10 common heart diseases with ecg changes and 10 ecg those images
Reading File
Finding Sources
Searching Images
ECG electrocardiogram myocardial infarction ST elevation
Searching the Web
10 common heart diseases ECG changes electrocardiogram findings
Searching Images
atrial fibrillation ECG irregularly irregular rhythm no P waves
Searching Images
ventricular tachycardia ECG wide QRS tachycardia
Searching Images
complete heart block third degree AV block ECG dissociation
Searching Images
Wolff-Parkinson-White syndrome ECG delta wave short PR
Searching Images
pericarditis ECG saddle shaped ST elevation diffuse
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain
Searching Images
hypertrophic cardiomyopathy ECG left ventricular hypertrophy
Searching Images
left bundle branch block LBBB ECG broad notched QRS
Searching Images
long QT syndrome ECG prolonged QT interval torsades
I now have excellent ECG images for all 10 conditions. Let me compile the comprehensive answer:
10 Common Heart Diseases with ECG Changes
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
Mechanism: Complete occlusion of a coronary artery → transmural ischemia
ECG Changes:
- Convex ("tombstone") ST elevation ≥1 mm in ≥2 contiguous limb leads or ≥2 mm in precordial leads
- Hyperacute T-waves (tall, peaked) — earliest sign
- Reciprocal ST depression in opposite leads
- Pathological Q waves (>25% of R wave height, >40 ms wide) develop hours later
- T-wave inversion in the evolutionary phase
Localisation:
| Territory | Leads with ST elevation |
|---|---|
| Anterior (LAD) | V1–V4 |
| Inferior (RCA) | II, III, aVF |
| Lateral (LCx) | I, aVL, V5–V6 |
| Posterior | Tall R in V1-V2 + ST depression V1–V3 |
ECG Image — Anterior STEMI (LAD occlusion):
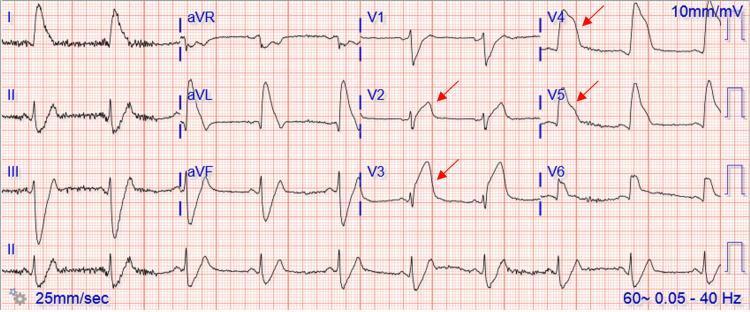
Tombstone ST-elevation in V2–V5 with reciprocal depression in II, III, aVF — proximal LAD occlusion.
2. 🫀 Inferolateral STEMI
ECG Changes:
- ST elevation in II, III, aVF and V4–V6
- Reciprocal ST depression in I, aVL, V2–V3
ECG Image — Inferolateral STEMI:
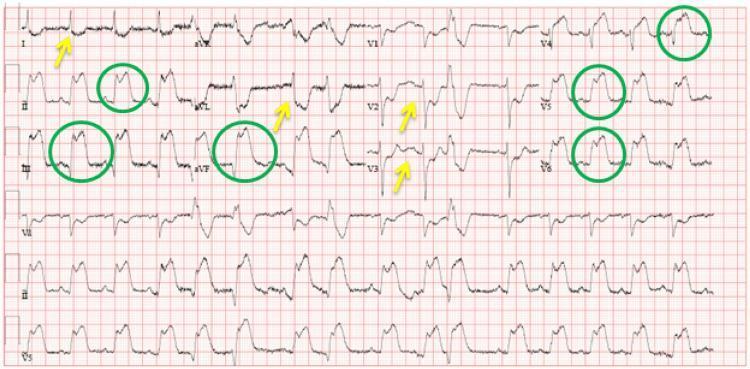
ST elevation (green circles) in inferior and lateral leads; reciprocal changes (yellow arrows) in I, aVL, V2–V3.
