Heyy Can you help me for my pathology exam
- Cell injury & death (necrosis, apoptosis)
- Inflammation (acute/chronic)
- Neoplasia (benign vs malignant, tumor markers)
- Specific organ pathology (heart, lung, kidney, liver, etc.)
- Hemodynamic disorders (thrombosis, embolism, infarction)
- Infectious diseases / immunopathology
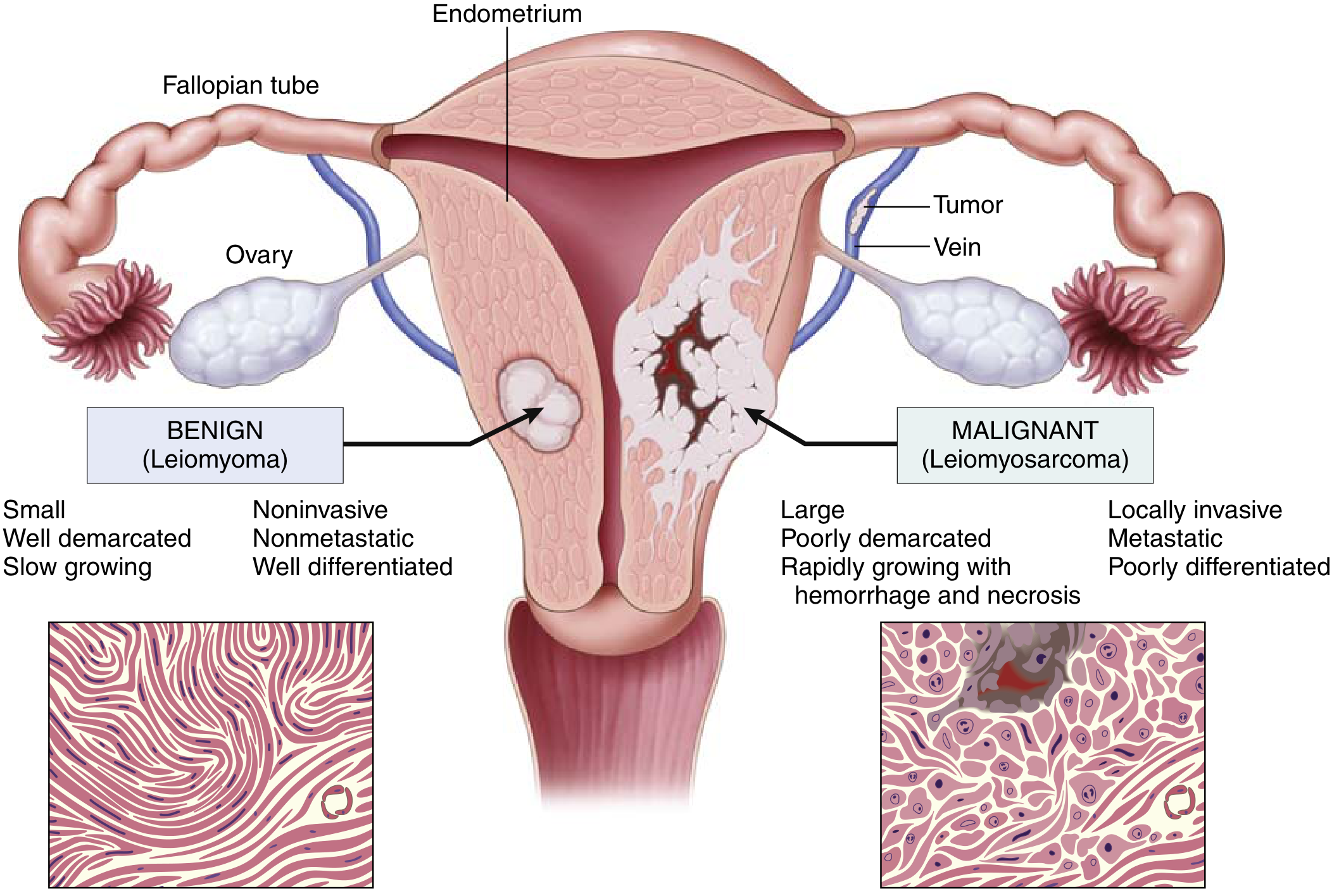
Benign vs malignant tumors
Benign vs Malignant Tumors - Pathology Exam Guide
The Classic Comparison Diagram
The 4 Key Distinguishing Features (Table 7.2 - Robbins Cotran)
| Feature | Benign | Malignant |
|---|---|---|
| Differentiation / Anaplasia | Well differentiated; structure typical of tissue of origin | Some lack of differentiation (anaplasia); structure often deranged |
| Rate of Growth | Usually slow and progressive; may regress; mitoses rare and normal | Erratic, may be slow to rapid; mitoses may be numerous and abnormal |
| Local Invasion | Cohesive, expansile, well-demarcated masses; do NOT invade surrounding tissue | Locally invasive; infiltrate surrounding tissue; no clean margin |
| Metastasis | Absent | Frequent; more likely with large, undifferentiated tumors |
1. Differentiation & Anaplasia
-
Benign tumors are almost always well differentiated
- A lipoma looks like normal adipocytes; a chondroma looks like normal cartilage cells
- Mitoses are rare and look normal
- Retain normal functions (e.g., endocrine tumors still secrete hormones)
-
Malignant tumors range from well-differentiated to completely anaplastic (undifferentiated)
- Anaplasia literally means "backward formation" - loss of structural and functional differentiation
- Well-differentiated cancers (e.g., thyroid follicular carcinoma) may look almost normal - their malignancy is betrayed only by invasion or metastasis
- Poorly differentiated cancers show obvious morphologic abnormalities
Morphologic hallmarks of malignant cells (anaplastic features):
| Feature | Description |
|---|---|
| Pleomorphism | Variation in cell and nuclear size/shape |
| Hyperchromatic nuclei | Dark-staining; coarsely clumped chromatin at nuclear membrane |
| High N:C ratio | Nuclear-to-cytoplasm ratio approaches 1:1 (normal is 1:4 to 1:6) |
| Prominent nucleoli | Abnormally large nucleoli |
| Atypical mitoses | Bizarre mitotic figures (tripolar spindles, etc.) - key indicator of malignancy |
| Loss of polarity | Cells grow in disorganized sheets, lose normal orientation |
| Tumor giant cells | Huge cells with one large or two hyperchromatic nuclei |
