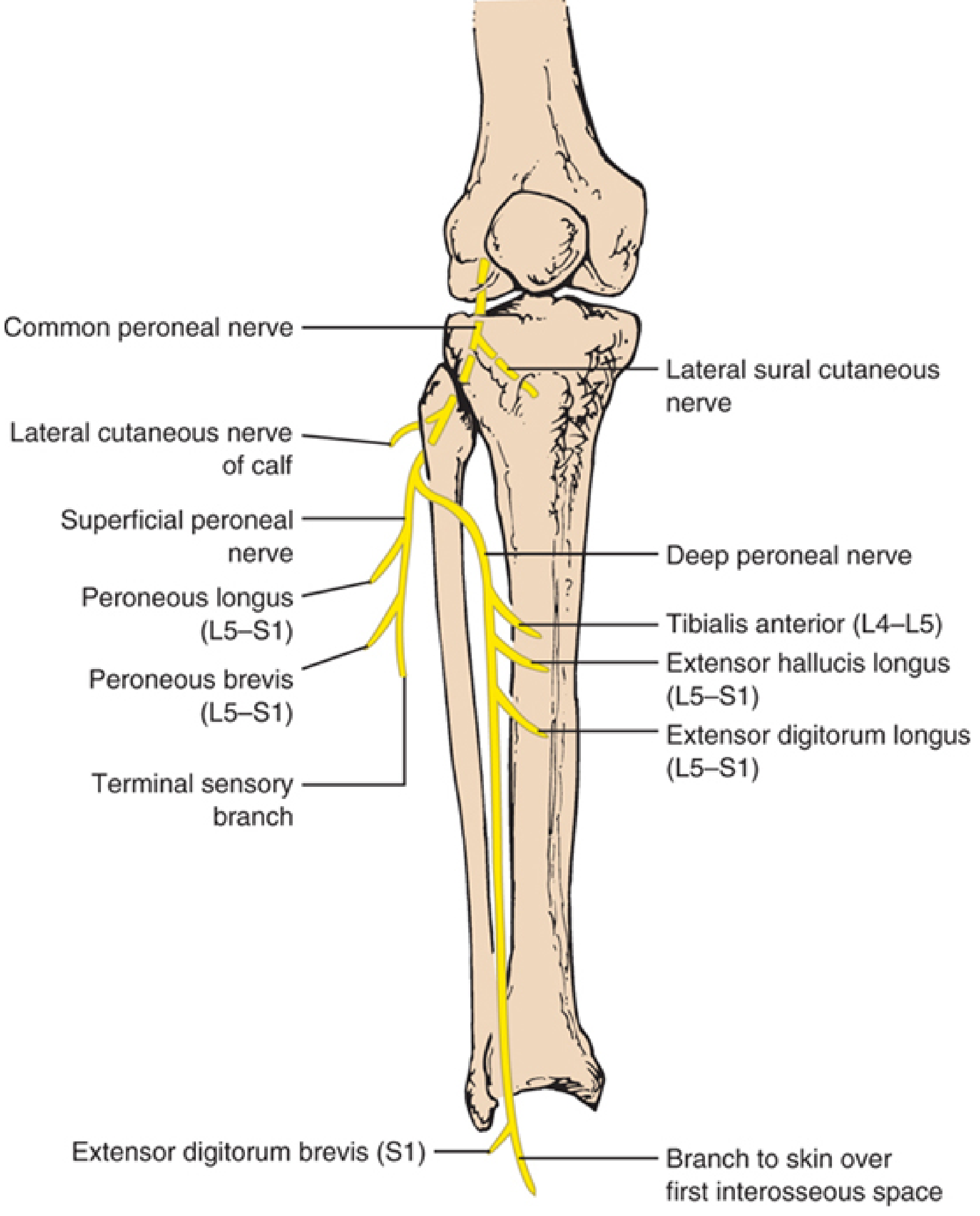
The Common Peroneal (Fibular) Nerve
- Origin: Terminal branch of sciatic nerve (L4, L5, S1, S2)
- Course: Descends in popliteal fossa → winds around the neck/head of fibula (most vulnerable point) → enters peroneus longus muscle → divides into two terminal branches
Two Terminal Branches:
A. Deep Peroneal Nerve (Anterior Tibial Nerve)
Supplies the dorsiflexors - the muscles lost in foot drop:
| Muscle | Root | Function | Test |
|---|---|---|---|
| Tibialis Anterior | L4-L5 | Dorsiflexion + inversion | Heel walking; resist dorsiflexion |
| Extensor Hallucis Longus (EHL) | L5-S1 | Extension of big toe + dorsiflexion | Dorsiflex big toe against resistance |
| Extensor Digitorum Longus (EDL) | L5-S1 | Extension of 4 toes + dorsiflexion | Dorsiflex toes against resistance |
| Extensor Digitorum Brevis (EDB) | L5-S1 | Extension of toes | Dorsiflex proximal phalanges |
| Peroneus Tertius | L5-S1 | Dorsiflexion + eversion | Part of EDL |
Sensory: Only the first web space (skin between first and second toes)
B. Superficial Peroneal Nerve
Supplies the evertors:
| Muscle | Root | Function | Test |
|---|---|---|---|
| Peroneus Longus | L5-S1 | Plantarflexion + eversion | Evert foot against resistance |
| Peroneus Brevis | L5-S1 | Plantarflexion + eversion | Evert foot against resistance |
Sensory: Lateral two-thirds of leg + dorsum of foot (EXCEPT first web space)
Key Point: Complete common peroneal palsy = foot drop + loss of eversion + sensory loss over lateral leg and dorsum of foot (except sole which is tibial nerve territory).
