Fever in pediatrics
Reading File
Finding Sources
Finding Sources
Searching PubMed
"fever" AND "pediatric" AND "management"
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive content to deliver a thorough, well-structured response on pediatric fever. Let me compile the full answer.
Fever in Pediatrics
Fever is the most common complaint among pediatric patients presenting to the emergency department. Viruses cause the vast majority of childhood febrile illnesses and are generally self-limited. However, identifying the subset of children with serious bacterial infection (SBI) is the central clinical challenge.
Source: Rosen's Emergency Medicine - Concepts and Clinical Practice
Definition
- Fever = rectal temperature ≥ 38°C (100.4°F); some guidelines use ≥ 38.3°C
- High fever = ≥ 39°C (102.2°F)
- Rectal measurement is the standard in infants and young children
- Defervescence after acetaminophen does not reliably exclude bacteremia
Serious Bacterial Infection (SBI)
SBI = growth of pathogenic bacteria in a previously sterile site. Includes:
- UTI (most common cause of SBI at all pediatric ages)
- Bacteremia / sepsis
- Bacterial meningitis
- Pneumonia
- Osteomyelitis / septic arthritis
- Bacterial gastroenteritis
- Cellulitis
Age-Stratified Approach
1. Neonates (0-28 days)
- Highest risk group - immature immune system, incomplete vaccination, exposure to birthing-process pathogens (Group B Streptococcus, Chlamydia trachomatis, N. gonorrhoeae)
- Rate of SBI: 6-10% in febrile infants < 3 months
- Bacterial meningitis: ~3/1000 febrile infants < 3 months
- All febrile neonates require full septic workup and empirical antibiotics
Workup:
- CBC with differential
- Blood culture
- Urinalysis + urine culture (catheterization - not bag specimen)
- Lumbar puncture (CSF culture, cell count, glucose, protein)
- CXR if respiratory symptoms
