Why CO isused for Dlco. What's the application of DLCO
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have all the information needed to give a thorough, well-cited answer.
Why CO is Used for DLCO
The Problem with Oxygen
To measure diffusing capacity, you need a gas whose uptake rate across the alveolar-capillary membrane can be accurately calculated. The formula is:
D = Gas uptake / (Alveolar partial pressure - Capillary partial pressure)
For oxygen, this is impossible to use clinically because the pulmonary capillary PO2 rises continuously as blood passes through the capillary - it cannot be accurately measured at any single moment. Therefore, Pc'O2 cannot be determined, making DLO2 unmeasurable in practice.
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 952
Why CO Solves This Problem
Carbon monoxide has two properties that make it ideal:
-
Extremely high affinity for hemoglobin - CO binds hemoglobin approximately 200-240 times more avidly than oxygen. This means that virtually all CO that crosses into the blood is immediately bound to hemoglobin and almost none remains dissolved as free CO in capillary plasma.
-
Near-zero back pressure - Because dissolved CO in capillary blood is essentially zero (Pc'CO ≈ 0), the driving pressure for CO diffusion equals the alveolar partial pressure alone:
DLCO = CO uptake / PACO
This makes the denominator fully measurable and the calculation straightforward.
- Barash Clinical Anesthesia, 9e, p. 1138
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 952
- Miller's Anesthesia, 10e, p. 1304
What DLCO Actually Measures
DLCO is not a single membrane property - it collectively reflects all factors affecting gas transfer across the alveolar-capillary interface:
| Factor | Effect on DLCO |
|---|---|
| Alveolar surface area | Reduced area → lower DLCO |
| Alveolar-capillary membrane thickness | Thickening → lower DLCO |
| Pulmonary capillary blood volume | Less blood → lower DLCO |
| Hemoglobin concentration | Anemia → lower DLCO |
| V/Q matching | Mismatch → lower DLCO |
| Body position | Supine → higher DLCO |
| Alveolar PCO2 | Elevated PCO2 → higher DLCO |
Normal resting DLCO (single-breath method): ~25 mL CO/min/mmHg. This can increase 2-3 times during exercise.
- Barash Clinical Anesthesia, 9e, p. 1138
How DLCO is Measured (Single-Breath Technique)
- Patient exhales fully to residual volume
- Rapidly inhales a gas mixture containing a known concentration of CO + an inert tracer gas (helium or methane) to total lung capacity
- Holds breath for 10 seconds - CO diffuses across the membrane and binds hemoglobin; tracer gas remains in alveolar space
- Exhales - the inert gas calculates alveolar volume (VA); CO concentration drop calculates CO uptake
- Goldman-Cecil Medicine, p. 868
Clinical Applications of DLCO
1. Differentiating Obstructive Lung Diseases
| Disease | DLCO | Reason |
|---|---|---|
| Emphysema | Markedly reduced | Destruction of alveolar walls and capillary bed; loss of surface area |
| Asthma | Normal (or mildly reduced) | Airway problem, parenchyma intact |
| Chronic bronchitis | Normal or mildly reduced | Airway secretions, not alveolar destruction |
DLCO distinguishing emphysema from asthma in an obstructed patient is one of its most practical clinical uses.
- Goldman-Cecil Medicine, p. 868 | Barash Clinical Anesthesia, 9e, p. 1138
2. Detecting and Monitoring Interstitial Lung Disease (ILD)
Reduced DLCO is one of the earliest functional abnormalities in ILD. Diseases include:
- Idiopathic pulmonary fibrosis
- Sarcoidosis
- Asbestosis
- Berylliosis
- Connective tissue disease-associated ILD (e.g., systemic sclerosis - DLCO is used as a monitoring marker in SSc)
- Oxygen toxicity, pulmonary edema
3. Identifying Pulmonary Vascular Disease
An isolated reduction in DLCO (with normal TLC, VC, FEV1) is a red flag for pulmonary vascular disease (e.g., pulmonary hypertension, pulmonary emboli). The vascular bed destruction reduces the available surface area for gas exchange.
