Malaria
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"malaria"[MeSH Terms] AND ("treatment" OR "management")
Reading File
Reading File
Finding Sources
Searching Images
malaria Plasmodium life cycle diagram
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content across pathophysiology, morphology, clinical features, diagnosis, and treatment. Let me compile the full overview.
Malaria — Comprehensive Overview
1. Epidemiology
Malaria is one of the world's most serious infectious diseases. The WHO estimated over 200 million cases and more than 600,000 deaths annually, with the vast majority caused by Plasmodium falciparum. It is endemic across sub-Saharan Africa, Asia, Oceania, Central and South America, and the Middle East. More than 41% of the global population lives in endemic areas. With widespread jet travel, cases now appear worldwide in returning travelers and immigrants. — Robbins & Kumar Basic Pathology; Rosen's Emergency Medicine
2. Causative Organisms
Five Plasmodium species infect humans, transmitted by the bite of female Anopheles mosquitoes (humans are the only natural reservoir):
| Species | Disease | Fever Cycle | Notes |
|---|---|---|---|
| P. falciparum | Tertian (falciparum) malaria | 48 h | Most lethal; multidrug resistance; causes cerebral malaria |
| P. vivax | Benign tertian | 48 h | Hypnozoite stage → relapse months–years later |
| P. ovale | Benign tertian | 48 h | Hypnozoite stage → relapse |
| P. malariae | Quartan malaria | 72 h | Mild; associated with nephrotic syndrome |
| P. knowlesi | Knowlesi malaria | 24 h | Zoonosis from macaques; Southeast Asia; occasionally severe |
Other routes of transmission include blood transfusions, contaminated needles/syringes, organ transplantation, maternal-fetal perinatal spread, and "airport malaria." — Rosen's Emergency Medicine, Medical Microbiology 9e
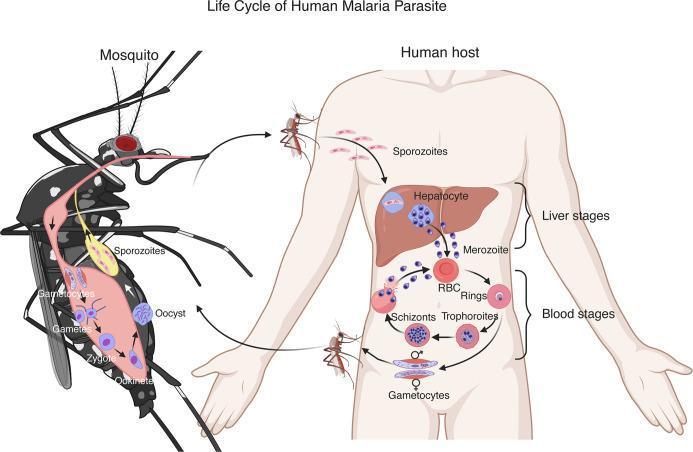
3. Life Cycle & Pathogenesis
The life cycle involves two hosts and is key to understanding both disease and drug targets:
Mosquito → Human (sporozoite stage)
- Infected Anopheles injects sporozoites into the bloodstream.
- Sporozoites (via thrombospondin-related adhesive protein and circumsporozoite protein) bind proteoglycans on hepatocytes and enter the liver → differentiate into merozoites (incubation 1–4 weeks).
- In P. vivax and P. ovale, some parasites become hypnozoites — dormant liver forms causing relapse.
Erythrocytic (blood) stage
- Merozoites bind sialylated glycophorin on RBCs and invaginate into a "digestive vacuole."