3. GAIT IN FOOT DROP - STEPPAGE GAIT
In foot drop, the patient cannot lift the foot during the swing phase. The foot would drag on the floor. To compensate:
Steppage Gait (High-Stepping Gait):
- Exaggerated hip and knee flexion during swing phase
- Raises the leg higher than normal to prevent the foot dragging
- Foot "slaps" down on heel strike
- Characteristic "slap" sound with each step
- May also circumduct the leg to clear the foot
This is tested clinically by asking the patient to walk on their heels - they cannot do so on the affected side.
4. CAUSES - LEVEL-BY-LEVEL APPROACH (HIGH YIELD)
Organize causes by anatomical level. This is critical for exams.
Level 1: Cortical / Upper Motor Neuron
- Cerebral stroke (parasagittal cortical lesion - leg area)
- Brain tumor
- Cerebral palsy (spastic type)
- Multiple sclerosis
(Note: UMN foot drop has spasticity + brisk reflexes + extensor plantar - different from LMN)
Level 2: Spinal Cord
- Spinal cord injury / trauma
- Spinal cord compression (disc, tumor, abscess)
- Motor neuron disease (ALS)
- Transverse myelitis
Level 3: Nerve Root (L4-L5 Radiculopathy) ← VERY COMMON
- L4-L5 disc prolapse (most common spinal cause)
- L5 root compression by disc or osteophyte
- Cauda equina syndrome
- Key: L5 radiculopathy - also has back pain + dermatomal sensory loss over dorsum of foot
Level 4: Lumbosacral Plexus
- Lumbar plexopathy (diabetes, malignancy)
- Retroperitoneal hemorrhage
- Post-delivery (obstetric palsy - baby's head pressing on lumbosacral trunk)
Level 5: Sciatic Nerve
- Sciatic nerve palsy (deep injection in buttock - commonest iatrogenic cause in India)
- Hip dislocation / acetabular fractures
- Posterior surgical approach to hip
Level 6: Common Peroneal (Fibular) Nerve ← MOST COMMON PERIPHERAL CAUSE
This is the most common compressive neuropathy of the lower limb.
Causes at the fibular head (most common site):
- Compression (most frequent cause):
- Prolonged squatting - "strawberry picker's palsy", yoga foot drop
- Leg crossing - habitual leg crossers, especially after weight loss
- Cast or tight bandage at fibula head
- Bedridden patients - pressure on outer knee
- Intraoperative positioning (lateral decubitus, lithotomy position)
- Post-arthroplasty (TKA/THA) - "post-arthroplasty foot drop"
- Trauma:
- Proximal fibular fracture
- Knee dislocation (peroneal nerve injured in 25-45% of knee dislocations!)
- Tibial plateau fracture
- Laceration/penetrating injury
- Masses:
- Intraneural ganglion (from superior tibiofibular joint capsule) - underdiagnosed but treatable
- Baker cyst
- Ganglion cyst
- Osteochondroma
- Schwannoma
- Leprosy (common in India)
- Stretch injury - forced foot inversion + plantarflexion ("punter's palsy" in footballers)
- Weight loss - nerve becomes vulnerable without subcutaneous fat padding
Specific iatrogenic causes:
- TKA - retractor tip compressing nerve against proximal fibula (most common TKA nerve injury)
- THA - especially with valgus-flexion deformity correction
- Tibial osteotomy - EHL nerve supply at risk
Level 7: Anterior Compartment
- Anterior compartment syndrome - pressure necrosis of tibialis anterior and deep peroneal nerve
Level 8: Ankle (Anterior Tarsal Tunnel Syndrome)
- Compression of deep peroneal nerve under the inferior extensor retinaculum
- Causes: fractures, tight shoes, ankle sprain
- Only EDB affected; sensory loss only in first web space
Level 9: Muscle / Tendon
- Tibialis anterior tendon rupture
- Myopathies (rare)
- Scapuloperoneal syndromes
Level 10: Peripheral Neuropathies (Bilateral foot drop)
- Diabetes mellitus
- Charcot-Marie-Tooth disease (hereditary motor-sensory neuropathy)
- Alcohol neuropathy
- Lead poisoning
- Guillain-Barré syndrome
- Leprosy
5. CLINICAL FEATURES OF COMMON PERONEAL NERVE PALSY (Most Common Cause)
History:
- Inability to lift the foot/toes
- Foot drag while walking
- Frequent tripping/falling
- Numbness/tingling over dorsum of foot and lateral leg
- History of recent weight loss, leg crossing, prolonged squatting, trauma, surgery
Examination:
Motor (the key findings):
- Loss of dorsiflexion (ankle) - tibialis anterior
- Loss of toe extension (EHL, EDL)
- Loss of foot eversion (if whole common peroneal involved)
- Plantar flexion and inversion PRESERVED (tibial nerve intact)
- Wasting of anterior and lateral compartment muscles in chronic cases
Sensory:
- Loss over lateral leg (lower 2/3) and dorsum of foot
- First web space involved if deep peroneal involved
- Sole of foot NORMAL (tibial nerve territory) - this distinguishes it from sciatic nerve palsy
Reflexes:
- Ankle jerk (S1) PRESERVED (gastrocnemius-soleus is tibial nerve)
- Knee jerk normal
- Plantar response: normal (flexor)
Other findings:
- Foot rests in plantarflexion and inversion at rest (equinovarus posture)
- No inversion of foot on walking (tibialis posterior - tibial nerve - still works)
- Tinel's sign may be positive at fibular head
6. DISTINGUISHING FOOT DROP CAUSES - KEY DIFFERENTIAL POINTS
| Feature | Common Peroneal Palsy | L5 Radiculopathy | Sciatic Nerve Palsy |
|---|---|---|---|
| Inversion (Tibialis Posterior) | NORMAL | WEAK (L5 supplies TP too) | WEAK |
| Ankle jerk | Normal | Normal (L5-S1 root) | ABSENT (S1 tibial division) |
| Plantar flexion | Normal | Normal | WEAK |
| Sole sensation | Normal | Normal | LOST |
| Hamstrings | Normal | May be weak | WEAK |
| Back pain | Absent | Present (radicular) | Absent |
| EMG - Short head biceps femoris | Normal | Normal | Abnormal (this is key) |
| EMG - Tibialis posterior | Normal | Abnormal | Abnormal |
| Tinel at fibular head | Often positive | Negative | Negative |
Critical point for exams:
- Tibialis posterior (inversion) is spared in peroneal palsy but weak in L5 radiculopathy - this is the key distinguishing muscle
- Short head of biceps femoris is supplied by the common peroneal division of sciatic nerve in the thigh - if abnormal on EMG, lesion is ABOVE the fibular head (sciatic nerve), not at fibular head
7. EVALUATION / INVESTIGATIONS
Step 1: Clinical Localization
Examine to determine: UMN vs LMN, and what level of LMN.
