tendinopathy of leg, treatment and symtoms
Reading File
Finding Sources
Searching PubMed
"tendinopathy" AND "treatment"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of tendinopathy of the leg based on multiple authoritative textbooks.
Tendinopathy of the Leg
What is Tendinopathy?
"Tendinopathy" is an umbrella term covering tendinitis (implying inflammation), tendinosis (degenerative change without active inflammation), partial tears, and peritendinous pathology. Histopathology typically shows degenerative changes with few inflammatory cells, so "tendinopathy" is now the preferred clinical term. - ROSEN's Emergency Medicine, p. 2345
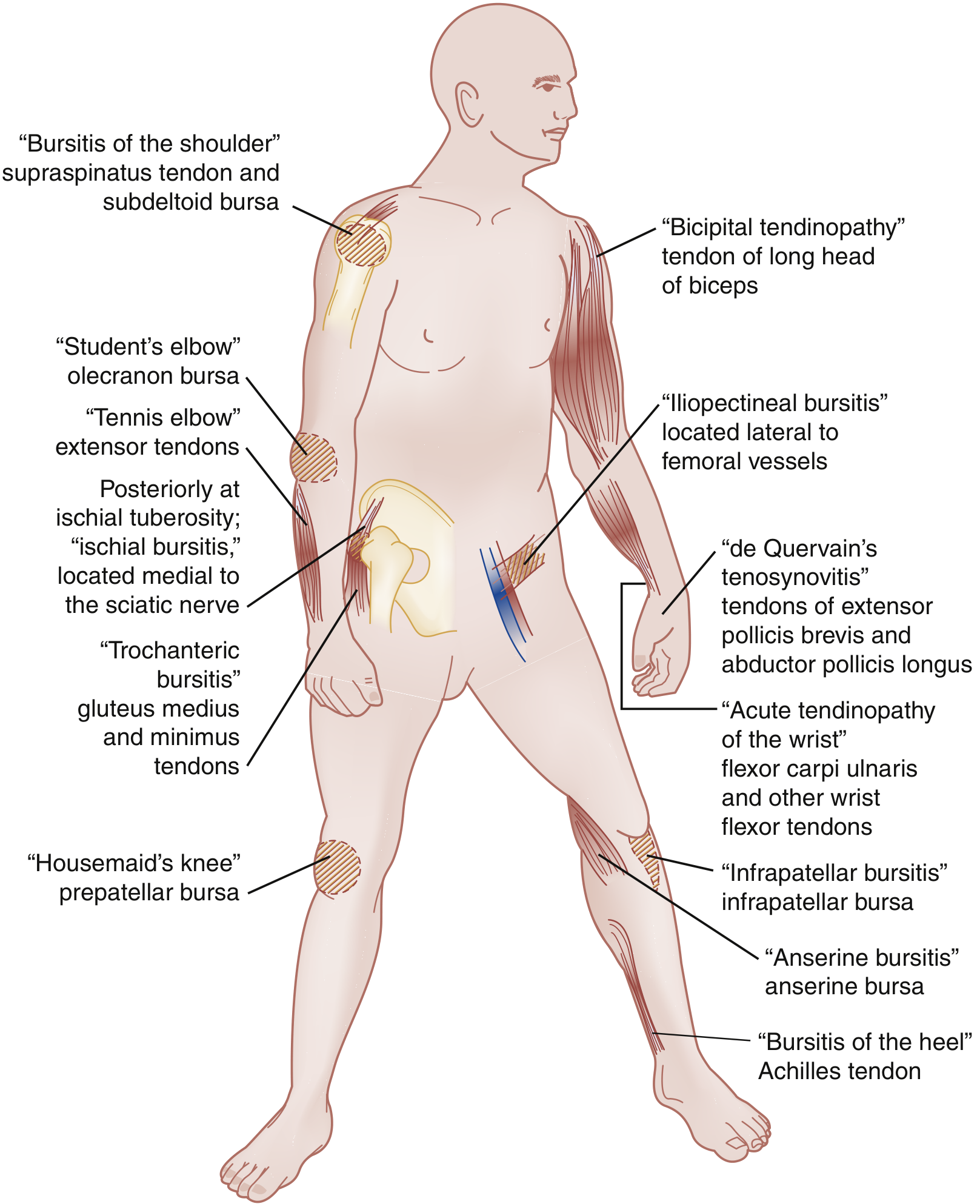
Common Leg Tendons Affected
The leg (below the knee to the ankle/foot) has several tendons prone to overuse:
| Tendon | Common Name | Mechanism |
|---|---|---|
| Achilles tendon | Achilles tendinopathy | Eccentric overload; running/jumping |
| Patellar tendon | Jumper's knee | Repetitive knee extension load |
| Tibialis posterior | Posterior tibial tendinopathy | Overpronation, flatfoot |
| Peroneal tendons | Peroneal tendinopathy | Ankle inversion stress |
Symptoms
Patients typically present with:
- Progressive, localized pain worsening after repetitive work- or sports-related activity - ROSEN's, p. 2345
- Morning stiffness that improves with gentle activity ("warm-up phenomenon")
- Tenderness to palpation directly over the affected tendon
- Swelling or thickening of the tendon; "wet crepitus" may be noted (fluid in peritenon)
- Reduced strength - assessed by single-leg heel raises or manual testing
- Pain with loading - push-off activities (stairs, hills, running, jumping) worsen Achilles symptoms - Textbook of Family Medicine 9e, p. 842
Achilles Tendinopathy - Specific Findings:
- Pain in the posterior distal lower leg or heel