Empirical antibiotic therapy:
- Ampicillin + gentamicin OR ampicillin + cefotaxime
- Covers Group B Strep, Listeria, gram-negatives
HSV empirical therapy (IV acyclovir) is indicated if:
- Maternal history of genital herpes
- Ill appearance with fever + seizure
- Cutaneous vesicles on exam
- Transaminitis or coagulopathy
Note: RSV and influenza do not reduce SBI risk in neonates < 28 days - a positive viral test does not change the workup in this age group.
2. Infants 1-3 Months (29-90 days)
- Immune function is improving but still immature
- Primary vaccination series begins at 2 months
- Risk stratification tools help guide management:
Rochester/Philadelphia/Boston Criteria are used to identify "low-risk" infants who may be managed as outpatients without antibiotics. Low-risk features include:
- Previously healthy, term infant
- Non-toxic appearance
- No focal bacterial infection on exam
- WBC 5,000-15,000/mm³
- Normal urinalysis
- Stool: WBC < 5/hpf if diarrhea present
- CSF: WBC < 10 cells/mm³
Management:
- Low-risk infants: may be discharged with close follow-up (24 hours) after blood culture and urinalysis; LP may be deferred
- High-risk or ill-appearing infants: full septic workup + admission + empirical antibiotics
3. Infants 3-36 Months
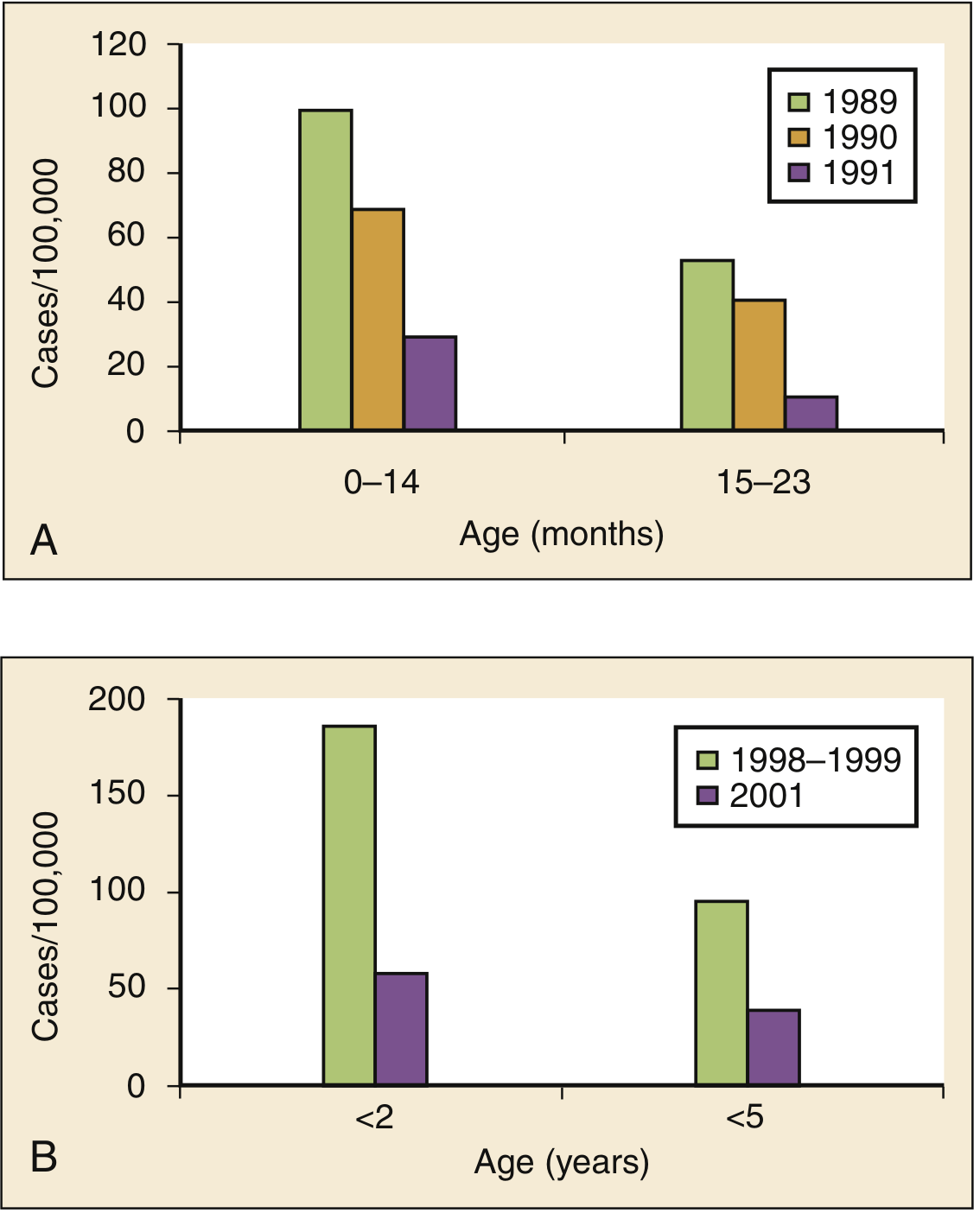
The post-vaccine era has dramatically changed this age group. Since introduction of PCV7 and PCV13:
- Invasive pneumococcal infections decreased >75% in children < 24 months
- Routine blood cultures for all febrile children in this age group are no longer recommended
Management algorithm for 3-36 month old febrile infants:
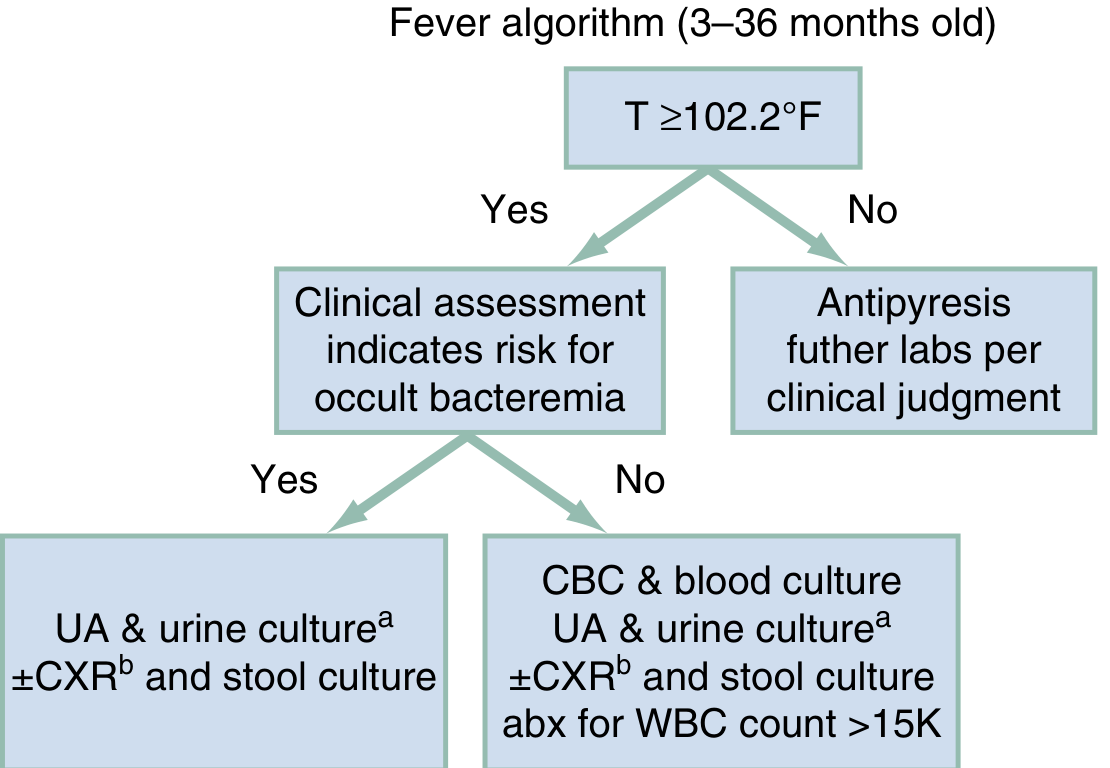
- T < 102.2°F: antipyresis + further labs per clinical judgment
- T ≥ 102.2°F + low clinical risk for occult bacteremia: UA + urine culture ± CXR ± stool culture