| Areas of necrosis | Due to rapid growth outpacing vascular supply |
Exam tip: Atypical (bizarre) mitotic figures are more reliable indicators of malignancy than merely increased mitoses, since normal rapidly proliferating tissues also have many mitoses.
2. Rate of Growth
- Benign tumors grow slowly and progressively; some may come to a standstill or even regress
- Malignant tumors generally grow faster but rate is variable - growth rate alone is not a reliable discriminator
- Rapidly growing tumors often develop central ischemic necrosis because the vascular stroma cannot keep up
3. Local Invasion
-
Benign: Grow as cohesive, expansile masses. They compress surrounding tissue, forming a fibrous capsule (e.g., fibroadenoma of the breast). The capsule makes them:
- Discrete and moveable ("nonfixed")
- Easily surgically excised (enucleation)
-
Malignant: Lack well-defined capsules. They infiltrate and destroy surrounding tissue with "crab-like" extensions. Surgeons must remove a wide margin of normal tissue around them. Pathologists check for clean surgical margins.
Important exceptions:
- Some benign tumors have no capsule (e.g., uterine leiomyomas have a compressed zone but no true capsule; hemangiomas are neither encapsulated nor well-defined)
- Some malignant tumors may appear encapsulated but show microscopic invasion at the edges (e.g., follicular carcinoma of the thyroid)
- Lack of capsule does NOT automatically = malignant
- Malignant tumors may also induce desmoplasia - a dense, fibrous stromal reaction making the tumor hard ("scirrhous" tumors), classically seen in breast carcinoma
4. Metastasis
- Definitive hallmark of malignancy - benign tumors NEVER metastasize
- ~30% of newly diagnosed solid tumors already have clinically evident metastases; another ~20% have occult metastases
Three pathways of spread:
| Pathway | Details | Common Examples |
|---|---|---|
| Lymphatic spread | Most common for carcinomas; goes to regional lymph nodes first | Breast, lung, colon |
| Hematogenous spread | Veins invaded → liver and lungs are most common sites | Sarcomas; also carcinomas |
| Seeding of body cavities | Direct spread into peritoneal, pleural, pericardial cavities | Ovarian carcinoma → peritoneum ("pseudomyxoma peritonei") |
Exam tip: Basal cell carcinoma of the skin and most primary CNS tumors are locally invasive but rarely metastasize - proof that local invasion and metastasis are separable properties.
Dysplasia & Carcinoma In Situ (Related Concepts)
-
Dysplasia = disordered proliferation (not synonymous with cancer!)