Bedside tests:
- Walk on heels (tests dorsiflexion - will fail)
- Observe gait - steppage gait
- Test all muscles systematically (grade 0-5 MRC scale)
- Test sensation precisely
- Check reflexes
- Tinel sign at fibular head
- Spine examination (SLR, dermatomes)
Step 2: Electrodiagnostic Studies (Most Important Investigation)
Nerve Conduction Study (NCS):
- Tests deep and superficial peroneal motor and sensory responses
- Can demonstrate focal conduction block across fibular head
- Compare both sides
- Fibular motor amplitude recording tibialis anterior = best prognostic indicator
- Low/absent amplitude = axonal loss = poor prognosis
- Conduction block across fibula head = demyelination = good prognosis
Electromyography (EMG):
- Denervation (fibrillations, positive sharp waves) in peroneal-innervated muscles
- Key muscles to test:
- Tibialis anterior
- EHL, EDL, EDB
- Peroneus longus/brevis
- Short head of biceps femoris - if abnormal, lesion is in thigh/sciatic nerve
- Tibialis posterior - if abnormal, suggests L5 radiculopathy, NOT peroneal palsy
- Paraspinal muscles (L4-L5 level) - if abnormal, suggests radiculopathy
EMG timing matters:
- Fibrillations appear 2-3 weeks after nerve injury
- Early EMG (within days) only shows reduced/absent motor unit action potentials
- Repeat at 4-6 weeks for full picture
Step 3: Imaging
X-ray:
- Proximal fibula (fracture, tumor)
- Knee joint (dislocation, degenerative changes, osteochondroma at fibular head)
- Lumbar spine (disc space narrowing, osteophytes, spondylolisthesis)
MRI:
- MRI lumbar spine - for radiculopathy (disc herniation, spinal stenosis, tumor)
- MRI knee - for intraneural ganglion, Baker cyst, tumors, soft tissue masses at fibular head
- Cross-sectional area of nerve on MRI
- Better than ultrasound for spinal pathology
Ultrasound:
- Preferred imaging for fibular head lesions - slightly more accurate than MRI for compressive fibular neuropathies
- Shows thickened nerve (cross-sectional area >8 mm² is abnormal)
- Identifies intraneural ganglia, tumors, ganglia, Baker cysts
- Can identify involvement of anterior fascicles (deep peroneal fibers)
- Dynamic assessment possible
CT scan:
- For bony lesions (tumors, osteochondroma, fractures)
- CT myelogram if MRI contraindicated
Step 4: Blood Tests
- Blood glucose / HbA1c - diabetes
- ESR, CRP - inflammatory/infective causes
- Serum B12, folate - nutritional neuropathy
- Heavy metals (lead) - if occupational exposure
- Nerve biopsy - if hereditary neuropathy suspected (CMT)
8. COMPLETE vs INCOMPLETE FOOT DROP
| Feature | Incomplete | Complete |
|---|---|---|
| EMG/NCS | Partial denervation; some MUAPs present | Complete denervation |
| Partial motor recovery | Common (87% full recovery) | Less common (38% full recovery) |
| Management | Conservative first | Surgical exploration if no recovery |
(Campbell's Operative Orthopaedics data on knee dislocation peroneal nerve injuries)
9. TREATMENT
A. Non-Surgical (Conservative)
Immediate:
- Remove cause - remove tight cast, unpad the knee, change position of bed-bound patient
- For post-TKA peroneal palsy: Remove compressive dressings and flex the knee (reduces tension on nerve) - first treatment
- Protect foot from pressure sores
Orthotic support:
- AFO (Ankle-Foot Orthosis) - custom-made plastic AFO
- Holds foot in 90° or slight dorsiflexion
- Prevents equinus contracture
- Allows functional gait
- Used while awaiting nerve recovery
- Functional electrical stimulation (FES) - emerging option
Physiotherapy:
- Passive range-of-motion exercises (prevent contractures)
- Stretching of Achilles tendon
- Strengthening of partially active muscles
- Gait training with AFO
Medical:
- Treat underlying cause (control diabetes, treat leprosy, supplement B12)
- Nerve regeneration: no proven pharmacological agents
- Pain management for neuropathic pain
Wait for recovery:
- If nerve not cut: most palsies show return within 3 months (for neuropraxia)
- Axonotmesis: slower recovery, 1 mm/day nerve regeneration
- Watch for: Tinel sign advancing distally = progressing regeneration
B. Surgical
Indications:
- No recovery at 3 months + EMG showing no evidence of reinnervation
- Complete palsy with known structural cause (ganglion, tumor, entrapment)
- Persistent foot drop >1 year with no recovery
- Known transection (neurotmesis) - early repair
Surgical options:
1. Nerve decompression/exploration:
- For intraneural ganglia, fibular tunnel syndrome, entrapment
- Results: good for demyelinating lesions
2. Nerve repair / grafting:
- Direct end-to-end repair if gap small
- Sural nerve graft if large gap
- Best results within first 6 months
3. Neurolysis:
- Release of scar tissue around nerve
- For traction injuries
4. Tendon Transfer (Most important for established foot drop):
The goal is to restore active dorsiflexion when nerve recovery is not expected.