3. 🫀 Atrial Fibrillation (AF)
Mechanism: Chaotic, disorganized atrial electrical activity → no coordinated atrial contraction
ECG Changes:
- Absent P waves replaced by fibrillatory (f) waves (chaotic baseline)
- Irregularly irregular R-R intervals — the hallmark
- Narrow QRS complexes (unless aberrant conduction)
- Ventricular rate 60–180 bpm depending on AV node conduction
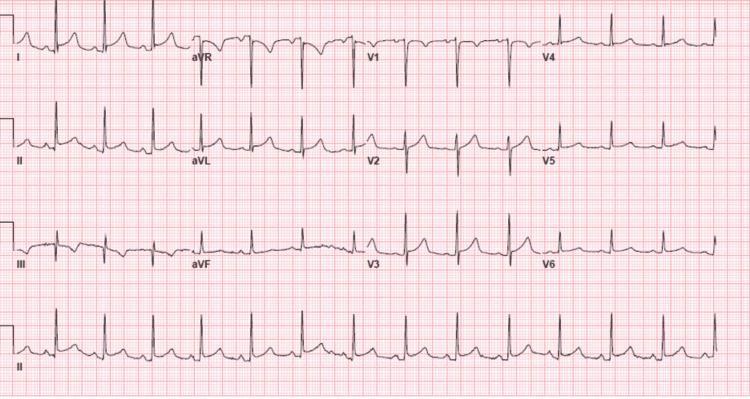
ECG Image — Atrial Fibrillation:
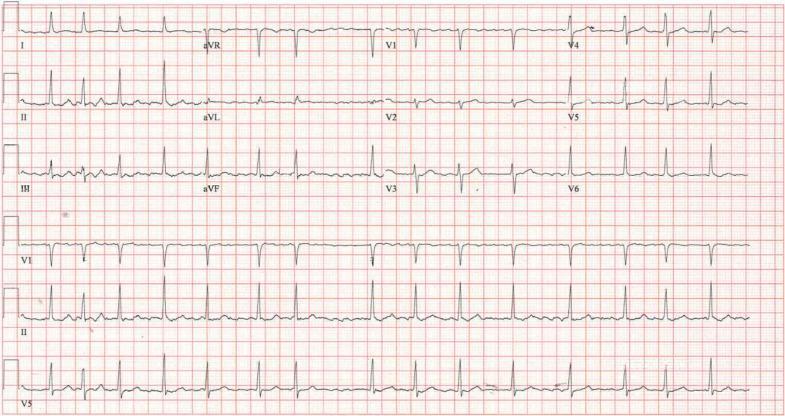
Classic AF: absent P waves, fine fibrillatory baseline (best seen in V1), irregularly irregular QRS intervals.
4. 🫀 Ventricular Tachycardia (VT)
Mechanism: Re-entrant circuit or triggered activity originating in the ventricles
ECG Changes:
- Wide QRS complexes (>120 ms), rate 100–250 bpm
- AV dissociation — P waves independent of QRS
- Fusion beats and capture beats (pathognomonic)
- Concordance across precordial leads (all positive or all negative)
- Brugada criteria / Vereckei algorithm used to confirm VT vs SVT with aberrancy
ECG Image — Monomorphic Ventricular Tachycardia:

Regular wide-complex tachycardia, superior axis, positive concordance V1–V6, no visible P waves — monomorphic VT.
5. 🫀 Complete (Third-Degree) AV Block
Mechanism: Total failure of conduction through the AV node or His-Purkinje system
ECG Changes:
- Complete AV dissociation — P waves and QRS complexes march independently
- P-P intervals regular; R-R intervals regular, but at different (slower) rates
- Ventricular escape rhythm: narrow QRS if junctional (40–60 bpm); wide QRS if ventricular (20–40 bpm)
- No relationship between P waves and QRS
ECG Image — Third-Degree Heart Block:
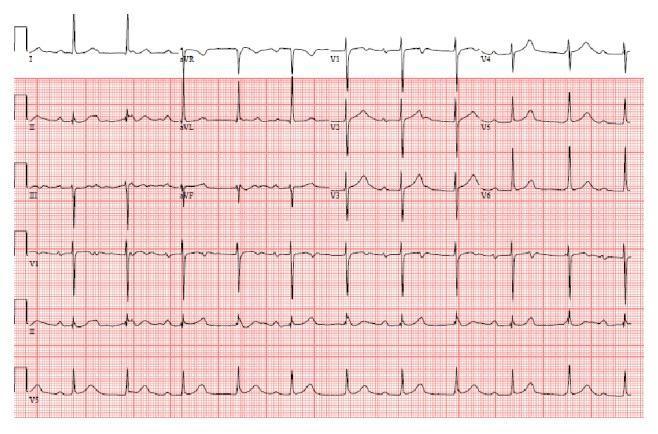
P waves "march through" the QRS complexes and T waves with no fixed PR relationship — complete heart block.