- Features: cellular pleomorphism, hyperchromatic nuclei, increased abnormal mitoses, loss of normal maturation
- Mild-moderate dysplasia may regress if the inciting cause is removed
- Marks tissue at increased risk for cancer
-
Carcinoma in situ = severe dysplasia involving the entire thickness of epithelium but NOT breaking through the basement membrane - a preinvasive stage of cancer
Tumor Nomenclature (Table 6.1 - Robbins Basic Pathology)
| Tissue | Benign | Malignant |
|---|---|---|
| Fibrous tissue | Fibroma | Fibrosarcoma |
| Fat | Lipoma | Liposarcoma |
| Cartilage | Chondroma | Chondrosarcoma |
| Bone | Osteoma | Osteosarcoma |
| Smooth muscle | Leiomyoma | Leiomyosarcoma |
| Striated muscle | Rhabdomyoma | Rhabdomyosarcoma |
| Blood vessels | Hemangioma | Angiosarcoma |
| Squamous epithelium | Squamous cell papilloma | Squamous cell carcinoma |
| Glandular epithelium | Adenoma | Adenocarcinoma |
| Melanocytes | Nevus | Melanoma |
Rule: Benign mesenchymal tumors = "-oma". Malignant mesenchymal = "-sarcoma". Malignant epithelial = "carcinoma". Exceptions exist (lymphoma, melanoma, hepatoma are all malignant despite the "-oma" suffix).
Key Concepts Summary (for quick recall)
- Three reliable distinguishing features: differentiation/anaplasia, local invasion, metastasis (not growth rate alone)
- Metastasis = only in malignant tumors - this is the most definitive sign
- Invasiveness = second most reliable sign after metastasis
- Anaplasia = marker of malignancy; involves pleomorphism, hyperchromatic nuclei, atypical mitoses, loss of polarity
- Benign tumors retain functions of parent cells; highly anaplastic tumors lose them (but may gain unexpected functions - e.g., ectopic hormone production in lung carcinoma)
- Dysplasia ≠ cancer but marks increased risk; carcinoma in situ = full-thickness but preinvasive
Difference between benign and malignant tumors table
Benign vs Malignant Tumors - Complete Comparison Table
| Feature | Benign | Malignant |
|---|---|---|
| Differentiation | Well differentiated; structure typical of tissue of origin | Variable - well to poorly differentiated (anaplastic); structure often deranged |
| Anaplasia | Absent | Present (in poorly differentiated tumors) |
| Rate of growth | Slow, progressive; may regress or plateau | Erratic - slow to rapid; generally faster |
| Mitoses | Rare; normal configuration | Numerous; atypical/bizarre mitotic figures |
| Pleomorphism | Absent (uniform cells) | Present - variation in cell and nuclear size/shape |
| Nuclear morphology | Normal N:C ratio (1:4-1:6) | High N:C ratio (approaches 1:1); hyperchromatic, irregular nuclei |
| Nucleoli | Normal | Prominent, abnormally large |
| Capsule | Usually present (fibrous capsule) | Absent - no well-defined margin |
| Border | Well demarcated, discrete, moveable | Poorly demarcated, fixed to surrounding tissue |
| Local invasion | Absent - grows as cohesive expansile mass | Present - infiltrates and destroys surrounding tissues |
| Metastasis | Never | Frequent - hallmark of malignancy |
| Necrosis / Hemorrhage | Absent (rare) | Common (due to rapid growth outpacing blood supply) |
| Desmoplasia | Absent | May be present (dense fibrous stromal reaction) |
| Effect on host | Usually local pressure effects only | Cachexia, paraneoplastic syndromes, death |
| Recurrence after surgery | Rare | More common |
| Prognosis | Generally excellent | Varies; often poor if metastasized |
| Cell polarity | Maintained | Lost (disorganized sheets of cells) |
| Function | Retains normal cell functions | May lose normal function; may acquire ectopic functions |
| Vascular invasion | Absent | Present |
Quick Memory Hook
"BENIGN = CALM" - Capsule, Alike (well differentiated), Low mitoses, Moveable (not fixed)"MALIGNANT = PAIN" - Pleomorphism, Atypical mitoses, Invasive, No capsule
Generate a visual infographic comparing these features
A clean medical education infographic titled "Benign vs Malignant Tumors" for pathology students. Split into two columns - left column in soft green for BENIGN tumors, right column in red for MALIGNANT tumors. Include a center divider with feature labels. Features to compare (listed vertically as rows): 1. Differentiation: Well differentiated | Poorly differentiated / Anaplastic 2. Growth Rate: Slow, may regress | Rapid, erratic 3. Capsule: Present, well encapsulated | Absent, no clear margin 4. Border: Well demarcated, moveable | Poorly demarcated, fixed 5. Local Invasion: Absent | Present - infiltrates tissue 6. Metastasis: NEVER | FREQUENT - hallmark 7. Mitoses: Rare, normal | Numerous, atypical/bizarre 8. Necrosis: Absent | Common 9. Nuclear morphology: Normal N:C ratio | High N:C ratio, hyperchromatic 10. Recurrence: Rare | Common 11. Prognosis: Excellent | Poor if metastasized Include small microscopic cell illustrations in each column - a uniform round cell cluster for benign, and irregular pleomorphic cells with abnormal mitoses for malignant. Add a memory aid box at the bottom: BENIGN = CALM (Capsule, Alike, Low mitoses, Moveable) | MALIGNANT = PAIN (Pleomorphism, Atypical mitoses, Invasive, No capsule). Professional medical textbook style with clear icons and readable fonts.
