Pigmented villonodular synovities in details according to cambell
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the information from Campbell's. Let me compile the complete detailed answer.
Pigmented Villonodular Synovitis (PVNS)
Campbell's Operative Orthopaedics, 15th Ed. (2026) - Chapter 30: Synovial Lesions
Overview / Classification
PVNS is a benign but locally aggressive synovial proliferative disorder that occurs in two distinct forms:
| Form | Also Known As | Key Feature |
|---|---|---|
| Localized | Focal nodular synovitis | Solitary pedunculated lesion |
| Diffuse | Classic PVNS | Involves entire synovium of the affected joint |
It is closely related to Giant Cell Tumor of Tendon Sheath (GCTTS) - the localized form is histologically identical to GCTTS; the diffuse form is also histologically identical but involves the entire joint synovium. Both are now increasingly classified under the umbrella term Tenosynovial Giant Cell Tumor (TSGCT).
Epidemiology & Clinical Presentation
- Typically presents with monoarticular pain and swelling
- Most common joint: Knee (by far the most frequent)
- Other joints affected: Hip, ankle, shoulder, wrist, and others
- Intraarticular lesions may cause mechanical symptoms (locking, clicking)
- A palpable mass may be present
- Symptoms are often nonspecific, leading to delayed diagnosis
- Joint aspiration characteristically reveals serosanguineous or blood-tinged fluid - a hallmark finding
Imaging
Plain Radiographs:
- Often normal in early or soft-tissue disease
- May show bony erosions, especially when the hip is involved
- No soft-tissue abnormality may be visible on plain films (see Figure 30.14 A & B below)
MRI - The Key Diagnostic Tool:
- Shows intraarticular masses that are dark on BOTH T1-weighted and T2-weighted sequences - this is the classic and virtually diagnostic MRI finding