6. 🫀 Wolff-Parkinson-White (WPW) Syndrome
Mechanism: Accessory pathway (Bundle of Kent) bypasses the AV node → ventricular pre-excitation
ECG Changes (Pre-excitation Triad):
- Short PR interval (<120 ms)
- Delta wave — slurred upstroke of the QRS (initial slow ventricular activation via accessory pathway)
- Widened QRS (>120 ms) due to fusion of pre-excited and normally conducted impulses
- Secondary ST-T changes (discordant to QRS)
- Risk of AF with rapid conduction → VF (avoid AV nodal blockers)
ECG Image — WPW Syndrome:

Classic WPW triad: short PR interval, prominent delta waves (slurred QRS upstroke in II, III, aVF, V2–V6), and QRS widening.
7. 🫀 Acute Pericarditis
Mechanism: Pericardial inflammation irritates superficial epicardium → diffuse repolarization changes
ECG Changes (4 Stages):
- Stage 1 (acute): Diffuse concave ("saddle-shaped") ST elevation in all leads except aVR and V1; PR segment depression (highly specific); PR elevation in aVR
- Stage 2: ST normalizes, T waves flatten
- Stage 3: T-wave inversion
- Stage 4: Normalization
- Spodick's sign — downward sloping TP segment
Key differentiator from STEMI: Diffuse (multi-territory) ST elevation, PR depression, no reciprocal changes (except aVR)
ECG Image — Acute Pericarditis:
Diffuse saddle-shaped ST elevation with PR segment depression in II, III, aVF, V4–V6 and reciprocal PR elevation in aVR — classic Stage 1 pericarditis.
8. 🫀 Pulmonary Embolism (PE)
Mechanism: Acute right heart strain from increased pulmonary vascular resistance
ECG Changes:
- S1Q3T3 pattern — deep S in lead I, Q wave in lead III, T-wave inversion in lead III (classic but present in only ~20%)
- Sinus tachycardia — most common finding
- T-wave inversions V1–V4 (right ventricular strain pattern)
- Incomplete or complete RBBB
- Right axis deviation
- P pulmonale (tall peaked P in II) in severe cases
ECG Image — Pulmonary Embolism with S1Q3T3:

S1Q3T3 pattern annotated with circles/arrows: deep S in I, Q wave in III, T-wave inversion in III — sinus tachycardia with right heart strain.
9. 🫀 Hypertrophic Cardiomyopathy (HCM)
Mechanism: Asymmetric septal hypertrophy → abnormal depolarization/repolarization
ECG Changes:
- Left ventricular hypertrophy (LVH) voltage criteria: S in V1 + R in V5/V6 ≥35 mm (Sokolow-Lyon)
- "Giant" deep T-wave inversions in V3–V5 (especially in apical HCM / Yamaguchi syndrome)
- Deep Q waves in lateral leads (I, aVL, V5–V6) from septal depolarization
- ST depression with strain pattern
- Left axis deviation
- Short PR (sometimes)
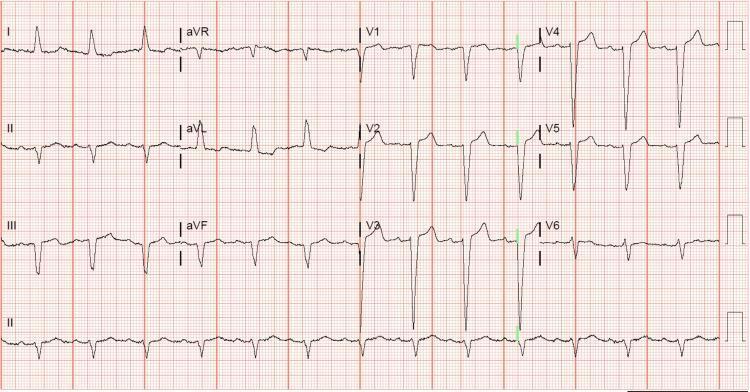
ECG Image — Hypertrophic Cardiomyopathy (Apical variant):
High-voltage QRS with deep, symmetric "giant" T-wave inversions V2–V5 — characteristic of apical HCM (Yamaguchi syndrome).