- Palpable thickening or nodularity in the tendon mid-substance (2-6 cm above calcaneus)
- The Thompson test is essential to rule out complete rupture: patient prone, knee at 90°; squeeze gastrocnemius - absent plantarflexion = positive (ruptured)
Causes and Risk Factors
Intrinsic factors: Age, obesity, blood type O, tobacco use, lower limb malalignment, joint laxity, muscle weakness/imbalance
Extrinsic factors: Sudden increase in training load, poor equipment, repetitive occupational motions, awkward positions, environmental conditions - ROSEN's, p. 2346
Non-mechanical causes to be aware of: fluoroquinolone or statin use, systemic diseases (rheumatoid arthritis, gout, psoriatic arthritis), and infectious causes.
Diagnosis
- Clinical diagnosis in most cases
- Plain X-rays: Useful to detect calcific tendinopathy or bony abnormalities (e.g., Haglund deformity of calcaneus)
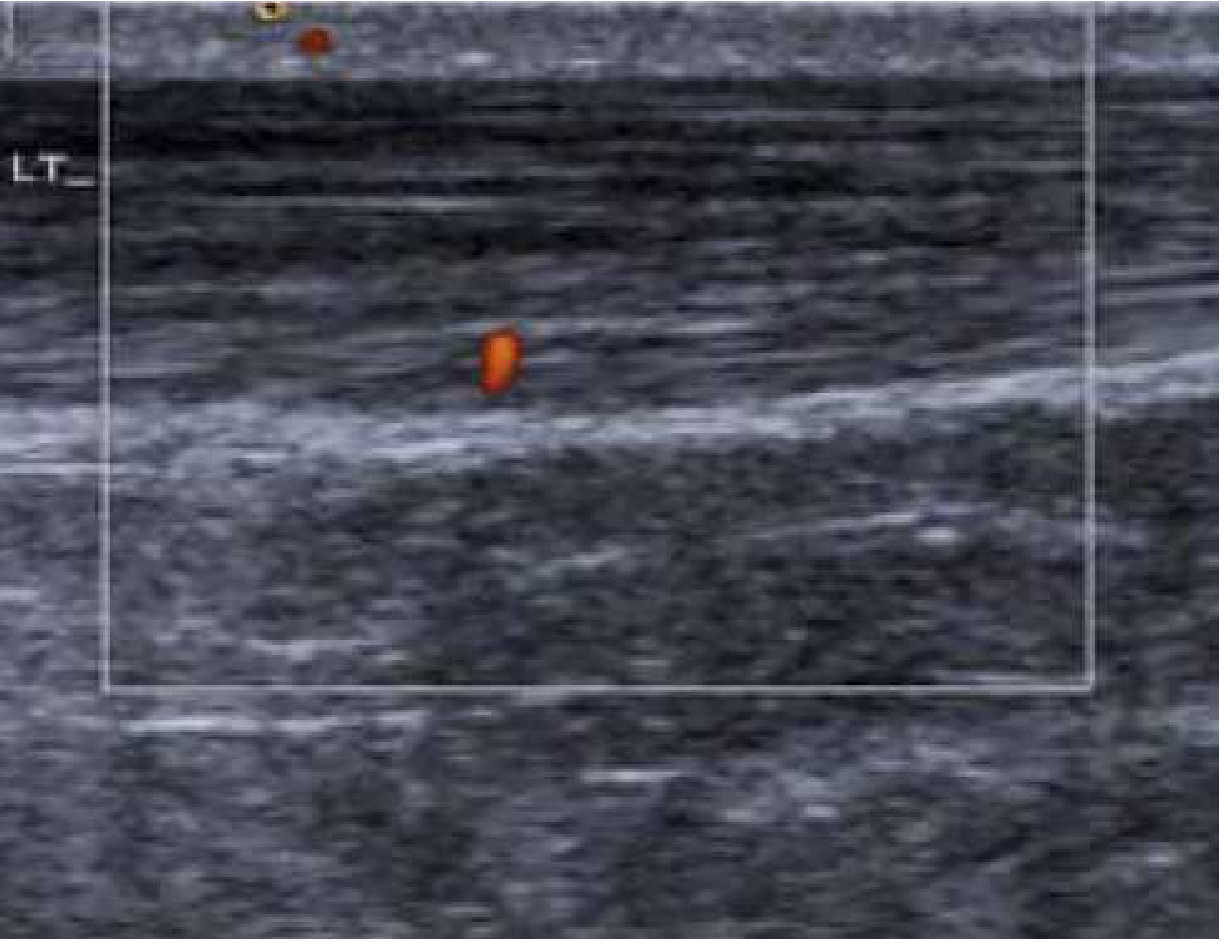
- Ultrasound (point-of-care): Preferred modality - can show focal thickening, loss of fibrillar echotexture, hypoechoic areas, peritendinous fluid, microruptures (100% sensitivity / 95% specificity in experienced hands) - ROSEN's, p. 2347
- MRI: High soft tissue resolution but sensitivity as low as 50%; used for complex/refractory cases
Treatment
1. Conservative (First Line - 6-12 weeks)
| Modality | Details |
|---|---|
| Activity modification | Reduce aggravating loads; complete rest is relatively contraindicated (leads to tendon deconditioning) |
| Cryotherapy (ice) | 20 min every few hours for the first 24-48 hours for pain relief |
| NSAIDs | Short course only (1 week preferred); helpful early for analgesia but impair long-term tendon healing - ROSEN's, p. 2348 |
| Eccentric exercise program | Gold standard for Achilles and patellar tendinopathy; promotes collagen remodeling - Family Medicine 9e, p. 843 |
| Stretching and proprioception | Part of a graduated rehabilitation program |