- Inside RBCs: merozoite → trophozoite → two paths:
- Some → gametocytes (sexual forms, ingested by next mosquito to continue the cycle)
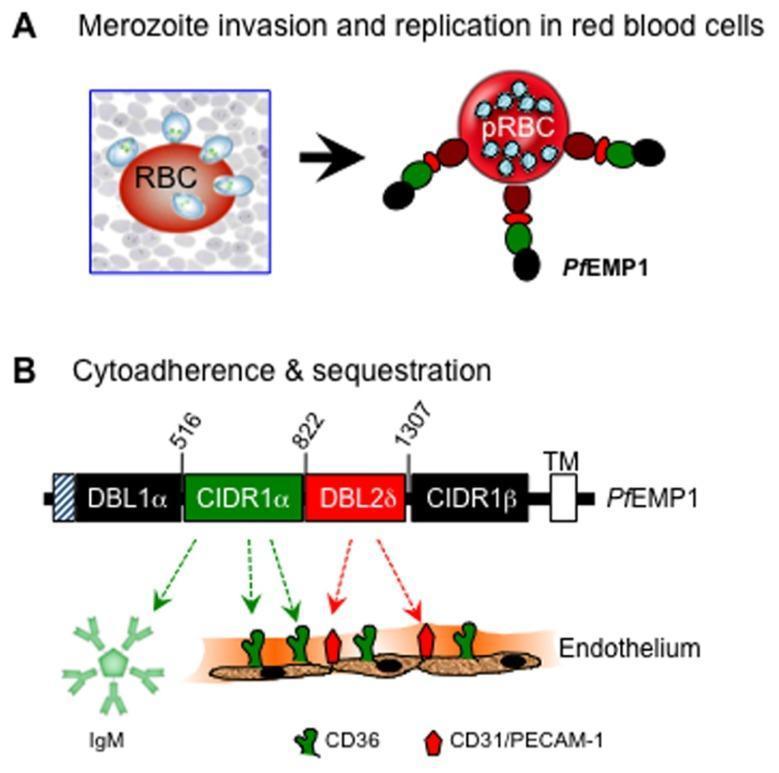
- Most → schizonts, which express PfEMP1 (P. falciparum erythrocyte membrane protein 1) — a key virulence factor inserting into knob-like protrusions on RBC surfaces. PfEMP1 binds ICAM-1, VCAM-1, and CD36 on vascular endothelium → cytoadherence and sequestration in capillary beds.
- Schizonts → merozoites → RBC lysis → another wave of infection.
In the mosquito
- Gametocytes mature into gametes → zygote → ookinete → oocyst → sporozoites migrate to salivary glands → transmitted to next human host.
— Robbins & Kumar Basic Pathology, pp. 392–393; Lippincott Illustrated Reviews: Pharmacology
4. Pathology & Morphology
- Hemolytic anemia: destruction of parasitized RBCs is the hallmark.
- Malarial pigment (hematin): brown hemoglobin-derived pigment released from ruptured RBCs; deposits in spleen, liver, lymph nodes, and bone marrow.
- Splenomegaly (often massive) and occasional hepatomegaly: from mononuclear phagocyte hyperplasia.
- Cerebral malaria (P. falciparum): small cerebral vessels become engorged and occluded by PfEMP1-mediated sequestration.
- Blackwater fever: rare complication of falciparum malaria — massive intravascular hemolysis → hemoglobinemia, hemoglobinuria, jaundice, renal failure.
- Peripheral blood smear: each species has a distinctive trophozoite morphology on Giemsa/Wright-stained thick smears.
— Robbins & Kumar Basic Pathology, p. 393
5. Clinical Features
- Classic presentation: headache and fatigue → episodic shaking chills, fever, and sweats
- Fever correlates with RBC lysis cycles:
- 48 h (P. vivax, P. ovale, P. falciparum); 72 h (P. malariae); 24 h (P. knowlesi)
- Fever may be continuous rather than periodic early in the illness (sensitivity >95% in low-endemicity areas along with headache)
- Severe/complicated falciparum malaria: persistent high fever, hyperparasitemia, organ dysfunction. Complications include:
- Cerebral malaria: seizures, coma, death within days
- Severe anemia
- Acute respiratory distress
- Hypoglycemia (parasite metabolic activity + quinine effect)
- Renal failure (blackwater fever)
- Metabolic acidosis
Risk factors for severe disease: longer travel duration, no or incomplete chemoprophylaxis, immunosuppression. — Rosen's Emergency Medicine; Lippincott Illustrated Reviews: Pharmacology
6. Diagnosis
Gold standard: Peripheral blood smear
- Thick and thin films stained with Giemsa or Wright stain
- Light microscopy identifies intraerythrocytic morphology and species
- Even if parasites are not visualized, treatment is indicated if malaria is strongly suspected
Rapid Diagnostic Test (RDT)
- Antigen-based (e.g., Alere BinaxNOW): detects all four species, ~$5/test
- Less sensitive than microscopy; positive RDTs should still be confirmed with smear for species ID and parasitemia quantification
PCR: highest sensitivity/specificity, useful in low-parasitemia or mixed infections
Always take a thorough travel history: dates, countries, rural vs. urban, prophylaxis adherence, insect precautions. — Rosen's Emergency Medicine, p. 2660
7. Treatment
Uncomplicated Malaria
| Situation | Treatment |
|---|---|
| Chloroquine-sensitive regions (Haiti, Dominican Republic, Central America N of Panama Canal, parts of Middle East) | Chloroquine phosphate (oral) |
