Post surgical management of glaucoma and complications of glaucoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
glaucoma surgery postoperative management complications
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the comprehensive information needed. Let me compile a thorough, well-organized answer.
Post-Surgical Management of Glaucoma and Complications of Glaucoma Surgery
Source: The Wills Eye Manual - Office and Emergency Room Diagnosis and Treatment of Eye Disease
Overview
Post-operative management after glaucoma filtering surgery (trabeculectomy, tube-shunt implants) centers on monitoring intraocular pressure (IOP), the filtering bleb, and the anterior chamber, while watching for a distinct set of complications that can be broadly grouped by IOP level and anatomical findings.
Differential Diagnosis Framework
The table below summarizes the key distinguishing features of post-operative complications based on IOP, anterior chamber depth, and bleb appearance:
| Diagnosis | IOP | Anterior Chamber | Iris Bombé | Pain | Bleb |
|---|---|---|---|---|---|
| Inflammation | Variable, may be low | Deep | No | Possible | Varies |
| Hyphema | Mildly to moderately elevated | Varies | Not early | Possible | Varies |
| Failure to filter | Moderately elevated | Deep | No | Possible | Flat |
| Aqueous misdirection / Malignant glaucoma | Early moderate → Late markedly elevated | Diffusely shallow, Grade 2 or 3 | No | Moderate | Flat |
| Suprachoroidal hemorrhage | Early markedly elevated → Late mild-moderate | Grade 1-2 | No | Excruciating | Flat |
| Pupillary block | Early moderate, may become markedly elevated | Grade 1-3 | Yes | Possible if high IOP | None |
| Serous choroidal detachment | Low | Shallow/flat | No | Minimal | Flat |
| Wound leak / Overfiltration | Low | Shallow/flat | No | Minimal | Large/diffuse |
A. INCREASED POSTOPERATIVE IOP AFTER FILTERING PROCEDURE
Grading of Anterior Chamber Shallowing
- Grade 1: Peripheral iris-cornea contact
- Grade 2: Entire iris in contact with cornea
- Grade 3: Lens (or lens implant or vitreous face) to corneal contact
Treatment (Step-by-Step)
-
Gonioscopy first - essential before starting any treatment to determine the cause.
-
Bleb not formed, deep anterior chamber: Apply light ocular pressure (Carlo Traverso Maneuver) to see if the sclerostomy will drain. In fornix-based procedures, take care not to disrupt the limbal wound.If the sclerostomy is blocked with iris, any globe pressure is contraindicated due to risk of further iris incarceration.
-
Laser suture lysis or removal of releasable sutures - may be indicated to increase filtration around the scleral flap.
-
Sclerostomy obstruction management:
- Iris: Topical pilocarpine or slow intracameral acetylcholine (within 2-3 days). If failed: transcorneal mechanical iris retraction, argon laser iridoplasty.
- Vitreous: YAG laser photodisruption of the sclerostomy.
- Blood or fibrin: Time, or intracameral tissue plasminogen activator (tPA, 10 µg).
-
Tube (glaucoma drainage device) obstruction: Remove stent suture or lyse ligature suture. Use caution - IOP may drop dramatically if tube opened before postoperative month 1.
-
Suprachoroidal effusion/hemorrhage:
- Mild IOP rise + formed chamber: observation + medical management.
- Persistent chamber flattening, corneal-lenticular touch, chronic retinal fold apposition, intolerable pain: surgical drainage.
- Delay drainage at least 10 days in cases of suprachoroidal hemorrhage.
-
If above measures fail: reoperation.
B. LOW POSTOPERATIVE IOP AFTER FILTERING PROCEDURE (Hypotony)
- IOP <7-8 mmHg: Risk of flat anterior chamber, choroidal detachment, suprachoroidal hemorrhage.
- IOP <4 mmHg: Risk of macular hypotony maculopathy and corneal edema.
Differential Diagnosis and Treatment by Bleb/Chamber Status
1. Large bleb + deep chamber (Overfiltration)
- A large bleb in the first few weeks is often desirable after trabeculectomy.
- Treat if: still present 6-8 weeks post-op, symptomatic, IOP decreasing, or anterior chamber shallowing.
- Treatment: topical atropine 1% b.i.d., intracameral viscoelastic, possibly autologous blood injection into the bleb.
- Observe if IOP is low but stable, vision stable, and anterior chamber deep.
2. Large bleb + flat chamber (Grade I or II)
- Cycloplegics (atropine 1% t.i.d.) and careful observation.
- If chamber becomes more shallow, IOP decreases as bleb flattens, or choroidal detachment develops: reform anterior chamber with viscoelastic.
3. No bleb + flat chamber
- Perform Seidel test to check for wound leak.
- If positive: aqueous suppressants, antibiotic ointment, bandage contact lens, patching, or surgical closure.