- The hemosiderin deposition (from repeated hemorrhage into the joint) causes low signal on both T1 and T2 due to its paramagnetic properties
- MRI also delineates the full extent of the disease process
Figure 30.14 from Campbell's - Plain radiographs (A, B), T1-weighted sagittal MRI (C), T2-weighted axial MRI (D), and intraoperative photograph (E) of PVNS of the knee:
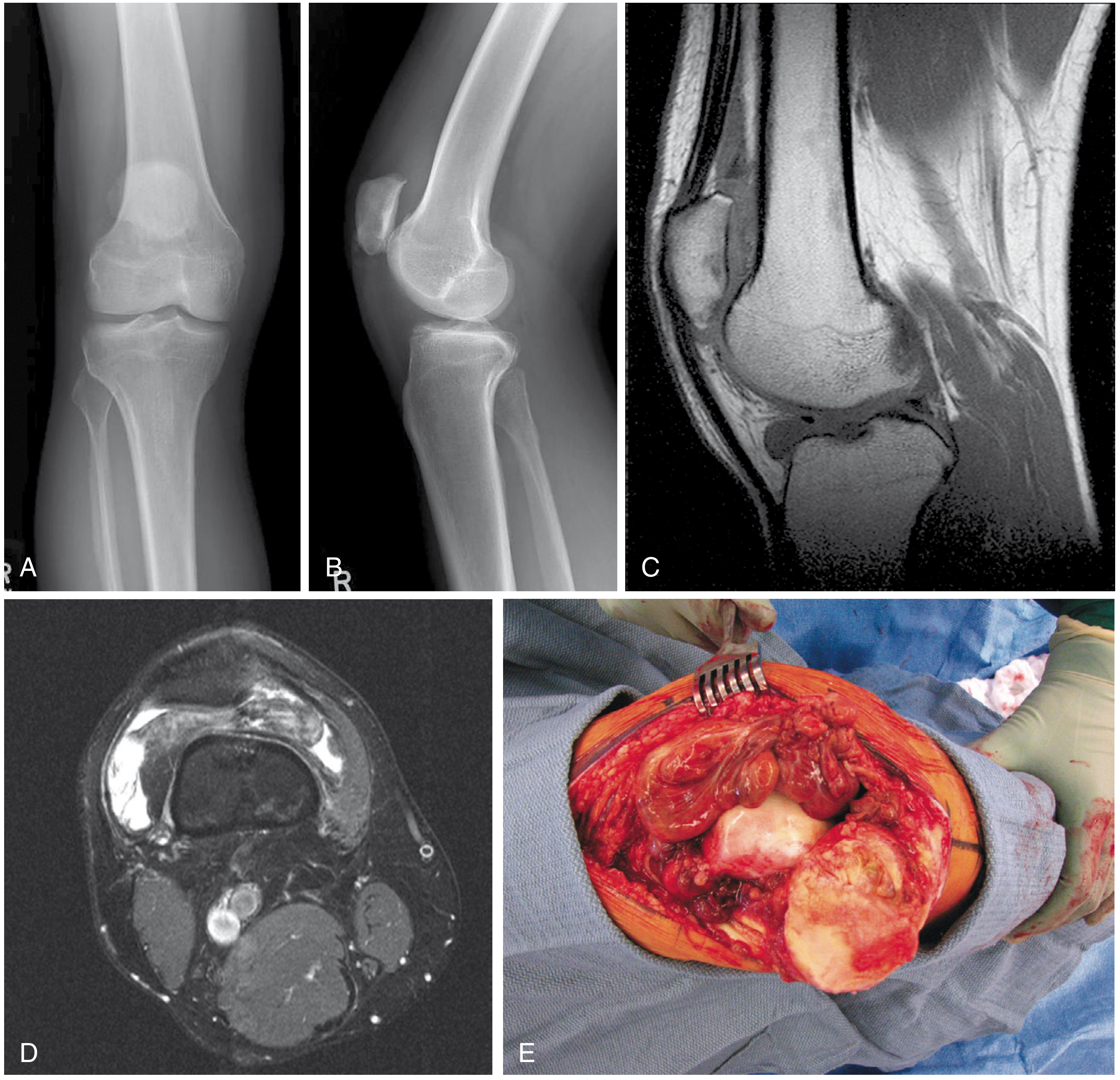
A & B: Plain radiographs show no soft-tissue abnormality. C: T1-weighted (sagittal) MRI - diffuse dark intraarticular process. D: T2-weighted (axial) MRI - also dark (hemosiderin). E: Intraoperative view of diffuse PVNS of the knee.
Histology
Localized form (Focal Nodular Synovitis):
- Solitary pedunculated lesion
- Histologically identical to Giant Cell Tumor of Tendon Sheath
Diffuse form:
- Also histologically identical to the localized form
- The distinction is that it involves the entire synovium of the affected joint
Microscopic features (Figure 30.13):
- Bland polyhedral (histiocyte-like) cells surrounded by collagen
- Giant cells (multinucleated)
- Hemosiderin deposits (the "pigmented" component, responsible for brown-yellow appearance)
- Foam cells (lipid-laden histiocytes)
- Low mitotic activity
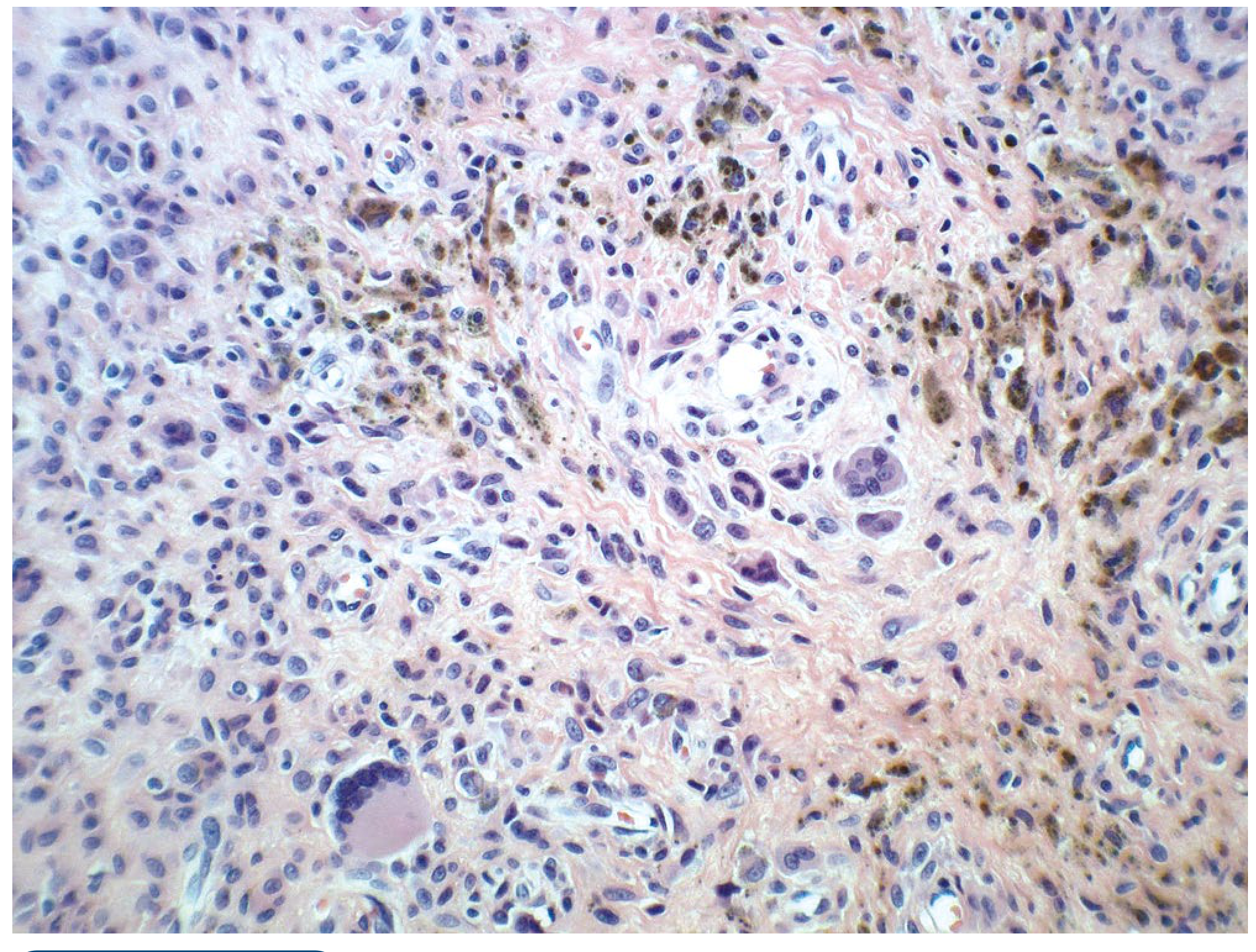
H&E ×20: Bland polyhedral cells with collagen stroma, multinucleated giant cells, and scattered hemosiderin deposits (brown granules).
Treatment
The three goals of treatment are:
- Alleviation of symptoms
- Minimizing recurrence
- Preservation of the joint
Localized Form
- Marginal excision is the recommended treatment
- Can frequently be treated by arthroscopic excision
- Reported recurrence rate with arthroscopic excision: 0% to 8%
Diffuse Form
- Total synovectomy is the recommended treatment (open or arthroscopic)
- Higher recurrence rates than the localized form