| Chloroquine-resistant regions | Oral quinine + doxycycline or clindamycin; or proguanil-atovaquone (Malarone) |
| Uncomplicated (any region, approved in US) | Artemether-lumefantrine (Coartem) |
Severe/Complicated Falciparum Malaria
- IV artesunate — recommended first-line (in US, obtain via CDC Malaria Hotline: 770-488-7788 Mon–Fri, 770-488-7100 after hours)
- IV quinine or quinidine (not available in US) — alternative; requires cardiac monitoring (risk of severe hypoglycemia, hyponatremia)
- Supportive care: mechanical ventilation, anti-epileptics, correct hypoglycemia and acidosis
Preventing Relapse (P. vivax / P. ovale)
- Primaquine eliminates hepatic hypnozoites
- Contraindicated in G6PD deficiency (risk of severe hemolytic anemia) — test G6PD before use
- Tafenoquine is an alternative for relapse prevention
Cerebral Malaria
- IV quinine, quinidine, or artesunate + full supportive care
- Corticosteroids are not beneficial and may increase mortality in cerebral malaria
— Rosen's Emergency Medicine, pp. 2660–2669; Lippincott Illustrated Reviews: Pharmacology
8. Antimalarial Drugs — Mechanisms
| Drug | Mechanism | Key Notes |
|---|---|---|
| Chloroquine | Inhibits heme polymerization in parasite vacuole | Blood schizonticide; widespread resistance in P. falciparum |
| Artemisinin derivatives (artesunate, artemether) | Free radical generation via endoperoxide bridge cleavage by heme iron | First-line for multidrug-resistant P. falciparum; short half-life (not for prophylaxis); use as ACT (combo) |
| Quinine | Interferes with heme polymerization | Cinchonism (tinnitus, nausea, vertigo); cardiac monitoring needed IV |
| Mefloquine | Similar to quinine | Neuropsychiatric side effects; avoid with quinine/quinidine |
| Primaquine | Oxidant metabolites disrupt mitochondrial processes | Liver/hypnozoite stage; gametocytocidal; causes hemolysis in G6PD deficiency |
| Atovaquone-proguanil (Malarone) | Blocks mitochondrial electron transport + folate synthesis | Prophylaxis and treatment |
| Pyrimethamine | Inhibits dihydrofolate reductase → blocks folate synthesis | Used as pyrimethamine-sulfadoxine combo; resistance common; add artemisinin |
| Doxycycline | Protein synthesis inhibitor | Used adjunctively or for prophylaxis |
— Lippincott Illustrated Reviews: Pharmacology
9. Chemoprophylaxis
Travelers to endemic areas should receive prophylaxis matched to the region's resistance patterns:
- Atovaquone-proguanil: widely used; well tolerated; start 1–2 days before, end 7 days after travel
- Doxycycline: alternative; daily; photosensitivity risk
- Mefloquine: weekly; neuropsychiatric side effects; start 2 weeks before travel
- Chloroquine: only for sensitive regions; start 1–2 weeks before, end 4 weeks after
Additional prevention: insecticide-treated bed nets, mosquito repellents (DEET), protective clothing, removal of stagnant water (breeding sites).
10. Prevention & Vaccine
A vaccine containing sporozoite antigens (RTS,S/AS01 — Mosquirix) has been developed. While protection is partial, deployment is expected to prevent thousands of deaths from cerebral malaria in children. The WHO recommended it for broad pediatric use in sub-Saharan Africa in 2021, and the R21/Matrix-M vaccine (Oxford) has shown higher efficacy in trials. — Robbins & Kumar Basic Pathology
Sources: Robbins & Kumar Basic Pathology; Rosen's Emergency Medicine; Lippincott Illustrated Reviews: Pharmacology; Medical Microbiology 9e
This is a shared conversation. Sign in to Orris to start your own chat.