- If negative: look for cyclodialysis cleft (gonioscopy + UBM) or serous choroidal detachments.
- Cyclodialysis cleft: cycloplegics, laser/cryotherapy to close, or surgical closure.
- Serous choroidal detachment: usually observed, resolves as IOP normalizes.
4. Grade III flat chamber - SURGICAL EMERGENCY
- Prompt correction required.
- Office-based: reformation with viscoelastic.
- Surgical: drainage of choroidal detachment, reformation of anterior chamber ± revision of scleral flap/tube, or cataract extraction ± other procedures.
C. BLEB INFECTION (BLEBITIS) - Section 9.19
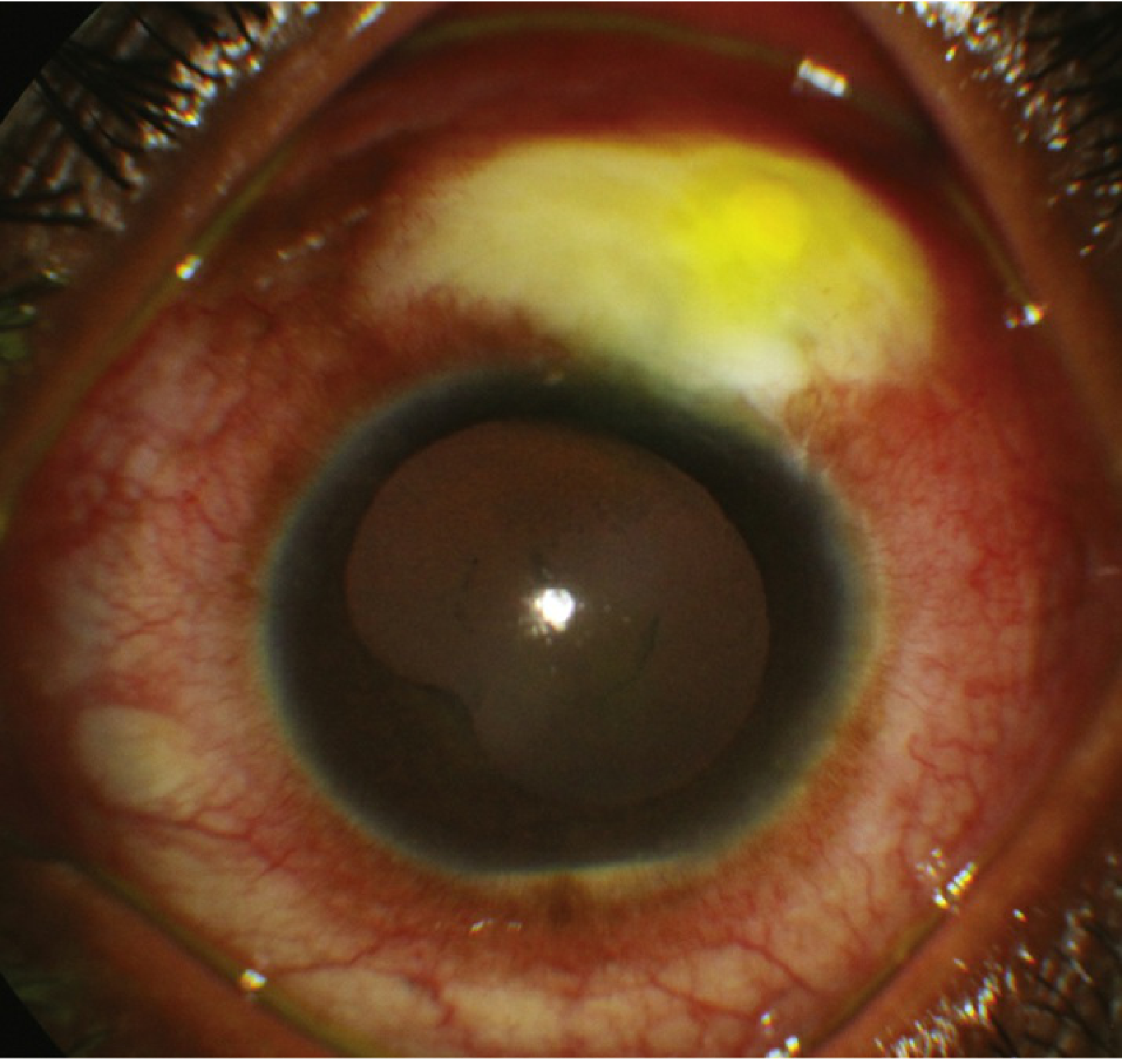
Blebitis: milky bleb with purulent material and intense conjunctival injection.
Definition
Infection of a filtering bleb. Can occur any time after filtering surgery (days to years). Higher incidence with antimetabolite use, multiple surgeries, flat anterior chamber, and wound leak.