10. 🫀 Left Bundle Branch Block (LBBB)
Mechanism: Block in the left bundle branch → abnormal septal and LV activation (right-to-left)
ECG Changes (William: WiLLiaM mnemonic):
- Wide QRS (>120 ms)
- Broad, notched ("M-shaped") R wave in lateral leads I, aVL, V5, V6 — no septal Q waves
- Deep, broad rS or QS pattern in V1–V3
- Discordant ST-T changes (ST and T opposite to main QRS deflection)
- Left axis deviation
- New LBBB + chest pain = treat as STEMI equivalent (Sgarbossa criteria)
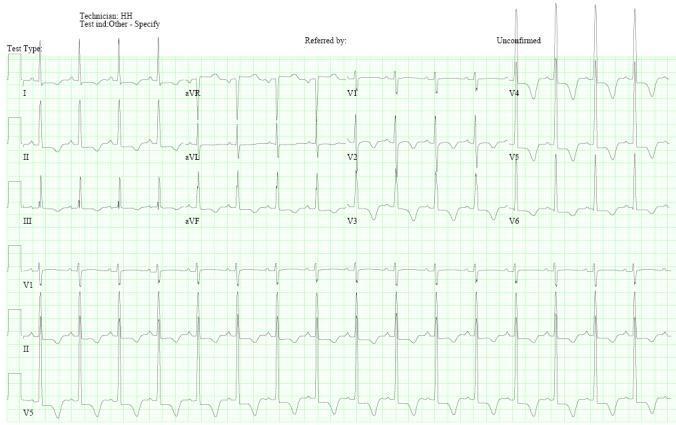
ECG Image — Left Bundle Branch Block:
Broad M-shaped R waves in V5–V6/I/aVL; deep S waves V1–V3; discordant ST-T changes — classic LBBB.
🔟 + Bonus: Long QT Syndrome (LQTS)
Mechanism: Impaired cardiac repolarization (channelopathy or drug-induced) → prolonged QT interval → risk of Torsades de Pointes (TdP) and sudden death
ECG Changes:
- Prolonged QTc (>440 ms men, >460 ms women) — calculated with Bazett formula: QTc = QT/√RR
- T-wave abnormalities: broad notched (LQT1), late-onset peaked (LQT2), small T with large U wave (LQT3)
- T-wave alternans in severe cases
- Triggers TdP — polymorphic VT with "twisting" QRS morphology
ECG Image — Long QT Syndrome with Torsades de Pointes:
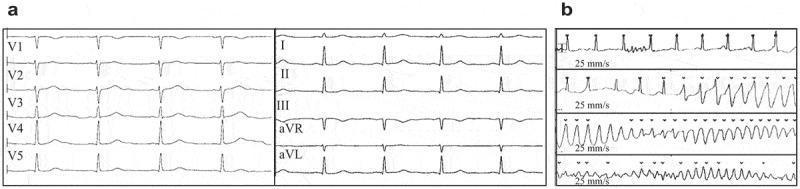
Panel (a): Prolonged QTc (478 ms) in sinus rhythm. Panel (b): Initiation of Torsades de Pointes — polymorphic VT with twisting QRS morphology around the isoelectric line.
Quick Reference Summary Table
| # | Disease | Key ECG Findings |
|---|---|---|
| 1 | Anterior STEMI | ST elevation V1–V4, reciprocal depression II/III/aVF, Q waves |
| 2 | Inferolateral STEMI | ST elevation II/III/aVF + V4–V6, reciprocal depression I/aVL |
| 3 | Atrial Fibrillation | Absent P waves, fine fibrillatory baseline, irregularly irregular QRS |
| 4 | Ventricular Tachycardia | Wide QRS >120ms, AV dissociation, concordance, rate 100–250 bpm |
| 5 | Complete Heart Block | P waves and QRS fully dissociated, slow escape rhythm |
| 6 | WPW Syndrome | Short PR <120ms, delta wave, wide QRS |
| 7 | Acute Pericarditis | Diffuse saddle ST elevation, PR depression, no reciprocal changes |
| 8 | Pulmonary Embolism | S1Q3T3, sinus tachycardia, T inversions V1–V4, RBBB |
| 9 | HCM | LVH voltage, giant T inversions V3–V5, deep lateral Q waves |
| 10 | LBBB | Wide QRS, notched R (I/aVL/V5–V6), deep S (V1–V3), discordant ST-T |
| +1 | Long QT Syndrome | QTc >440ms, T-wave morphology changes, Torsades de Pointes |
This is a shared conversation. Sign in to Orris to start your own chat.