- T ≥ 102.2°F + higher risk: CBC + blood culture + UA + urine culture ± CXR; antibiotics if WBC > 15,000
Urine screening indications:
- Females < 24 months
- Circumcised males < 6 months
- Uncircumcised males < 12 months
- Bladder catheterization is the preferred method for non-toilet-trained infants (bag specimen has high false-positive rate but if negative, rules out UTI)
4. Children ≥ 3 Years to Adulthood
- Occult bacteremia risk decreases markedly
- Focal infections predominate: strep pharyngitis, pneumonia, otitis media, cellulitis, peritonsillar abscess (adolescents), septic arthritis
- Consider Mycoplasma pneumoniae in community-acquired pneumonia
- Community-acquired MRSA is increasing - consider in skin abscesses/pyogenic infections
- Management: incision and drainage + antibiotics (especially abscesses > 5 cm, cellulitis, or fever)
- Viral causes: EBV (infectious mononucleosis), influenza, RSV
Clinical Evaluation
History
- Duration of fever, localizing symptoms (headache/neck stiffness, ear pain, cough)
- Sick contacts, travel history
- Immunization status
- Prior antibiotic use (may mask meningitis findings)
- Birth history in young infants (gestational age, maternal infections)
- Rash history (roseola vs. meningococcemia, RMSF, toxic shock syndrome)
Physical Examination - "Traffic Light" Approach
Assess for toxicity: lethargy, poor perfusion, hypo/hyperventilation, cyanosis, petechiae/purpura
| Feature | Low Concern | High Concern |
|---|---|---|
| Color | Normal | Pale, mottled, ashen, cyanotic |
| Activity | Normal | Decreased, inconsolable |
| Hydration | Normal skin/eyes/mucosa | Dry mucosa, sunken eyes, poor turgor |
| Respirations | Normal | Tachypneic, grunting, retractions |
| Rash | None / viral exanthem | Petechiae, purpura (meningococcemia) |
Purpuric/petechial rash in a febrile child = meningococcemia until proven otherwise - immediate management required.