Grading
| Grade | Description |
|---|---|
| Grade 1 (mild) | Bleb infection only - hyperemia or purulence, no AC or vitreous involvement |
| Grade 2 (moderate) | Bleb infection + anterior chamber inflammation, no vitreous involvement |
| Grade 3 (severe) | Bleb infection + anterior chamber + vitreous involvement = treat as endophthalmitis |
Signs
- Grade 1: Milky bleb with loss of translucency, microhypopyon in bleb loculations, frank purulent material, intense conjunctival injection. IOP usually unaffected.
- Grade 2: Grade 1 + AC cell/flare ± anterior chamber hypopyon; no vitreous inflammation.
- Grade 3: Grade 2 + vitreous involvement (same appearance as endophthalmitis but with bleb involvement).
Symptoms
Red eye and discharge early; later: aching pain, photophobia, decreased vision, mucous discharge.
Workup
- Slit lamp exam of bleb, anterior chamber, vitreous. Seidel test for bleb leak. Gonioscopy for microhypopyon.
- Culture bleb or anterior chamber tap for Grade 2. If Grade 3: treat as endophthalmitis.
- B-scan ultrasound to identify vitritis if visualization is difficult.
Common Organisms
- Early post-op: S. epidermidis, S. aureus, other Gram-positive organisms.
- Late (months-years): Streptococcus, Haemophilus influenzae, S. aureus, Moraxella, Pseudomonas, Serratia.
Treatment
Grade 1:
- Option A: Fortified cefazolin or vancomycin + fortified tobramycin or gentamicin, alternating every 30 minutes (first 24 hours). Loading dose: 1 drop each every 5 minutes x 4 doses.
- Option B: Fluoroquinolones q1h around the clock after a loading dose.
- Reevaluate at 6-12 hours and 12-24 hours. Must not be getting worse.
- May treat concurrent bleb leak with aqueous suppressants and cycloplegia.
Grade 2:
- Same as Grade 1, plus cycloplegics.
- Consider oral fluoroquinolones (e.g., ciprofloxacin 500 mg p.o. b.i.d. or moxifloxacin 400 mg daily).
- More careful, frequent monitoring.
Grade 3:
- Treat as endophthalmitis. Preference for early pars plana vitrectomy - bleb-associated endophthalmitis is more fulminant than post-cataract endophthalmitis.
Follow-up: Daily until infection is resolving. Hospital admission may be indicated.
D. COMPLICATIONS OF ANTIMETABOLITES (5-Fluorouracil, Mitomycin C)
These agents are used to improve bleb survival but carry specific risks:
- Corneal epithelial defects
- Corneal edema
- Conjunctival wound leaks
- Bleb overfiltration
- Bleb rupture
- Scleral thinning and perforation
- Increased risk of blebitis (long-term)
E. COMPLICATIONS OF CYCLODESTRUCTIVE PROCEDURES
(Cyclodiode laser, cyclocryotherapy)
- Pain, uveitis, decreased vision
- Cataract
- Hypotony
- Scleral thinning
- Choroidal effusion
- Suprachoroidal hemorrhage
- Sympathetic ophthalmia
- Phthisis bulbi (end-stage globe atrophy)
F. MISCELLANEOUS COMPLICATIONS OF FILTERING PROCEDURES
- Cataracts
- Corneal edema, corneal delle (drying/thinning adjacent to bleb)
- Endophthalmitis
- Uveitis
- Hyphema
- Bleb dysesthesia (discomfort/foreign body sensation)
G. COMPLICATIONS OF TUBE-SHUNT (DRAINAGE DEVICE) IMPLANTS
- Cataracts
- Corneal edema
- Endophthalmitis
- Hyphema
- Scleral perforation
- Diplopia
- Tube/implant erosion through conjunctiva
Key Post-Operative Monitoring Points
| Time Frame | Key Assessment |
|---|---|
| Day 1 | IOP, anterior chamber depth, bleb formation, wound integrity |
| Week 1-2 | Bleb morphology, suture lysis if needed, signs of infection |
| Week 6-8 | If large bleb persists with low IOP: consider treatment for overfiltration |
| Months-Years | Bleb-associated infection risk persists indefinitely; patient education essential |
- The Wills Eye Manual, Ch. 9.18-9.19, pp. 626-635
Recent evidence note: A 2024 systematic review and meta-analysis (PMID 39293570) found trabeculectomy and tube shunt implantation have comparable IOP outcomes in uveitic glaucoma, though tube shunts showed lower reoperation rates. A 2026 meta-analysis (PMID 41842588) on drainage device surgery in uveitic glaucoma confirms drainage devices remain effective but carries meaningful rates of hypotony and device-related complications, consistent with the management framework above.
This is a shared conversation. Sign in to Orris to start your own chat.