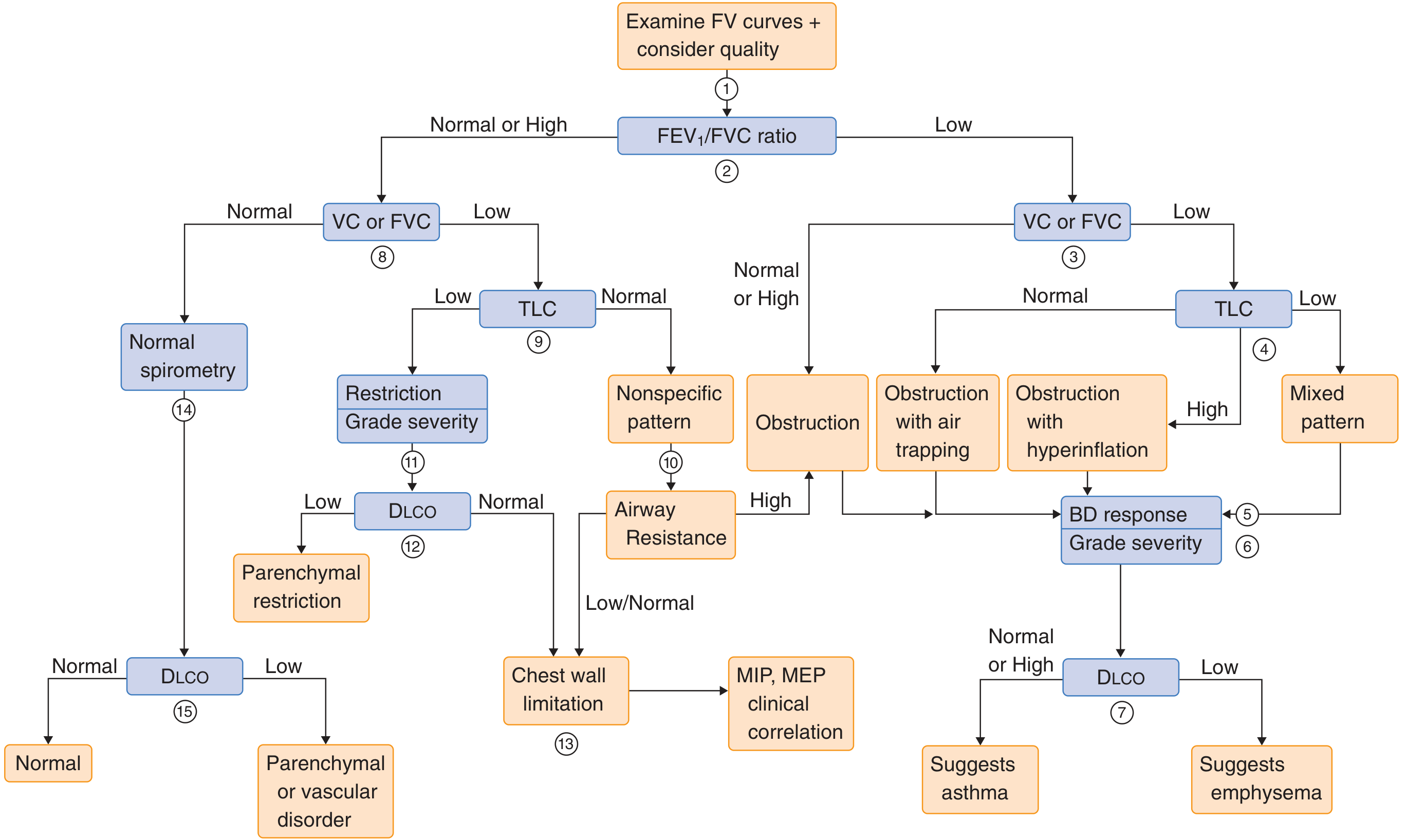
4. Distinguishing Parenchymal from Chest Wall Restriction
In a restrictive pattern (low TLC), DLCO helps separate:
- Low DLCO + restriction = parenchymal (ILD, sarcoid) disease
- Normal DLCO + restriction = chest wall / neuromuscular cause (scoliosis, obesity, neuromuscular disease)
See the algorithm below:
5. Pre-operative Risk Assessment
DLCO below 60% of predicted is associated with increased risk of postoperative pulmonary complications. It is an indication for further preoperative workup, often exercise testing (cardiopulmonary exercise testing / CPET).
- Miller's Anesthesia, 10e, p. 1304
Similarly, for thoracic surgery (lung resection), a predicted postoperative DLCO (ppo-DLCO) <40% predicts high perioperative risk.
- Barash Clinical Anesthesia, 9e, p. 1138
6. Exercise-Induced Dyspnoea
DLCO can increase 2-3x during exercise in normal individuals due to alveolar microvascular recruitment. Failure to augment DLCO with exercise is seen in pulmonary hypertension and other vascular diseases.
Summary Table
| Clinical Question | How DLCO Helps |
|---|---|
| Emphysema vs. Asthma | Low in emphysema, normal in asthma |
| Is ILD present? | Early reduction even before symptoms |
| Pulmonary hypertension screen | Isolated DLCO reduction |
| Parenchymal vs. chest wall restriction | Low vs. normal DLCO |
| Preoperative lung surgery | ppo-DLCO predicts complications |
| Anemia correction | Adjust DLCO for Hb (low Hb falsely lowers DLCO) |
Bottom line: CO is used precisely because its near-zero back pressure in the blood (due to extreme Hb affinity) makes the diffusion equation solvable. DLCO is one of the most clinically informative pulmonary function tests because it reflects the integrated health of the alveolar membrane, capillary bed, and ventilation-perfusion matching - not just airflow.
This is a shared conversation. Sign in to Orris to start your own chat.