Differential Diagnosis
| Category | Examples |
|---|---|
| Viral | RSV, influenza, rhinovirus, adenovirus, EBV, roseola (HHV-6), parainfluenza |
| Bacterial | UTI, bacteremia, meningitis, pneumonia, otitis media, strep pharyngitis, GBS (neonates) |
| HSV | Neonatal HSV (encephalitis, disseminated) |
| Autoimmune | Kawasaki disease, juvenile idiopathic arthritis, SLE |
| Other | Malignancy, CNS tumors (rare), drug fever, heat stroke |
Antipyretic Management
Goals: Improve patient comfort; does not alter disease course or prevent febrile seizures.
| Drug | Dose | Route | Notes |
|---|---|---|---|
| Acetaminophen | 15 mg/kg q4-6h | PO/PR | First-line; safe from birth |
| Ibuprofen | 10 mg/kg q6-8h | PO | Use ≥ 6 months; avoid in renal disease, dehydration |
- Aspirin is contraindicated in children with viral illness (Reye syndrome risk)
- Alternating acetaminophen and ibuprofen: A 2024 network meta-analysis (PMID: 39318339) showed short-term dual therapy has modest superiority for fever reduction vs. monotherapy, but clinical guidelines traditionally favor monotherapy for simplicity
- Tepid sponging may provide temporary comfort but does not substitute for antipyretics
Febrile Seizures
- Simple febrile seizure: generalized, < 15 minutes, occurs once in 24 hours in a child 6 months - 5 years with fever, no neurological deficits
- Complex febrile seizure: focal onset, > 15 minutes, recurs within 24 hours, or child has a neurological abnormality
- LP is indicated in complex febrile seizures or if meningitis is suspected
- Antipyretics do not prevent febrile seizures
Red Flags - Do Not Miss
| Finding | Concern |
|---|---|
| Petechiae / purpura | Meningococcemia, DIC |
| Bulging fontanelle | Meningitis (infants) |
| Nuchal rigidity / Kernig's / Brudzinski's | Bacterial meningitis |
| Strawberry tongue, conjunctivitis, rash, lip cracking | Kawasaki disease |
| Ill appearance / toxic-looking child | SBI, sepsis |
| Neonatal fever (< 28 days) | Always high-risk - treat empirically |
| Fever in immunocompromised child | Broad workup + urgent empirical antibiotics |
Disposition Summary
| Age | Action |
|---|---|
| < 28 days | Full septic workup + admission + empirical antibiotics |
| 29-90 days, low-risk | Blood culture + UA; may discharge with 24-hr follow-up |
| 29-90 days, high-risk | Full workup + admission |
| 3-36 months, non-toxic, vaccinated | UA/urine culture; selective blood work |
| 3-36 months, toxic or high WBC | Blood culture + antibiotics |
| > 3 years, non-toxic, focal source | Treat source; outpatient |
Sources:
- Rosen's Emergency Medicine - Pediatric Fever chapter (Nathan W. Mick), pp. 3151-3160
- 2024 Network Meta-Analysis on dual vs. mono antipyretic therapy - PMID 39318339 (Pediatrics, Oct 2024)
This is a shared conversation. Sign in to Orris to start your own chat.