- Radiotherapy may be justified if surgery fails to control the disease process
Advanced / Refractory Disease
- If significant secondary degenerative changes of the joint surfaces have occurred, arthroplasty should be strongly considered
- Clinical trials are currently underway evaluating a potential role for CSF1R inhibitors (Colony Stimulating Factor 1 Receptor - targets the CSF1/CSF1R signaling pathway which drives synovial proliferation; pexidartinib is the approved CSF1R inhibitor)
Relationship to Adjacent Lesions (Campbell's Context)
Campbell's places PVNS within the Synovial Lesions chapter alongside:
| Lesion | Key Distinguishing Feature |
|---|---|
| Synovial chondromatosis | Cartilaginous metaplasia; multiple loose bodies; radiographically visible calcified loose bodies |
| Giant cell tumor of tendon sheath | Fingers/tendon sheaths; localized; histologically same as PVNS |
| PVNS | Joint synovium; hemosiderin; dark on T1 and T2 MRI |
Summary Table
| Feature | Detail |
|---|---|
| Nature | Benign synovial proliferative lesion |
| Forms | Localized (focal) vs. Diffuse |
| Most common joint | Knee; also hip, ankle, shoulder, wrist |
| Symptom | Monoarticular pain, swelling, mechanical symptoms |
| Joint fluid | Serosanguineous / blood-tinged |
| X-ray | Often normal; bony erosion (especially hip) |
| MRI hallmark | Dark on BOTH T1 and T2 (hemosiderin) |
| Histology | Bland polyhedral cells, giant cells, hemosiderin, foam cells |
| Localized Rx | Marginal/arthroscopic excision (recurrence 0-8%) |
| Diffuse Rx | Total synovectomy ± radiotherapy if refractory |
| End-stage joint | Arthroplasty |
| Emerging therapy | CSF1R inhibitors (e.g., pexidartinib) |
Source: Campbell's Operative Orthopaedics, 15th Edition (2026), Chapter 30 - Soft Tissue Tumors, Synovial Lesions section, pp. 1264-1268.
This is a shared conversation. Sign in to Orris to start your own chat.