Most common transfer: Tibialis Posterior Tendon Transfer (TPTT)
- Tibialis posterior (tibial nerve, L4-L5) rerouted to dorsum of foot
- Transferred through interosseous membrane ("transmembranous route") to dorsum of foot
- Attached to mid-dorsum (third cuneiform / base of second metatarsal)
- Prerequisites:
- Tibialis posterior must be grade 4-5 strength
- Foot must be passively correctable
- Joint must be mobile
- TAL (Tendo-Achilles Lengthening) if equinus present
- Indication: Persistent foot drop >1 year with no neurological recovery
Other tendon transfers:
- Peroneus longus to dorsum
- EHL to dorsum (if hindfoot stable)
5. Arthrodesis (Ankle/Triple fusion):
- For rigid deformity with irreversible foot drop
- Provides stable plantigrade foot
- Triple arthrodesis (subtalar + talonavicular + calcaneocuboid) - for fixed equinovarus
- Lambrinudi's arthrodesis - special triple arthrodesis with dorsal wedge at talonavicular to correct foot drop passively
6. Functional electrical stimulation (FES)/neuroprosthesis:
- Implantable devices for irreversible cases
10. PROGNOSIS - KEY NUMBERS
| Situation | Prognosis |
|---|---|
| Neuropraxia (compressive) | Very good; recovery in days-weeks (3 months) |
| Incomplete common peroneal palsy (knee dislocation) | 87% full motor recovery |
| Complete common peroneal palsy (knee dislocation) | Only 38% full motor recovery |
| Axonotmesis | Recovery at rate of 1 mm/day (approx 1 inch/month) |
| Neurotmesis (transection) | Poor without surgical repair |
| Distal fibular motor amplitude (NCS) | Best prognostic indicator |
Rule: Acute demyelinating lesions - uniformly good prognosis. Axonal loss and stretch injuries - delayed and incomplete recovery.
11. POST-TKA / POST-THA FOOT DROP - SPECIAL SCENARIO
After TKA:
- Most common nerve injury after TKA
- Usually due to retractor tip compressing nerve against proximal fibula
- Also with valgus + flexion contracture correction
- Immediate management: Remove compressive dressings + FLEX THE KNEE
- Most recover within 3 months if nerve not cut
- If no recovery at 3 months: EMG/NCS → explore and decompress
After THA:
- Peroneal division of sciatic nerve most at risk (because it has less movement capacity)
- Risk factors: cementless prosthesis, revision surgery, leg lengthening >2.7 cm
- Immediate management: flex hip, flex knee (reduce tension on sciatic nerve)
12. KEY EXAM SUMMARY TABLE
| Fact | Answer |
|---|---|
| Most common cause of foot drop | L4-L5 disc prolapse (spinal) / Common peroneal nerve palsy (peripheral) |
| Most common compressive neuropathy of lower limb | Common peroneal nerve at fibular head |
| Gait in foot drop | Steppage gait (high-stepping gait) |
| Muscle that distinguishes peroneal palsy from L5 root | Tibialis posterior (weak in L5 root, normal in peroneal palsy) |
| Sole sensation in peroneal palsy | Normal (tibial nerve) |
| Ankle jerk in peroneal palsy | Normal (S1, tibial nerve) |
| Best EMG prognostic indicator | Fibular motor amplitude recording tibialis anterior |
| Immediate treatment post-TKA peroneal palsy | Remove compressive dressings + flex the knee |
| Gold standard AFO for foot drop | Custom-made plastic ankle-foot orthosis |
| Best tendon transfer for established foot drop | Tibialis posterior tendon transfer (transmembranous route) |
| Prerequisite for TPTT | TP muscle strength grade 4-5; passive correctability |
| Recovery rate of complete peroneal palsy post knee dislocation | Only 38% full recovery |
| EMG timing for denervation changes | 2-3 weeks after injury |
| Nerve crossing at fibular head - surgical landmark | 10-12 cm below knee joint; wraps around fibular neck in peroneus longus origin |
| "Strawberry picker's palsy" | Peroneal palsy from prolonged squatting |
| "Punter's palsy" | Peroneal palsy from forced foot inversion in football |
| Intraneural ganglion source | Superior tibiofibular joint capsule disruption |
Sources:
- Localization in Clinical Neurology 8th Edition - comprehensive nerve anatomy and lesion localization
- Bradley and Daroff's Neurology in Clinical Practice - differential diagnosis and electrodiagnostics
- Campbell's Operative Orthopaedics 15th Ed 2026 - surgical management and TKA peroneal palsy
- Miller's Review of Orthopaedics 9th Ed - gait analysis and classification
- Gray's Anatomy for Students - anatomy of common fibular nerve
In detail about management of claw hand for Orthopaedic postgraduate exam
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive data. Let me compile the complete orthopaedic PG exam answer on claw hand management.
Management of Claw Hand - Complete Orthopaedic PG Exam Guide
1. DEFINITION
Claw hand (intrinsic-minus hand) is a deformity characterized by:
- Hyperextension at the metacarpophalangeal (MCP) joints
- Flexion at the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints
It results from paralysis of the intrinsic muscles of the hand (lumbricals and interossei), with the long flexors and extensors acting unopposed.
2. ANATOMY - WHY THE CLAW FORMS (The Key Concept)
To understand claw hand, you must understand the balanced action of intrinsics vs extrinsics.
Normal Intrinsic Function:
The lumbricals and interossei do two things:
- Flex the MCP joint (via their insertion into the volar plate/flexor aspect)
- Extend the PIP and DIP joints (via their insertion into the lateral bands of the extensor hood)
What happens when intrinsics are paralyzed:
| Muscle group | Action lost | Result |
|---|---|---|
| Interossei + Lumbricals lost | MCP flexion lost | Long extensors (EDC) hyperextend MCP |
| Interossei + Lumbricals lost | PIP/DIP extension lost | Long flexors (FDP, FDS) flex PIP and DIP |
Result: MCP hyperextension + PIP/DIP flexion = CLAW posture
The "Paradox of Ulnar Clawing" - High vs Low Lesion:
Low ulnar nerve palsy → MORE clawing (ring + little fingers)
High ulnar nerve palsy → LESS clawing (ring + little fingers)
Why? In high ulnar palsy, FDP (ring + little) is also paralyzed → cannot flex the PIP/DIP → less claw. This is the "ulnar paradox".