| Bracing/orthotics | Heel lifts for Achilles tendinopathy; supports for tibialis posterior |
| Nitroglycerin patches | Topical GTN patches for certain tendinopathies (evidence-based adjunct) |
2. Intermediate / Refractory Options
- Corticosteroid injections: Generally avoided for Achilles tendinopathy due to significant risk of tendon rupture. May be considered for other tendons with caution - Family Medicine 9e, p. 843
- Extracorporeal Shock Wave Therapy (ESWT): Evidence is mixed but used in recalcitrant cases
- Prolotherapy: Limited evidence; used in some chronic cases
- Platelet-Rich Plasma (PRP): Widely used; initiates a failed healing response in tendinosis. Note - for chronic Achilles tendinopathy, PRP has no benefit over saline injection per current evidence - Family Medicine 9e, p. 843
- Deep-friction massage / manual therapy
- Percutaneous tenotomy (dry needling): With or without autologous blood injection for degenerative tendons
3. Surgical Treatment
Reserved for:
- Complete tendon ruptures (e.g., Achilles rupture requiring primary repair)
- Cases failing 6+ months of conservative management
- Surgical debridement of degenerate tendon tissue - Family Medicine 9e
Prognosis
Recovery takes at least 6-12 weeks for most overuse tendinopathies. Recurrence is common - 49% of athletes with patellar tendinopathy and 40-50% with rotator cuff involvement report symptoms at 6-12 months. Patients should be counseled accordingly and referred to sports medicine or orthopedics for persistent symptoms. - ROSEN's Emergency Medicine, p. 2346
Recent Evidence Note: A 2025 Cochrane meta-analysis on exercise for patellar tendinopathy (PMID 40421598) confirms exercise therapy remains the cornerstone of treatment, which aligns with current textbook guidance.
This is a shared conversation. Sign in to Orris to start your own chat.