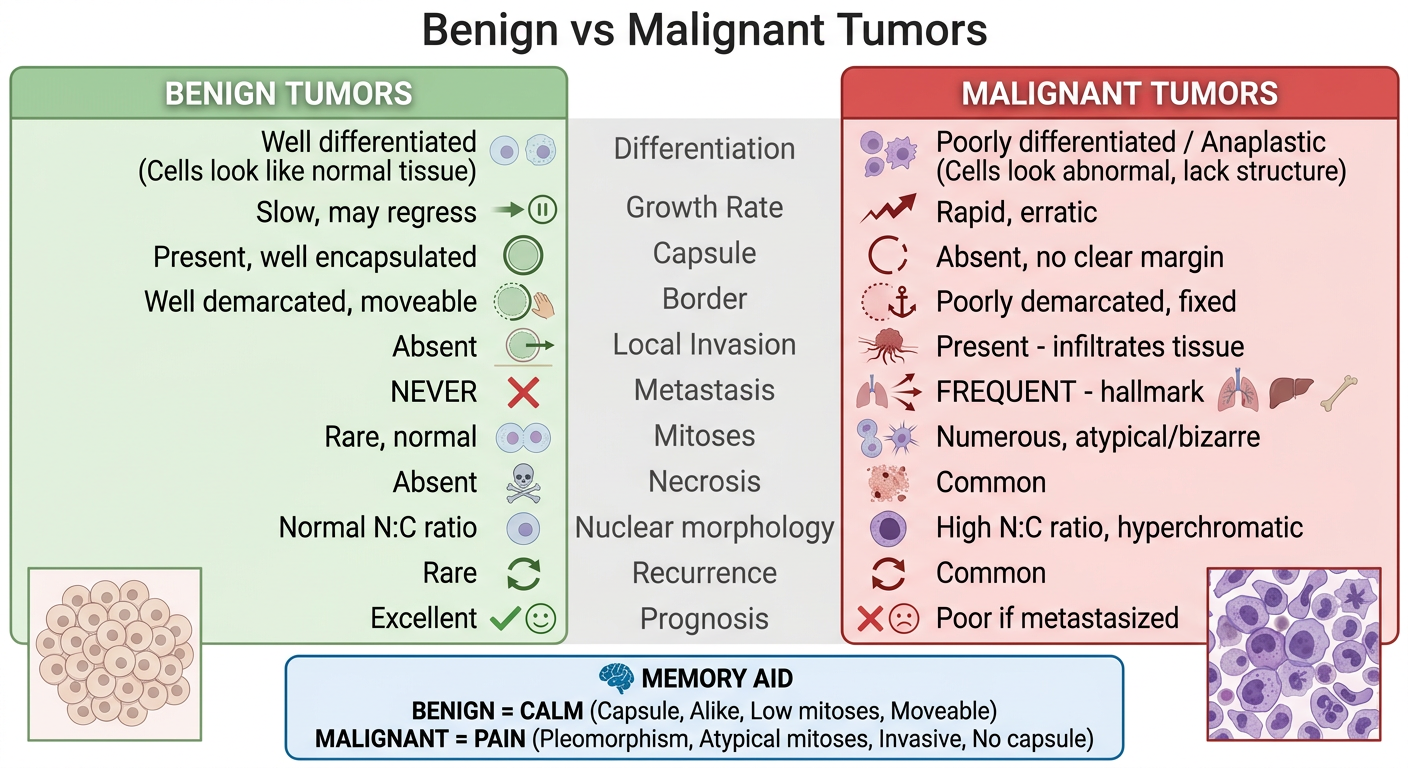
- Green (Benign) vs Red (Malignant) color coding for easy recall
- All 11 major features compared
- The CALM vs PAIN memory aid at the bottom