3. CAUSES OF CLAW HAND
A. Ulnar nerve palsy (Most common cause)
- Ring + little fingers only (ulnar 2 fingers)
- Why? Lumbricals to ring and little fingers = ulnar nerve. Lumbricals to index and middle = median nerve
- Degree of clawing: Ring > little (lumbrical to index/middle fingers partially corrects by median nerve)
B. Combined median + ulnar nerve palsy
- All four fingers involved
- Called "complete intrinsic minus hand" or "ape hand" + claw combined
C. Leprosy (Hansen's disease)
- Most common cause in India
- Ulnar nerve affected at elbow → ulnar claw
- Combined median + ulnar involvement = all finger clawing
- May have fixed contractures
D. Volkmann's ischemic contracture (severe form)
- Post-compartment syndrome
- Intrinsic-minus or claw hand deformity
- Fibrotic muscles, contractures
E. Rheumatoid arthritis
- Intrinsic muscle tightening → intrinsic-plus deformity (opposite) OR
- Intrinsic atrophy from nerve involvement → claw pattern
F. Cerebral palsy / Spastic conditions
- UMN type - different from true claw (has spasticity)
G. Charcot-Marie-Tooth disease
- Hereditary motor-sensory neuropathy
- Progressive clawing of all fingers
4. CLINICAL ASSESSMENT - THE EXAMINATION SEQUENCE
Inspection:
- Which fingers are clawed? (Ulnar 2 only? All 4?)
- Degree of clawing (mild to severe)
- Wasting of interosseous spaces (hollowing of dorsal web spaces)
- Hypothenar wasting (ulnar palsy)
- Thenar wasting (median palsy)
- Skin changes - anaesthetic skin, ulcers, scars (leprosy)
Assessment of deformity:
Is the deformity FLEXIBLE or FIXED?
- Flexible: can passively correct MCP hyperextension → surgical candidate
- Fixed: contractures present → needs preliminary treatment before tendon transfer
Key Clinical Tests:
1. Bouvier's Test (Most Important for Surgical Planning)
Purpose: Determines if the extensor mechanism (lateral bands) is competent.
How to do: Manually block (prevent) hyperextension of the MCP joint and ask patient to actively extend the PIP joint.
Interpretation:
| Result | Meaning | Treatment implication |
|---|---|---|
| Bouvier POSITIVE = PIP extends when MCP blocked | Extensor mechanism is competent | Static procedure alone sufficient (e.g., Zancolli capsulodesis) |
| Bouvier NEGATIVE = PIP cannot extend even when MCP blocked | Extensor mechanism is incompetent | Dynamic procedure needed (active tendon transfer) |
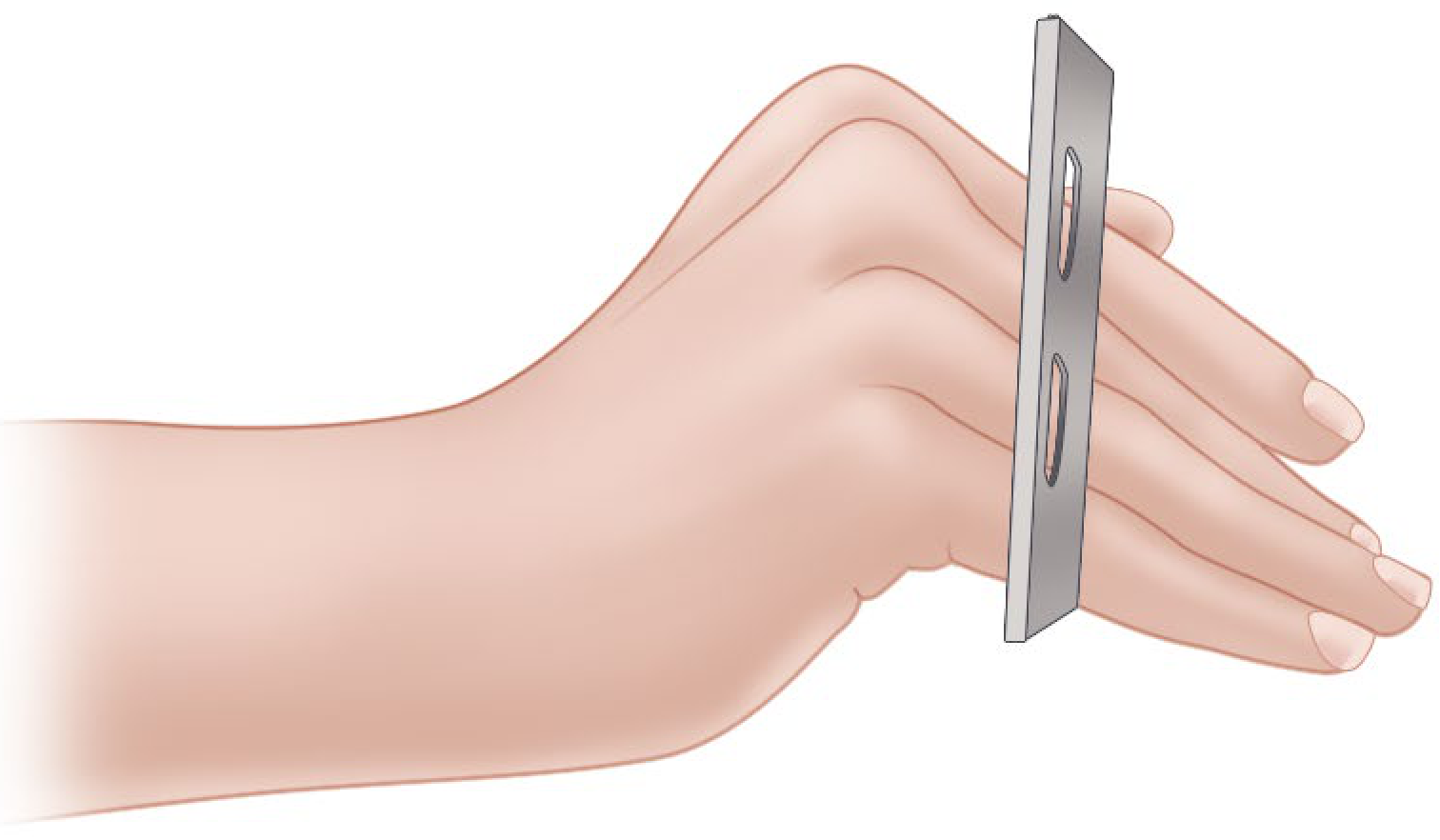
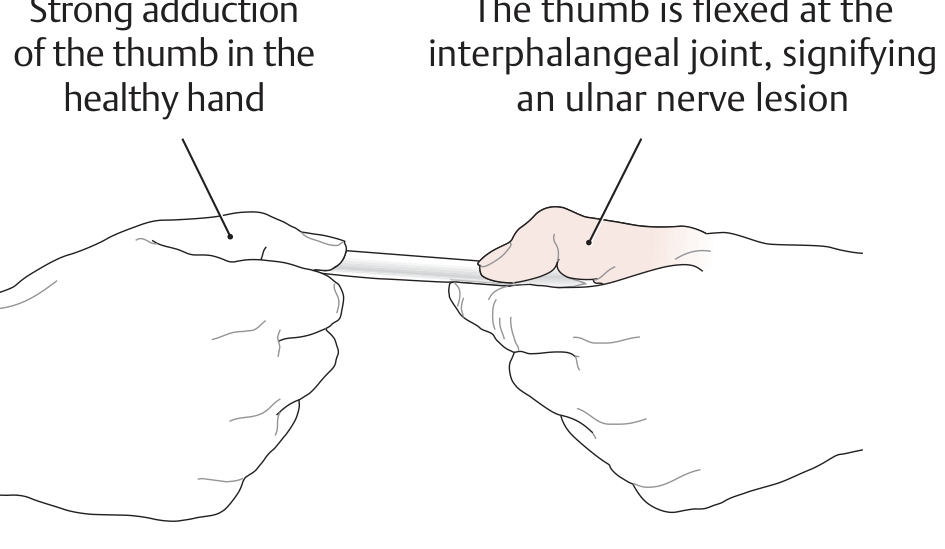
2. Froment's Sign (for adductor pollicis weakness in ulnar palsy)
- Ask patient to hold a flat object between thumb and index finger
- In ulnar palsy: adductor pollicis paralyzed → compensates by flexing thumb IP joint using FPL (median nerve)
- Positive: IP joint flexes during pinch → FPL compensating
