Hyperkalemia correction
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Searching PubMed
hyperkalemia treatment management
I now have all the information needed to give a comprehensive answer. Let me compile it.
Hyperkalemia: Correction & Management
Classification by Severity
| Severity | Serum K⁺ | Action |
|---|---|---|
| Mild | 5.5 - 6.0 mEq/L | Observe; eliminate exogenous K⁺ sources |
| Moderate | 6.1 - 6.9 mEq/L | Active shifting ± removal |
| Severe | ≥ 7.0 mEq/L | Immediate intervention; cardiac monitoring |
ECG Changes (Sequential with Rising K⁺)
The ECG below shows severe hyperkalemia with QRS widening merging into T waves and absent P waves:
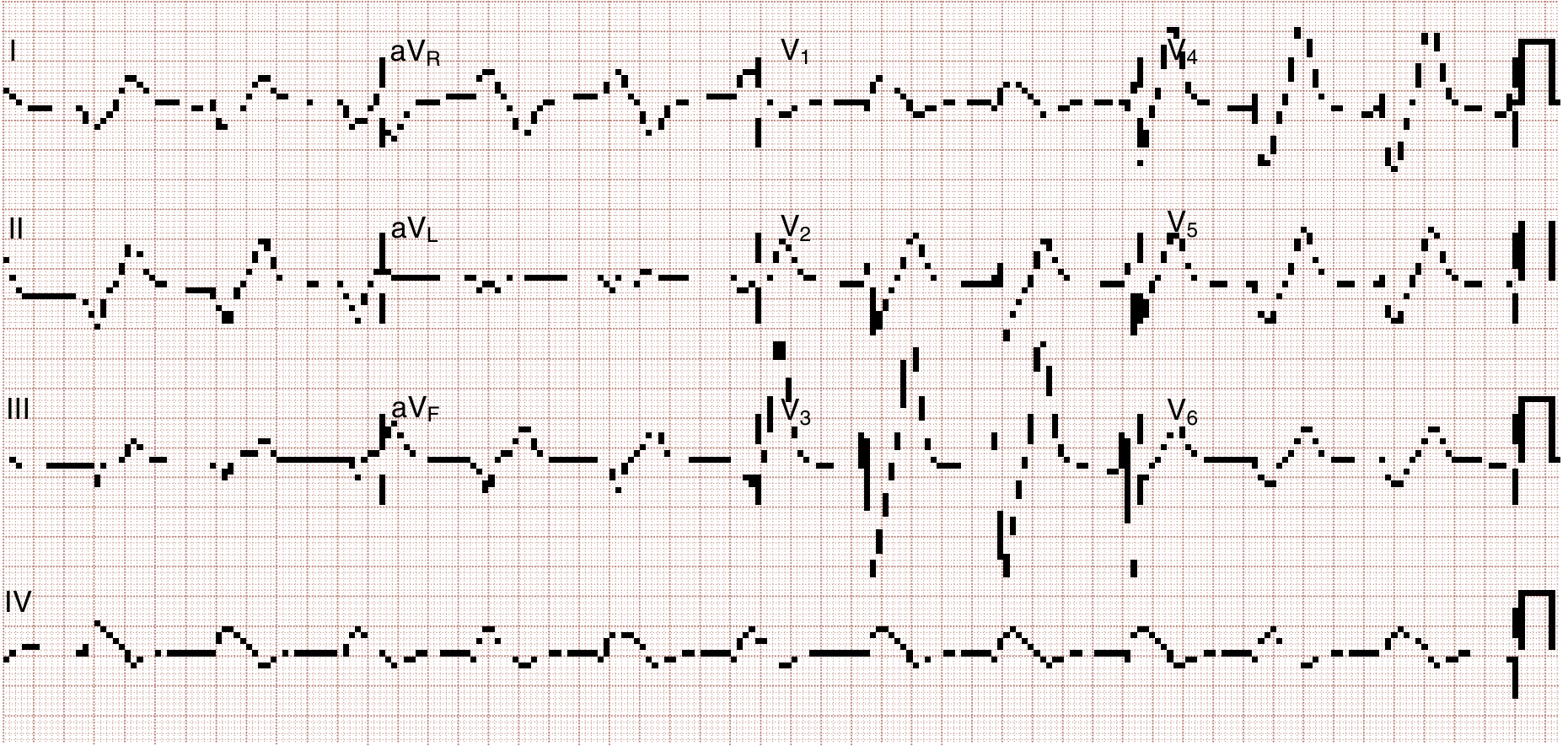
Progressive ECG changes:
- Peaked (tall, narrow, symmetric) T waves - K⁺ > 5.5-6.5 mEq/L
- Flattened P wave + prolonged PR interval - K⁺ > 6.5-7.5 mEq/L
- Wide QRS complex - K⁺ > 7.0-8.0 mEq/L
- Sine wave pattern (QRS merges with T) - impending VF/asystole
- Ventricular fibrillation / asystole
Note: ECG changes may be absent even with severe hyperkalemia - a normal ECG does not exclude the diagnosis. Hyperkalemia can also mimic Brugada pattern or cause atropine-resistant bradycardia.