3. Assessment of passive correctability:
- Can you passively flex the MCP and extend the PIP? → Prerequisite for tendon transfer
- If NOT passively correctable → splinting first, or PIP arthrodesis
4. Muscle testing (MRC grading 0-5):
- Test all intrinsic muscles: interossei (abduction/adduction), lumbricals
- Test extrinsic muscles: FDP, FDS, FPL, EPL, EDC
5. Sensory assessment:
- Two-point discrimination, monofilament testing
- Maps distribution (ulnar half of ring + entire little finger = ulnar nerve)
5. PRINCIPLES OF MANAGEMENT
The overall management strategy follows three steps:
Step 1: Treat the cause (if possible)
- Nerve repair/decompression if nerve injury is recent and accessible
- Leprosy treatment (MDT - multidrug therapy)
- Release of entrapment (cubital tunnel release for ulnar nerve)
- If nerve can recover → wait for recovery (up to 18-24 months)
Step 2: Prevent/correct contractures (Splinting)
- Lively/dynamic splints - hold MCP in slight flexion to prevent fixed hyperextension contracture
- Preserve passive range of motion
- Prerequisites before any tendon transfer:
- Passive MCP flexion must be possible
- Passive PIP extension must be possible
- Skin must be healthy, no ulcers
Step 3: Surgical correction (Tendon transfers or static procedures)
6. SURGICAL MANAGEMENT - DETAILED
The Goal of Surgery:
To restore MCP flexion (and PIP/DIP extension) while preserving grip and pinch function.
Surgery is planned based on:
- Bouvier's test result → static vs dynamic
- Available muscles (not paralyzed, grade 4+, expendable)
- Pattern of nerve palsy (ulnar only vs combined)
- Passive correctability of joints
A. STATIC PROCEDURES
(Used when Bouvier's test is POSITIVE - extensor mechanism intact)
1. Zancolli Capsulodesis (Most Important Static Procedure)
Principle: Tighten the volar plate of the MCP joint to create a 10-30° flexion contracture at the MCP → prevents hyperextension → allows long extensors to work on IP joints.
Technique:
- Transverse incision in palm at distal palmar crease
- Expose flexor tendon sheaths at each MCP joint
- Retract flexor tendons → expose MCP volar plate
- Resect an elliptical segment of the volar fibrocartilaginous plate (or advance it proximally)
- Close volar plate with non-absorbable sutures → creates MCP flexion contracture of 10-30°
- K-wires to maintain position if needed
- Dorsal splint with MCP in flexion + wrist in extension
Post-op: Cast for 3 weeks → then MCP exercises
Advantage: Simpler; no donor muscle sacrifice
Limitation: Does NOT restore grip strength; only corrects clawing
2. Fowler Tenodesis
Principle: A tendon graft looped through extensor retinaculum acts as a passive tenodesis - when wrist flexes, tension on graft passively extends IP joints.
- Activated by wrist flexion (passive, not active)
- Not useful in patients with wrist flexion weakness
3. Riordan Tenodesis
Principle: ECRB and ECU tendons cut in half at midforearm (distal insertion intact), split ends passed through lumbrical canals to radial finger.
- NOT activated by wrist motion (unlike Fowler)
4. Bone Block (Mikhail)
- Dorsal bone block at MCP joint prevents hyperextension
- Rarely used
5. MCP Joint Arthrodesis
- For severe, irreversible cases
- Sacrifices motion
B. DYNAMIC PROCEDURES
(Used when Bouvier's test is NEGATIVE - extensor mechanism incompetent)
(Also when grip strength restoration is needed)
These are tendon transfers - redirect an expendable functioning muscle to restore intrinsic function.
The Route of Transfer
All transfers pass through the lumbrical canal (volar to the deep transverse metacarpal ligament) and attach to the radial side of the lateral band of the extensor aponeurosis.
Why radial side? Attaching to the radial lateral band corrects both clawing AND restores MCP flexion with IP extension in the correct direction.
1. Modified Stiles-Bunnell Procedure
Donor: FDS (flexor digitorum superficialis) of ring or middle finger
Route: Through lumbrical canal → radial lateral band of finger
Key: One FDS can be split into four tails for all four fingers
Problem with original Bunnell (all FDS tendons): Too strong → PIP hyperextension = intrinsic-plus deformity (opposite of claw)
Modification: Use only ONE FDS split into 4 tails → reduces this risk
Insertion sites (in order of preference - decreasing intrinsic-plus risk):
- Into bone at base of proximal phalanx (safest)
- Into flexor sheath
- Into lateral band (highest risk of intrinsic-plus)
2. Zancolli Lasso Procedure
Donor: FDS (of the clawed finger itself)
How it works:
- FDS tendon is divided distally
- Passed through a slit in the flexor pulley sheath just distal to the MCP joint
- Looped back and sutured to itself
- Creates a dynamic block - when FDS contracts, it flexes the MCP
- Technically a dynamic transfer because FDS is still a functioning muscle-tendon unit
Advantage: Simple, elegant, preserves the original FDS in its original position
Indication: Very commonly used in low ulnar palsy when FDS is intact
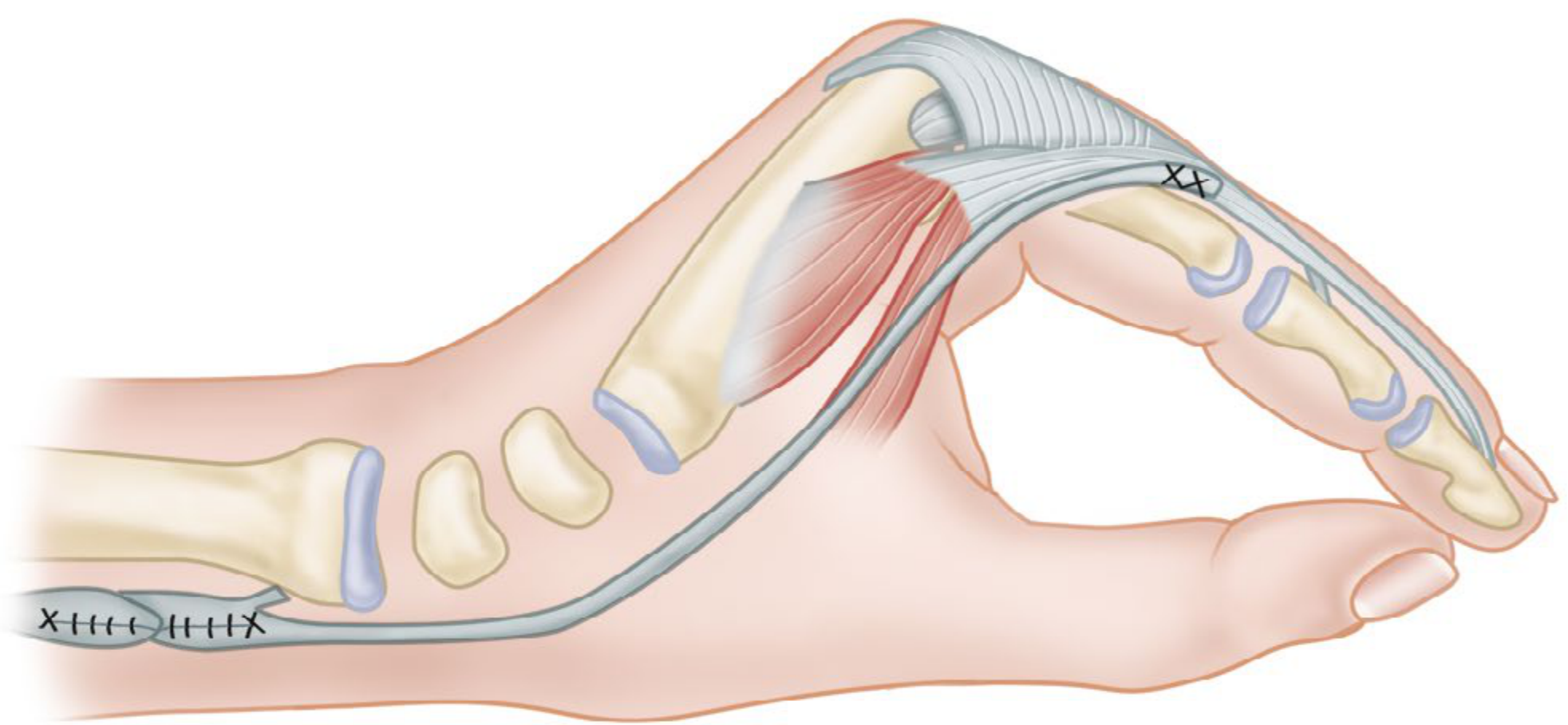
3. Brand Transfer (Paul Brand - Leprosy surgeon)
Donor: ECRB (extensor carpi radialis brevis) extended by plantaris tendon graft
Route: Through interosseous spaces → lumbrical canals → radial lateral band
Two techniques:
- Palmar route (through carpal tunnel): Passes under palmar ligaments
- Dorsal route (through interosseous spaces): More common, safer for median nerve
Advantage: Powerful transfer; restores grip strength well
Disadvantage: Reeducation difficult; may compress median nerve (palmar route)
Useful in leprosy/combined nerve palsies where FDS is unavailable
4. Riordan Transfer (FCR-based)
Donor: FCR (flexor carpi radialis) passed radially + extended with tendon graft (plantaris)
Route: Through lumbrical canals → radial lateral band
Note: Useful if patient has strong wrist flexion (which weakens Bunnell/intrinsic transfers)
5. Fowler Transfer (Riordan modification - most commonly tested)
Donor: EIP (extensor indicis proprius) + EDQ (extensor digiti quinti)
Riordan modification: EIP to ring/little fingers; Palmaris longus (extended with graft) to index/middle
Passed: Volar to deep transverse metacarpal ligament → radial lateral band
Advantage: Available even in combined nerve palsies (radial nerve preserved)
C. COMBINED NERVE PALSIES
Low Median + Low Ulnar Palsy (at wrist)
- All four fingers clawed + thumb opposition + adduction lost
- Clawing: Brand transfer (ECRB with graft) - best option
- Opposition: Riordan transfer (FCR-based)
- Thumb adduction: EIP through third intermetacarpal space to adductor insertion
Prerequisites: Must first correct any thumb web contracture and joint contractures.