Three-Step Treatment Approach
Step 1 - Cardiac Membrane Stabilization (Buys Time)
Calcium - acts within 1-3 minutes, lasts 30-60 minutes. Does NOT lower serum K⁺.
| Agent | Dose | Route | Notes |
|---|---|---|---|
| Calcium gluconate 10% | 10-30 mL IV over 2-3 min; repeat in 5 min if needed | Peripheral IV preferred | First choice; less tissue damage if extravasation |
| Calcium chloride 10% | 10 mL (1 g) IV | Central line preferred | Contains 3× more Ca²⁺ than gluconate; risk of tissue necrosis peripherally |
Mechanism: restores the depolarization threshold, narrows QRS, reduces myocyte excitability. Caution in digoxin toxicity - calcium can precipitate worsening toxicity.
Step 2 - Intracellular Potassium Shift (Temporary; lowers K⁺ by 0.6-1.5 mEq/L)
| Agent | Dose | Onset | Duration | Effect | Notes |
|---|---|---|---|---|---|
| Regular insulin + glucose | Insulin 10 units IV + D50W 1 ampule (or D10W if normoglycemic) | < 15 min | 4-6 h | ↓ 0.6 mEq/L | Most reliable agent; stimulates Na⁺/K⁺-ATPase. Monitor glucose for hours post-therapy |
| Nebulized albuterol | 10-20 mg (adults); weight-based in children | 15-30 min | 2+ h | ↓ 0.5-1.0 mEq/L | Stimulates Na⁺/K⁺-ATPase; additive with insulin (combo lowers ~1.2 mEq/L) |
| Sodium bicarbonate | 1-2 mEq/kg IV | 15-30 min | 1-2 h | Variable | Effective ONLY in acidotic patients; no benefit in non-acidotic hyperkalemia. Risk: volume overload, hypocalcemic tetany/seizures - use cautiously in renal failure |
| IV normal saline | Few hundred mL | Moderate | Short | Modest | Stimulates Na⁺/K⁺-ATPase pump; judiciously in anuric patients |
Step 3 - Potassium Removal from the Body (Definitive)
| Method | Rate of K⁺ Removal | Notes |
|---|---|---|
| Hemodialysis | ↓ ~1 mEq/L in first hour, another 1 mEq/L over next 2 hours | Only reliable, experimentally proven method. First choice in life-threatening hyperkalemia with renal failure |
| Furosemide | Variable | Use in patients with intact renal function (e.g., rhabdomyolysis, tumor lysis). No RCTs in acute emergency setting |
| Sodium polystyrene sulfonate (Kayexalate) | Slow (hours) | No longer considered effective or safe within first 4 hours. Risk of intestinal necrosis, especially with sorbitol |
| Patiromer | Slower onset (hours-days) | Newer non-absorbable cation exchanger; useful for chronic/subacute management in CKD + RAAS therapy. Not evaluated in acute hyperkalemia |
| Sodium zirconium cyclosilicate (SZC) | Onset within 1 hour reported | Newer agent; promising for subacute but limited data in acute emergency |
| Peritoneal dialysis | Slower than HD | Alternative when HD unavailable |
Special Situations
- Renal failure (AKI/CKD): K⁺ rises 0.3-0.5 mEq/L per day in oliguric patients - faster in catabolism, sepsis, acidosis, or rhabdomyolysis. Hemodialysis is the cornerstone of definitive therapy. Succinylcholine use is relatively contraindicated.
- Cardiac arrest with suspected hyperkalemia: Treat empirically while resuscitation continues.
- Digoxin toxicity: Avoid calcium (may worsen toxicity); consider digoxin-specific Fab antibodies.
- Metabolic acidosis: Sodium bicarbonate is useful here; correct acidosis to drive K⁺ intracellularly.
- Pseudohyperkalemia: Exclude hemolysis, excessive fist-clenching, thrombocytosis, leukocytosis - confirm with repeat sample and correlate with ECG.
Causes to Treat Simultaneously (Common)
- Renal failure (AKI/CKD) - most common
- Drugs: ACE inhibitors, ARBs, K⁺-sparing diuretics, NSAIDs, heparin, beta-blockers, digoxin, succinylcholine, trimethoprim
- Adrenal insufficiency / Addison's disease / Type 4 RTA
- Cell death: rhabdomyolysis, tumor lysis, hemolysis, burns
- Acidosis (non-anion gap metabolic or respiratory)
Key Points
- Always obtain an ECG immediately - do not wait for labs when hyperkalemia is suspected.
- The three steps must overlap: stabilize membrane first, then shift K⁺, then remove K⁺.
- All shifting measures are temporary (1-6 hours) - definitive removal is essential.
- Calcium gluconate and insulin/glucose are the workhorses of acute management.
- Bicarbonate's role is limited to acidotic patients only.
- A 2025 meta-analysis on novel K⁺ binders (PMID 40542996) confirms patiromer and SZC are effective for chronic management in CKD/heart failure patients on RAAS inhibitors, but are not replacements for acute-phase treatment.
Sources: Rosen's Emergency Medicine, 10e; Schwartz's Principles of Surgery, 11e; Harrison's Principles of Internal Medicine, 22e; Morgan & Mikhail's Clinical Anesthesiology, 7e; Barash's Clinical Anesthesia, 9e.
This is a shared conversation. Sign in to Orris to start your own chat.