High Median + High Ulnar Palsy (above elbow)
- FDS, FDP (all fingers), all intrinsics, thenar, hypothenar all paralyzed
- Only radial nerve muscles available for transfer
- Treatment:
- Arthrodesis of thumb MCP joint
- Zancolli capsulodesis of all MCP joints (for clawing)
- ECRL transfer for finger flexion
- ECRB for thumb and finger extension
7. SPECIAL CONSIDERATIONS
Leprosy Claw Hand Management
- Most important message: Prevent the claw from becoming FIXED
- Use dynamic splints early during active nerve inflammation
- Prednisolone for acute leprous neuritis (reduces nerve damage)
- Once deformity is fixed → surgical correction
Surgery in leprosy:
- If disease is inactive and joints are mobile:
- Brand transfer or Riordan transfer
- If skin is anaesthetic: Extra care to avoid pressure ulcers post-surgery
- Thumb: Opponensplasty for opposition loss (median nerve)
Post-Volkmann's Ischemic Contracture
- Claw hand from intrinsic fibrosis
- Treatment:
- Muscle slide (origin release of intrinsic muscles) for early/mild cases
- Tendon lengthening
- Limited goals; contracture releases improve function partially
8. PREREQUISITES FOR TENDON TRANSFER
Before any transfer surgery, all must be present:
- Passive correctability - MCP must flex passively, PIP must extend passively
- Donor muscle grade 4-5 MRC strength (will lose 1 grade after transfer)
- Stable skeletal framework - no untreated fractures
- Good soft tissue cover - no active infection, healing scars
- Patient motivation + compliance for rehabilitation
- Joint contractures corrected first (by splinting or surgery)
- If nerve can still recover - wait at least 18-24 months before tendon transfer
9. SUMMARY TABLE - PROCEDURES AT A GLANCE
| Procedure | Type | Donor | Best for |
|---|---|---|---|
| Zancolli Capsulodesis | Static | Volar plate | Bouvier +ve; simple claw |
| Zancolli Lasso | Dynamic | FDS (same finger) | Low ulnar; FDS intact |
| Modified Stiles-Bunnell | Dynamic | FDS (ring/middle) | All 4 fingers |
| Brand Transfer | Dynamic | ECRB + plantaris graft | Leprosy; combined palsy |
| Riordan Transfer | Dynamic | FCR + graft | Strong wrist flexors |
| Fowler/Riordan modification | Dynamic | EIP + EDQ | Radial nerve only available |
| Fowler Tenodesis | Static | Tendon graft from retinaculum | Passive correction |
10. KEY EXAM POINTS SUMMARY
| Fact | Answer |
|---|---|
| Most common cause of claw hand | Ulnar nerve palsy |
| Which fingers in ulnar palsy | Ring and little (ulnar 2) |
| Why index and middle less clawed | Lumbricals 1 and 2 supplied by median nerve |
| Ulnar paradox | High ulnar palsy = LESS claw (FDP also paralyzed) |
| Most important pre-op test | Bouvier's test |
| Bouvier positive → | Static procedure sufficient (Zancolli capsulodesis) |
| Bouvier negative → | Dynamic procedure needed (tendon transfer) |
| Route of all intrinsic replacements | Volar to deep transverse metacarpal ligament → radial lateral band |
| Simplest static procedure | Zancolli capsulodesis |
| Best transfer when only radial nerve intact | Fowler transfer (EIP + EDQ) |
| Best transfer in leprosy/combined palsy | Brand transfer (ECRB + plantaris graft) |
| Complication of Bunnell transfer | Intrinsic-plus deformity (PIP hyperextension) |
| Sign of adductor pollicis weakness | Froment's sign |
| Dose FDS gives 1 grade loss | Yes - always plan for grade 4+ donor |
| India most common cause of claw | Leprosy (Hansen's disease) affecting ulnar nerve at elbow |
Sources:
- Campbell's Operative Orthopaedics 15th Edition 2026 - Chapter 76 (Tendon transfers, intrinsic reconstruction)
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System - Ulnar nerve lesions
- Miller's Review of Orthopaedics 9th Edition - Hand surgery
This is a shared conversation. Sign in to Orris to start your own chat.